Practice Makes Perfect
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

IZOD Indycar® Series & Firestone Indy Lights
® DARIO FRANCHITTIDARIO Chip Ganassi Racing Target Series Champion 2011 IZOD IndyCar IZOD IndyCar ® Series & Firestone Indy Lights™ 2012 Trackside INDYCAR Media Web Site – media.indycar.com A media-only section of the INDYCAR’s Web site is available for media use. This site contains general content about the IZOD IndyCar® Series and Firestone Indy Lights, including: IZOD IndyCar Series and Firestone Indy Lights logos for download Graphics and special event photo galleries for download and publication INDYCAR PR contacts Team PR contacts Track contacts Teleconference advisories Teleconference transcripts, press releases, advisories and notebooks Weekly Video News Feed advisories and digital copies Information about each event also is available, including: Complete event schedules Broadcast information Daily Trackside Reports, including session details and quotes Event Video News Release advisories Event press conference transcripts The address for the media site is: http://media.indycar.com INDYCAR Media Photo Web Site – IndyCarMedia.com A media-only website is available for media to download high-resolution photos of at-track events and studio photos of drivers. Note, registration is required to access the side The address for the media site is: http://www.indycarmedia.com INDYCAR PR CONTACT INFORMATION 1. INDYCAR. Contact information for members of INDYCAR Public Relations: a. Amy Konrath, Vice President of Communications/Public Relations 317-331-7437 – cell; 317-492-6453 – office; [email protected] b. Denise Abbott, Vice President of Public Relations 310-430-0496 – cell; 317-492-8836 – office; [email protected] c. Steve Shunck, Vice President of Public Relations 317-716-9188 – cell; 317-492-8532 – office; [email protected] d. -

The Chicago March 2020
The chicago March 2020 Official Publication • PCA-Chicago Blackhawk Tips Bad Weather, Good Times Springtime for Autocrossers March 2020 Contents 6 Features 5 Letter from the President 6 Bad Weather, Good Times, Great Friends 9 Questions? Answers! A Day at Blackhawk 26 The Social Scene 14 Springtime for Autocrossers 29 2020 Chicago Region Calendar 20 Past Mistakes Make for Future Success (Rallye) 32 The Old Road Course: A Perspective 42 Backroads: 1997 32 14 On The Cover: Photo by Neil MacDonald Top photo: Zoe and the Christmas tree by Steve Marchino Bottom left: by Neil MacDonald Bottom right: by Phil Nesius March 2020 | The chicago Scene 3 Advertisers Northstar Motorsports . Inside Front Cover The Chicago Scene is an official publication of Midwest Performance Cars . Inside Back Cover PCA – Chicago Region. The magazine is G Design Racing . Back Cover published bimonthly. Isringhausen Imports . 8 Editor Lake Barrington Motorsports . 10 Neil MacDonald Fischer Motors . .11 Autobahn Country Club . 15 Contributing Writers Janet Marinis Group . 18 Dan Cubric Olsen MotorSports . 19 Dana Comolli Shawn Folkes Napleton Westmont Porsche . 21 James Jacisin Big Door . 24 Steve Kuk Porsche Auto Insurance . 25 Bob Rath Midwest Eurosport . 27 Anna Skura Porsche Exchange . 31 Contributing Photographers Porsche Barrington . 33 Michael Bene Barnaba Autosport . 34 Jeff Brown Collectors’ Car Garage . 36 Dan Cubric R .A . Adams . 37 Neil MacDonald Steve Marchino CWS Car Brokers . 39 Phil Nesius Iron Gate Motor Condos . 40 Archival photos provided by O’Hare -

