Langerhans Cell Histiocytosis: a Great Imitator Kayla St
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Regulation of Macrophage Development and Function in Peripheral Tissues
REVIEWS Regulation of macrophage development and function in peripheral tissues Yonit Lavin, Arthur Mortha, Adeeb Rahman and Miriam Merad Abstract | Macrophages are immune cells of haematopoietic origin that provide crucial innate immune defence and have tissue-specific functions in the regulation and maintenance of organ homeostasis. Recent studies of macrophage ontogeny, as well as transcriptional and epigenetic identity, have started to reveal the decisive role of the tissue stroma in the regulation of macrophage function. These findings suggest that most macrophages seed the tissues during embryonic development and functionally specialize in response to cytokines and metabolites that are released by the stroma and drive the expression of unique transcription factors. In this Review, we discuss how recent insights into macrophage ontogeny and macrophage–stroma interactions contribute to our understanding of the crosstalk that shapes macrophage function and the maintenance of organ integrity. Mononuclear phagocyte Macrophages are key components of the innate immune characterized the transcriptional and epigenetic pro- system system that reside in tissues, where they function as grammes of tissue-resident macrophages and revealed (MPS). A group of bone immune sentinels. They are uniquely equipped to sense the extent of diversity in these populations1,8. In addi- marrow-derived cells and respond to tissue invasion by infectious microorgan- tion to differences in ontogeny, locally derived tissue (monocytes, macrophages and isms and tissue -

The Best Diagnosis Is: A
DErmatopathology Diagnosis The best diagnosis is: a. eruptive xanthomacopy H&E, original magnification ×200. b. juvenile xanthogranuloma c. Langerhans cell histiocytosis d. reticulohistiocytomanot e. Rosai-Dorfman disease Do CUTIS H&E, original magnification ×600. PLEASE TURN TO PAGE 39 FOR DERMATOPATHOLOGY DIAGNOSIS DISCUSSION Alyssa Miceli, DO; Nathan Cleaver, DO; Amy Spizuoco, DO Dr. Miceli is from the College of Osteopathic Medicine, New York Institute of Technology, Old Westbury. Drs. Cleaver and Spizuoco are from Ackerman Academy of Dermatopathology, New York, New York. The authors report no conflict of interest. Correspondence: Amy Spizuoco, DO, Ackerman Academy of Dermatopathology, 145 E 32nd Street, 10th Floor, New York, NY 10016 ([email protected]). 16 CUTIS® WWW.CUTIS.COM Copyright Cutis 2015. No part of this publication may be reproduced, stored, or transmitted without the prior written permission of the Publisher. Dermatopathology Diagnosis Discussion rosai-Dorfman Disease osai-Dorfman disease (RDD), also known as negative staining for CD1a on immunohistochemis- sinus histiocytosis with massive lymphade- try. Lymphocytes and plasma cells often are admixed nopathy, is a rare benign histioproliferative with the Rosai-Dorfman cells, and neutrophils and R 1 4 disorder of unknown etiology. Clinically, it is most eosinophils also may be present in the infiltrate. frequently characterized by massive painless cervical The histologic hallmark of RDD is emperipolesis, lymphadenopathy with other systemic manifesta- a phenomenon whereby inflammatory cells such as tions, including fever, night sweats, and weight loss. lymphocytes and plasma cells reside intact within Accompanying laboratory findings include leukocyto- the cytoplasm of histiocytes (Figure 2).5 sis with neutrophilia, elevated erythrocyte sedimenta- The histologic differential diagnosis of cutaneous tion rate, and polyclonal hypergammaglobulinemia. -