Karam Leads Every Lap of USF2000 Race at Autobahn Country Club Sunday
Andersen RacePark 10101 U.S. Highway 41 North Palmetto, Fla. 34221 Tel.: (941) 723-3900 Fax: (941) 723-3992 E-mail: [email protected] Web site: usf2000.com Media inquiries: Linda Mansfield, Restart Communications Cell: (317) 201-0729 E-mail: [email protected] Karam Leads Every Lap of USF2000 Race At Autobahn Country Club Sunday JOLIET, Ill., Aug. 1 — Polesitter Sage Karam of Nazareth, Pa. led all 12 laps to win Round 8 of the “Cooper Tires Presents the USF2000 National Championship Powered by Mazda” in convincing fashion Sunday afternoon during the Harrahʼs Autobahn Grand Prix Presented by Mazda at the Autobahn Country Club. The Andretti Autosport driver had a 2.312-second advantage over the No. 2 Cape Motorsports with Wayne Taylor Racing car driven by Patrick McKenna of Dublin, Ireland at the checkered. Both Karam and McKenna were in Mazda- powered Van Diemens. Tonis Kasemets of Mundelein, Ill., who won a similar race here Saturday, finished third Sunday in a Zetec-powered Van Diemen fielded by Pabst Racing Services. Karam stretched his advantage to 4 seconds by lap seven and was never threat - ened with his No. 8, which is sponsored by the Michael Fux Foundation, Comfort Revolution, Bell Helmets, Alpine Stars, Walters Web and artrotundo.com. The real story was the battle for second. McKenna started in that position only to lose it to Kasemets working lap two. McKenna, who is sponsored by Motor - sport Ireland and Willsborough Transport, was in hot pursuit in third place, how - ever, followed closely by Liberty Motorsportsʼ Matthew Powers of Danville, Calif. -

IZOD Indycar® Series & Firestone Indy Lights™ 2012 Trackside
® DARIO FRANCHITTIDARIO Chip Ganassi Racing Target Series Champion 2011 IZOD IndyCar IZOD IndyCar ® Series & Firestone Indy Lights™ 2012 Trackside INDYCAR Media Web Site – media.indycar.com A media-only section of the INDYCAR’s Web site is available for media use. This site contains general content about the IZOD IndyCar® Series and Firestone Indy Lights, including: IZOD IndyCar Series and Firestone Indy Lights logos for download Graphics and special event photo galleries for download and publication INDYCAR PR contacts Team PR contacts Track contacts Teleconference advisories Teleconference transcripts, press releases, advisories and notebooks Weekly Video News Feed advisories and digital copies Information about each event also is available, including: Complete event schedules Broadcast information Daily Trackside Reports, including session details and quotes Event Video News Release advisories Event press conference transcripts The address for the media site is: http://media.indycar.com INDYCAR Media Photo Web Site – IndyCarMedia.com A media-only website is available for media to download high-resolution photos of at-track events and studio photos of drivers. Note, registration is required to access the side The address for the media site is: http://www.indycarmedia.com INDYCAR PR CONTACT INFORMATION 1. INDYCAR. Contact information for members of INDYCAR Public Relations: a. Amy Konrath, Vice President of Communications/Public Relations 317-331-7437 – cell; 317-492-6453 – office; [email protected] b. Denise Abbott, Vice President of Public Relations 310-430-0496 – cell; 317-492-8836 – office; [email protected] c. Steve Shunck, Vice President of Public Relations 317-716-9188 – cell; 317-492-8532 – office; [email protected] d. -
2012 Media Guide FAST FACTS
2012 Media Guide FAST FACTS Story Ideas: Highly-competitive season makes returns to ovals at Milwaukee The2012 Firestone Indy Lights season returns to ovals for the next two races beginning with the Firestone Indy Lights 100 at the famed Milwaukee Mile. Firestone Indy Defending race winner Esteban Guerrieri leads the points by 15 markers over rookie. Lights 100 teammate Tristan Vautier with Sebastian Saavedra 16 points behind. Can one of the lead trio take control of the points at Milwaukee? Date / Time 5:45 p.m. (EDT) Veterans return in search champion’s scholarship Friday, June 15 Esteban Guerrieri, who finished second in the point standings in 2011, leads a talented group of drivers returning to Firestone Indy Lights for the 2012 season in hopes of Track securing the Mazda Road to Indy scholarship to graduate to the IZOD IndyCar Series in The Milwaukee 2013. Belle Isle race winner Gustavo Yacaman, who will race in his fourth Firestone Mile Freedom 100, Jorge Goncalvez, Juan Pablo Garcia, join Guerrieri, a two-time race (1-mile oval) winner in 2012, in the field for this weekend’s race. Distance Saavedra returns to chase title 100 laps/100 miles Sebastian Saavedra, who claimed three wins and the series rookie title in his two seasons in Firestone Indy Lights, is off to a strong start in his returns to the series. The TV Colombian returned AFS Racing/Andretti Autosport to victory lane at Barber. Can NBC Sports Saavedra, who competed in the IZOD IndyCar Series in 2011, do the same in Network (Taped), Milwaukee? 5 p.m. -