WSC 10-11 Conf 7 Layout Master
The Armed Forces Institute of Pathology Department of Veterinary Pathology Conference Coordinator Matthew Wegner, DVM WEDNESDAY SLIDE CONFERENCE 2010-2011 Conference 7 29 September 2010 Conference Moderator: Thomas Lipscomb, DVM, Diplomate ACVP CASE I: 598-10 (AFIP 3165072). sometimes contain many PAS-positive granules which are thought to be phagocytic debris and possibly Signalment: 14-month-old , female, intact, Boxer dog phagocytized organisms that perhaps Boxers and (Canis familiaris). French bulldogs are not able to process due to a genetic lysosomal defect.1 In recent years, the condition has History: Intestine and colon biopsies were submitted been successfully treated with enrofloxacin2 and a new from a patient with chronic diarrhea. report indicates that this treatment correlates with eradication of intramucosal Escherichia coli, and the Gross Pathology: Not reported. few cases that don’t respond have an enrofloxacin- resistant strain of E. coli.3 Histopathologic Description: Colon: The small intestine is normal but the colonic submucosa is greatly The histiocytic influx is reportedly centered in the expanded by swollen, foamy/granular histiocytes that submucosa and into the deep mucosa and may expand occasionally contain a large clear vacuole. A few of through the muscular wall to the serosa and adjacent these histiocytes are in the deep mucosal lamina lymph nodes.1 Mucosal biopsies only may miss the propria as well, between the muscularis mucosa and lesions. Mucosal ulceration progresses with chronicity the crypts. Many scattered small lymphocytes with from superficial erosions to patchy ulcers that stop at plasma cells and neutrophils are also in the submucosa, the submucosa to only patchy intact islands of mucosa. -
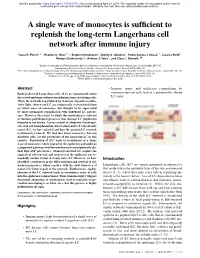
A Single Wave of Monocytes Is Sufficient to Replenish the Long-Term
bioRxiv preprint doi: https://doi.org/10.1101/617514; this version posted April 24, 2019. The copyright holder for this preprint (which was not certified by peer review) is the author/funder. All rights reserved. No reuse allowed without permission. A single wave of monocytes is sufficient to replenish the long-term Langerhans cell network after immune injury Ivana R. Ferrer1,2,a, Heather C. West1,2,a, Stephen Henderson2, Dmitry S. Ushakov3, Pedro Santos e Sousa1,2, Jessica Strid4, Ronjon Chakraverty1,2, Andrew J. Yates5, and Clare L. Bennett1,2 1Institute of Immunity and Transplantation, Division of Infection and Immunity, University College London, London NW3 2PF, UK 2Haematology, Division of Cancer Studies, University College London, London WC1E 6DD, UK. 3Peter Gorer Department of Immunobiology, School of Immunology and Microbial Sciences, King’s College London, New Hunt’s House, Newcomen St, London SE1 1UL, UK 4Division of Immunology and Inflammation, Imperial College London, Hammersmith campus, London W12 0NN, UK. 5Department of Pathology and Cell Biology, Columbia University Medical Center, New York, NY10032, USA. aThese authors contributed equally to this work Abstract • Immune injury and inefficient repopulation by Embryo-derived Langerhans cells (eLC) are maintained within monocyte-derived cells lead to a permanently altered the sealed epidermis without contribution from circulating cells. LC niche. When the network is perturbed by transient exposure to ultra- violet light, short-term LC are temporarily reconstituted from an initial wave of monocytes, but thought to be superseded by more permanent repopulation with undefined LC precur- sors. However, the extent to which this mechanism is relevant to immune-pathological processes that damage LC population integrity is not known. -

Human Anatomy As Related to Tumor Formation Book Four
SEER Program Self Instructional Manual for Cancer Registrars Human Anatomy as Related to Tumor Formation Book Four Second Edition U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Public Health Service National Institutesof Health SEER PROGRAM SELF-INSTRUCTIONAL MANUAL FOR CANCER REGISTRARS Book 4 - Human Anatomy as Related to Tumor Formation Second Edition Prepared by: SEER Program Cancer Statistics Branch National Cancer Institute Editor in Chief: Evelyn M. Shambaugh, M.A., CTR Cancer Statistics Branch National Cancer Institute Assisted by Self-Instructional Manual Committee: Dr. Robert F. Ryan, Emeritus Professor of Surgery Tulane University School of Medicine New Orleans, Louisiana Mildred A. Weiss Los Angeles, California Mary A. Kruse Bethesda, Maryland Jean Cicero, ART, CTR Health Data Systems Professional Services Riverdale, Maryland Pat Kenny Medical Illustrator for Division of Research Services National Institutes of Health CONTENTS BOOK 4: HUMAN ANATOMY AS RELATED TO TUMOR FORMATION Page Section A--Objectives and Content of Book 4 ............................... 1 Section B--Terms Used to Indicate Body Location and Position .................. 5 Section C--The Integumentary System ..................................... 19 Section D--The Lymphatic System ....................................... 51 Section E--The Cardiovascular System ..................................... 97 Section F--The Respiratory System ....................................... 129 Section G--The Digestive System ......................................... 163 Section -