2020 Suzuki Road Racing Contingency Payout Schedule (Schedule and Payouts Are Subject to Change at the Discretion of Suzuki)
2020 SUZUKI ROAD RACING CONTINGENCY PAYOUT SCHEDULE (SCHEDULE AND PAYOUTS ARE SUBJECT TO CHANGE AT THE DISCRETION OF SUZUKI) AFM www.AFMracing.org 1st 2nd 3rd 4th 5th 600 Superbike $500 $250 $125 $75 $50 750 Superbike $500 $250 $125 $75 $50 Open Superstock $500 $250 $125 $75 $50 Formula Pacific $500 $250 $125 $75 $50 900 Superbike $500 $250 $125 $75 $50 600 Superstock $500 $250 $125 $75 $50 750 Superstock $500 $250 $125 $75 $50 900 Superstock $500 $250 $125 $75 $50 Qualified Events: 7 Series Payout: $42,000 Mar 21-22 Buttonwillow Bakersfield, CA Apr 25-26 Buttonwillow Bakersfield, CA May 9-10 Thunderhill Willows, CA Jun 27-29 Thunderhill Willows, CA Sept 5-6 Sonoma Sonoma, CA Oct 3-4 Buttonwillow Bakersfield, CA Oct 17-18 Pacific Pro Am- Thunderhill *DOUBLE CONTINGENCY Willows, CA 3/5/2020 2020 SUZUKI ROAD RACING CONTINGENCY PAYOUT SCHEDULE (SCHEDULE AND PAYOUTS ARE SUBJECT TO CHANGE AT THE DISCRETION OF SUZUKI) CCS www.ccsracing.us 1st 2nd 3rd 4th 5th Ex. Supersport Middleweight $500 $250 $125 $75 $50 Ex. Supersport Heavyweight $500 $250 $125 $75 $50 Ex. Supersport Unlimited $500 $250 $125 $75 $50 Ex. Grand Prix Unlimited $500 $250 $125 $75 $50 Qualified Events: 29 Series Payout: $116,000 *Sunday only on dbl. weekends Feb 8-9 Homestead Miami Cancelled Miami, FL Feb 29-Mar 1 Roebling Raceway Bloomingdale, GA Mar 13-15 Daytona Intl Speedway Daytona Beach, FL Apr 4-5 Carolina Motorsports Park Kershaw, SC Apr 25-26 New Jersey Motorsports Park Millville, NJ May 2-3 Autobahn Country Club Joilet, IL May 2-3 New Hampshire Mtr Speedway Loudon, NH May 16-17 Blackhawk Farms Raceway S. -

Racing Factbook Circuits
Racing Circuits Factbook Rob Semmeling Racing Circuits Factbook Page 2 CONTENTS Introduction 4 First 5 Oldest 15 Newest 16 Ovals & Bankings 22 Fastest 35 Longest 44 Shortest 48 Width 50 Corners 50 Elevation Change 53 Most 55 Location 55 Eight-Shaped Circuits 55 Street Circuits 56 Airfield Circuits 65 Dedicated Circuits 67 Longest Straightaways 72 Racing Circuits Factbook Page 3 Formula 1 Circuits 74 Formula 1 Circuits Fast Facts 77 MotoGP Circuits 78 IndyCar Series Circuits 81 IMSA SportsCar Championship Circuits 82 World Circuits Survey 83 Copyright © Rob Semmeling 2010-2016 / all rights reserved www.wegcircuits.nl Cover Photography © Raphaël Belly Racing Circuits Factbook Page 4 Introduction The Racing Circuits Factbook is a collection of various facts and figures about motor racing circuits worldwide. I believe it is the most comprehensive and accurate you will find anywhere. However, although I have tried to make sure the information presented here is as correct and accurate as possible, some reservation is always necessary. Research is continuously progressing and may lead to new findings. Website In addition to the Racing Circuits Factbook file you are viewing, my website www.wegcircuits.nl offers several further downloadable pdf-files: theRennen! Races! Vitesse! pdf details over 700 racing circuits in the Netherlands, Belgium, Germany and Austria, and also contains notes on Luxembourg and Switzerland. The American Road Courses pdf-documents lists nearly 160 road courses of past and present in the United States and Canada. These files are the most comprehensive and accurate sources for racing circuits in said countries. My website also lists nearly 5000 dates of motorcycle road races in the Netherlands, Belgium, Germany, Austria, Luxembourg and Switzerland, allowing you to see exactly when many of the motorcycle circuits listed in the Rennen! Races! Vitesse! document were used. -