Histiocytic and Dendritic Cell Lesions
1/18/2019 Histiocytic and Dendritic Cell Lesions L. Jeffrey Medeiros, MD MD Anderson Cancer Center Outline 2016 classification of Histiocyte Society Langerhans cell histiocytosis / sarcoma Erdheim-Chester disease Juvenile xanthogranuloma Malignant histiocytosis Histiocytic sarcoma Interdigitating dendritic cell sarcoma Follicular dendritic cell sarcoma Rosai-Dorfman disease Hemophagocytic lymphohistiocytosis Writing Group of the Histiocyte Society 1 1/18/2019 Major Groups of Histiocytic Lesions Group Name L Langerhans-related C Cutaneous and mucocutaneous M Malignant histiocytosis R Rosai-Dorfman disease H Hemophagocytic lymphohistiocytosis Blood 127: 2672, 2016 L Group Langerhans cell histiocytosis Indeterminate cell tumor Erdheim-Chester disease S100 Normal Langerhans cells Langerhans Cell Histiocytosis “Old” Terminology Eosinophilic granuloma Single lesion of bone, LN, or skin Hand-Schuller-Christian disease Lytic lesions of skull, exopthalmos, and diabetes insipidus Sidney Farber Letterer-Siwe disease 1903-1973 Widespread visceral disease involving liver, spleen, bone marrow, and other sites Histiocytosis X Umbrella term proposed by Sidney Farber and then Lichtenstein in 1953 Louis Lichtenstein 1906-1977 2 1/18/2019 Langerhans Cell Histiocytosis Incidence and Disease Distribution Incidence Children: 5-9 x 106 Adults: 1 x 106 Sites of Disease Poor Prognosis Bones 80% Skin 30% Liver Pituitary gland 25% Spleen Liver 15% Bone marrow Spleen 15% Bone Marrow 15% High-risk organs Lymph nodes 10% CNS <5% Blood 127: 2672, 2016 N Engl J Med -

Progress in Understanding the Pathogenesis of Langerhans Cell Histiocytosis: Back to Histiocytosis X?
review Progress in understanding the pathogenesis of Langerhans cell histiocytosis: back to Histiocytosis X? Marie-Luise Berres,1,2,3,4 Miriam Merad1,2,3 and Carl E. Allen5,6 1Department of Oncological Sciences, Mount Sinai School of Medicine, 2Tisch Cancer Institute, Mount Sinai School of Medicine, 3Immunology Institute, Mount Sinai School of Medicine, New York, NY, USA, 4Department of Internal Medicine III, University Hospital, RWTH Aachen, Aachen, Germany, 5Texas Children’s Cancer Center, and 6Baylor College of Medicine, Houston, TX, USA Summary Langerhans cell histiocytosis (LCH) is the most common his- tiocytic disorder, arising in approximately five children per Langerhans cell histiocytosis (LCH), the most common million, similar in frequency to paediatric Hodgkin lym- histiocytic disorder, is characterized by the accumulation of phoma and acute myeloid leukaemia (AML) (Guyot-Goubin CD1A+/CD207+ mononuclear phagocytes within granuloma- et al, 2008; Stalemark et al, 2008; Salotti et al, 2009). The tous lesions that can affect nearly all organ systems. Histori- median age of presentation is 30 months, though LCH is cally, LCH has been presumed to arise from transformed or reported in adults in approximately one adult per million, pathologically activated epidermal dendritic cells called Lan- both as unrecognized chronic paediatric disease and de novo gerhans cells. However, new evidence supports a model in disease (Baumgartner et al, 1997). There are occasional which LCH occurs as a consequence of a misguided differen- reports of affected non-twin siblings and multiple cases in tiation programme of myeloid dendritic cell precursors. one family, though it is not clear if this is significantly more Genetic, molecular and functional data implicate activation frequent than one would expect by chance (Arico et al, of the ERK signalling pathway at critical stages in myeloid 2005). -

Cutaneous Neonatal Langerhans Cell Histiocytosis
F1000Research 2019, 8:13 Last updated: 18 SEP 2019 SYSTEMATIC REVIEW Cutaneous neonatal Langerhans cell histiocytosis: a systematic review of case reports [version 1; peer review: 1 approved with reservations, 1 not approved] Victoria Venning 1, Evelyn Yhao2,3, Elizabeth Huynh2,3, John W. Frew 2,4 1Prince of Wales Hospital, Randwick, Sydney, NSW, 2033, Australia 2University of New South Wales, Sydney, NSW, 2033, Australia 3Sydney Children's Hospital, Randwick, NSW, 2033, Australia 4Department of Dermatology, Liverpool Hospital, Sydney, Sydney, NSW, 2170, Australia First published: 03 Jan 2019, 8:13 ( Open Peer Review v1 https://doi.org/10.12688/f1000research.17664.1) Latest published: 03 Jan 2019, 8:13 ( https://doi.org/10.12688/f1000research.17664.1) Reviewer Status Abstract Invited Reviewers Background: Cutaneous langerhans cell histiocytosis (LCH) is a rare 1 2 disorder characterized by proliferation of cells with phenotypical characteristics of Langerhans cells. Although some cases spontaneously version 1 resolve, no consistent variables have been identified that predict which published report report cases will manifest with systemic disease later in childhood. 03 Jan 2019 Methods: A systematic review (Pubmed, Embase, Cochrane database and all published abstracts from 1946-2018) was undertaken to collate all reported cases of cutaneous LCH in the international literature. This study 1 Jolie Krooks , Florida Atlantic University, was registered with PROSPERO (CRD42016051952). Descriptive statistics Boca Raton, USA and correlation analyses were undertaken. Bias was analyzed according to Milen Minkov , Teaching Hospital of the GRADE criteria. Medical University of Vienna, Vienna, Austria Results: A total of 83 articles encompassing 128 cases of cutaneous LCH were identified. -

Case Report Congenital Self-Healing Reticulohistiocytosis
Case Report Congenital Self-Healing Reticulohistiocytosis Presented with Multiple Hypopigmented Flat-Topped Papules: A Case Report and Review of Literatures Rawipan Uaratanawong MD*, Tanawatt Kootiratrakarn MD, PhD*, Poonnawis Sudtikoonaseth MD*, Atjima Issara MD**, Pinnaree Kattipathanapong MD* * Institute of Dermatology, Department of Medical Services Ministry of Public Health, Bangkok, Thailand ** Department of Pediatrics, Saraburi Hospital, Sabaruri, Thailand Congenital self-healing reticulohistiocytosis, also known as Hashimoto-Pritzker disease, is a single system Langerhans cell histiocytosis that typically presents in healthy newborns and spontaneously regresses. In the present report, we described a 2-month-old Thai female newborn with multiple hypopigmented flat-topped papules without any internal organ involvement including normal blood cell count, urinary examination, liver and renal functions, bone scan, chest X-ray, abdominal ultrasound, and bone marrow biopsy. The histopathology revealed typical findings of Langerhans cell histiocytosis, which was confirmed by the immunohistochemical staining CD1a and S100. Our patient’s lesions had spontaneously regressed within a few months, and no new lesion recurred after four months follow-up. Keywords: Congenital self-healing reticulohistiocytosis, Congenital self-healing Langerhans cell histiocytosis, Langerhans cell histiocytosis, Hashimoto-Pritzker disease, Birbeck granules J Med Assoc Thai 2014; 97 (9): 993-7 Full text. e-Journal: http://www.jmatonline.com Langerhans cell histiocytosis (LCH) is a multiple hypopigmented flat-topped papules, which clonal proliferative disease of Langerhans cell is a rare manifestation. involving multiple organs, including skin, which is the second most commonly involved organ by following Case Report the skeletal system(1). LCH has heterogeneous clinical A 2-month-old Thai female infant presented manifestations, ranging from benign single system with multiple hypopigmented flat-topped papules since disease to fatal multisystem disease(1-3). -

Malignant Histiocytosis in a Cat – Case Report
Trost et al; Malignant histiocytosis in a cat - Case report. Braz J Vet Pathol; 2008, 1(1): 32 - 35 32 Case Report Malignant histiocytosis in a cat – Case report Maria E. Trost 1, Adriano T. Ramos 1, Eduardo K. Masuda 1, Bruno L. dos Anjos 1, Marina G. M. C. M. Cunha 2, Dominguita L. Graça 3* 1Laboratory of Veterinary Pathology, Federal University of Santa Maria (UFSM), RS, Brazil. 2Laboratory of Veterinary Surgery, Federal University of Santa Maria (UFSM), RS, Brazil. 3Department of Pathology, Federal University of Santa Maria (UFSM), RS, Brazil. *Corresponding author: Dominguita L. Graça, Department of Pathology, Science Health Center, UFSM, 97105-900, Santa Maria, RS, Brazil. Email: [email protected]. Submitted December 13th 2007, Accepted March 3rd 2008 Abstract A crossbred 14-year-old castrated male cat had a history of lethargy, anorexia and weight loss of one month evolution. On clinical examination, anemia, emaciation, jaundice and a large mass in the abdomen were detected. Ultrasonography revealed hepatomegaly and a single splenic mass. The cat was submitted to biopsy and euthanatized during the surgical procedure. The diagnosis of malignant histiocytosis was achieved on the basis of the clinical presentation, histopathologic and immunoistochemical findings. Key Words: Malignant histiocytosis, histiocytic diseases, neoplasia, pathology, diseases of cats Introduction in the literature (8); It affects individuals of several ages, with no sex or breed predisposition. The most affected Histiocytic neoplasms are a group of diseases organs are the spleen, liver, lung and bone marrow. Cats classified accordingly to local and biological behavior. with MH are anorexic, emaciated, lethargic, with fever and Focal and self-limiting lesions (cutaneous histiocytoma), dyspnea in a few cases. -