Remarks Chicago Region RE, Rick Bentson July 1, 2016
REmarks Chicago Region RE, Rick Bentson July 1, 2016 What a month June has been! The first 9 days of the month were the calm before the storm of events. Beginning June 10 things got real with 44 cars taking to the track at our PDX Track Day event at Autobahn Country Club. Yours truly served as Chief Steward, with an assist from George Laws so I could exit early to get some sleep before getting up at half-past-the- middle-of-the-night for the drive to Blackhawk Farms, timed to arrive in time for the morning Worker meeting to work corners for the Milwaukee/Blackhawk Valley regions Double Divisional race weekend. This would be weekend one of the June Triple Header of race weekends. Following the Blackhawk Farms weekend, the 61st running of the Chicago Region June Sprints at Road America greeted 308 entries with great weather (unlike last year, which featured 3 days of rain) and 3 days of very competitive racing, including 67 Spec Racer Fords! As an added bonus for the spectators in attendance the Battery Tender Mazda MX-5 Cup pro series was included on the weekend’s schedule, bringing an additional 42 cars and their own brand of great racing. As a Jack-of-all-Trades of sorts for the weekend I had the pleasure of being able to experience the many flavors of the June Sprints and I gotta tell ya, I couldn’t be more proud of the event we put on! From Registration, to Tech (with free soft-serve ice cream for drivers, crew and anyone else who stops by!), to the amazing job done by the combined Road America/SCCA crew in Race Control, to the best corner marshalling crew in the country (a bit of personal bias there, I admit, but I don’t think I’m wrong), to the best, and I mean the BEST podium ceremony in all of amateur racing. -

Star Mazda Racers to Battle for VISIT FLORIDA Cup
Contact: Dean Case, Communications Officer , MAZDASPEED Motorsports Development (310) 318-4582, [email protected] Kathy Torian, Corporate Communications Manager, VISIT FLORIDA (850) 205-3865, [email protected] ® ZOOM-ZOOM FLORIDA STYLE Star Mazda Racers to Battle for VISIT FLORIDA Cup December 10, 2009 (Orlando, Fla.). MAZDASPEED racers compete in a host of series from coast-to- coast, but certain states have a disproportionate number of great race tracks. Florida, the No. 1 travel destination in the world, is home to dozens of iconic race tracks including Daytona, Sebring, Homestead, Gainesville and the St. Petersburg street course. ® Mazda has formed a partnership with VISIT FLORIDA , the state’s official tourism marketing corporation, to promote awareness of the many attributes of the Sunshine State to race fans. Mazda race teams will be promoting Florida vacations in target markets throughout the year. Racers competing in the Star Mazda Championship Presented by Goodyear will be competing for a new award, the VISIT FLORIDA Cup. The racer scoring the most points in five specific races will win the Cup, as well as a personalized Florida dream vacation. The five races are: • Sebring International Raceway (Sebring) • New Jersey Motorsports Park (New York City) • Autobahn Country Club (Chicago) • Mosport International Raceway (Toronto) • Road Atlanta (Atlanta) Quotes: Will Seccombe, Chief Marketing Officer, VISIT FLORIDA -- “We’ve seen what the Mazda racers have done as brand ambassadors for Mazda and are anxious to have them share the wonders of Florida with their friends and fans. The fact that the Star Mazda series draws racers from around the world makes it a great fit to promote Florida on a global level.” Robert Davis, Senior Vice President, Mazda North American Operations -- “Growing up in the South, I’ve taken many wonderful trips to Florida for Speed Week and Bike Week over the years. -