Epidermal Macrophage Induction, and Langerhans Cell Depletion (Photoimmunology/Ozone Depletion/Contact Sensitivity/T Lymphocytes/Antigen Presenting Cells) K
Proc. Nati. Acad. Sci. USA Vol. 89, pp. 8497-8501, September 1992 Immunology UV exposure reduces immunization rates and promotes tolerance to epicutaneous antigens in humans: Relationship to dose, CDla-DR+ epidermal macrophage induction, and Langerhans cell depletion (photoimmunology/ozone depletion/contact sensitivity/T lymphocytes/antigen presenting cells) K. D. COOPER*t*, L. OBERHELMAN*, T. A. HAMILTON*, 0. BAADSGAARD*§, M. TERHUNE*, G. LEVEE*, T. ANDERSON*t, AND H. KOREN¶ *Immunodermatology Unit, Department of Dermatology, University of Michigan, Ann Arbor, MI 48109; tVeterans Administration Hospital, Ann Arbor, MI 48105; and 'Health Effects Research Labs, Environmental Protection Agency, Chapel Hill, NC 27711 Communicated by Thomas M. Donahue, May 1, 1992 ABSTRACT Increasing UVB radiation at the earth's sur- tibility of UV-exposed mice and the unresponsiveness of face might have adverse effects on in vivo immunologic responses UV-exposed mice to contact allergens were found to be due in humans. We prospectively randomized subjects to test to antigen-specific suppressor T lymphocytes (12, 13). whether epicutaneous immunization is altered by prior admin- UV regulation of murine contact sensitivity has held up istration of biologically equalized doses of UV radiation. Mul- well as a model of immunologic events occurring in photo- tiple doses of antigens on upper inner arm skin (UV protected) carcinogenesis. Epidermal Langerhans cells, an antigen pre- were used to elicit contact sensitivity responses, which were senting population of dendritic cell lineage present in the quantitated by measuring increases in skin thickness. If a dose epidermis (14), have a potent capacity to initiate contact of UVB sufficient to induce redness (erythemagenic) was ad- sensitivity reactions (15, 16), as well as tumor rejection (17). -

Langerhans Cell Langhans Cell
1 Q Ocular-Surface Immunology The names of these two cell types are easily confused—what are they? This one is: --A type of dendritic cell residing in the ocular surface epithelium --An antigen-presenting cell (APC) --Described as the ‘immune sentinels of the ocular surface’ Langerhans cell This one is: --A type of giant cell found in granulomas --Associated with TB --Horseshoe-like arrangement of nuclei Langhans cell 2 A Ocular-Surface Immunology The names of these two cell types are easily confused—what are they? This one is: --A type of dendritic cell residing in the ocular surface epithelium --An antigen-presenting cell (APC) --Described as the ‘immune sentinels of the ocular surface’ Langerhans cell This one is: --A type of giant cell found in granulomas --Associated with TB --Horseshoe-like arrangement of nuclei Langhans cell 3 Ocular-Surface Immunology The names of these two cell types are easily confused—what are they? This one is: --A type of dendritic cell residing in the ocular surface epithelium --An antigen-presenting cell (APC) --Described as the ‘immune sentinels of the ocular surface’ Langerhans cell The … This one is: ER --A type of giant cell found in granulomas --Associated with TB --Horseshoe-like arrangement of nuclei Langhans cell 4 Ocular-Surface Immunology The names of these two cell types are easily confused—what are they? This one is: --A type of dendritic cell residing in the ocular surface epithelium --An antigen-presenting cell (APC) --Described as the ‘immune sentinels of the ocular surface’ Langerhans cell