Andersen Racing Takes Second, Third and Fourth in Sunday's Star
10101 U.S. Highway 41 Palmetto, Fla. 34221 Tel.: (941) 723-3900 Fax: (941) 723-3992 [email protected] andersenracing.com For media information: Linda Mansfield, Restart Communications Cell: (317) 201-0729 E-mail: [email protected] Andersen Racing Takes Second, Third and Fourth In Sunday’s Star Mazda Race At Autobahn Country Club JOLIET, Ill., Aug. 1 — Two Andersen Racing drivers, Tristan Vautier and Anders Krohn, finished second and third in Sunday’s Star Mazda race at the Autobahn Country Club, while the Andersen Racing driver who won Saturday’s race, Mikael Grenier, placed fourth. Nick Andries placed tenth for the team Sunday and Dom Bastien was 21st in Round 9 of the series, which is presented by Goodyear. m-o-r-e Andersen Racing Sunday Star Mazda Results/Page 2 of 7 Vautier was just 0.213 of a second behind polesitter and eventual winner Conor Daly in qualifying Sunday morning to earn a spot on the front row for the standing start Sunday afternoon. Krohn was just a heartbeat slower to earn the third starting position. Grenier qualified fifth; Andries 11th and Bastien 23rd. The only change to the top four positions in the non-stop, 45-minute/21- lap race occurred at the start when Grenier blasted by the driver who had qualified fourth, Caio Lara, to earn that position. Daly had over a 3-second lead several times, but Vautier had cut that to only 0.979 of a second at the checkered. The rookie from Corenc, France was rebounding from electrical problems with his car, which is sponsored by Moulin T.P., Cecibon, Circuit du Laquis, Fontanel Promotion and Allied Building Products Corp., in Saturday’s race. -

USA Track Data Base (68) / As of 11/10/2020
Garmin Catalyst - USA Track Data Base (68) / as of 11/10/2020 Arizona Motorsports Park, Litchfield Park, AZ Arroyo Seco Raceway, Deming, NM Aspen Motorsports Park, Woody Creek, CO Atlanta Motor Speedway, Hampton, GA Atlanta Motorsports Park, Dawsonville, GA Auto Club Speedway, Fontana, CA Autobahn Country Club, Joliet, IL Barber Motorsports Park, Birmingham, AL Berlin Raceway, Marne, MI Blackhawk Farms Raceway, South Beloit, IL Brainerd International Raceway, Brainerd, MN Bristol Motor Speedway, Bristol, TN Brooklyn Street Circuit, Brooklyn, NY Buttonwillow Raceway Park, Buttonwillow, CA Canaan Motor Club, Canaan, NH Carolina Motorsports Park Inc, Kershaw, SC Charlotte Motor Speedway, South Concord, NC Chicagoland Speedway, Joliet, IL Chuckwalla Valley Raceway CCW, Desert Center, CA Circuit of the Americas (COTA), Austin, TX Club Motorsports, Tamworth, NH Darlington Raceway, Darlington, SC Daytona International Speedway, Daytona Beach, FL Detroit Belle Isle, Detroit, MI Dominion Raceway, Thornburg, VA Dover International Speedway, Dover, DE Driveway Austin, Austin, TX Eagles Canyon Raceway, Decatur, TX Exotics Racing Las Vegas, Las Vegas, NV Firestone Grand Prix of St. Petersburg, St. Petersburg, FL Gingerman Raceway, South Haven, MI Grand Prix Of Long Beach, Long Beach, CA Grattan Raceway, Belding, MI Hallett Motor Racing Circuit, Jennings, OK Harris Hill Raceway, San Marcos, TX Heartland Motorsports Park, Topeka, KS High Plans Raceway, Deer Tail, CO Homestead-Miami Speedway, Homestead, FL Hutchinson -
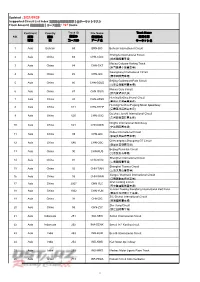
Updated : 2021/09/29 Supported Circuit List Index 支援的全球賽道清單│全サーキットリスト Track Amount 賽道總數量│コース総数 : 747 Tracks
Updated : 2021/09/29 Supported Circuit List Index 支援的全球賽道清單│全サーキットリスト Track Amount 賽道總數量│コース総数 : 747 tracks Continent Country Track ID File Name Track Name NO. 洲別 國家 賽道ID 賽道檔名 賽道名稱 地域 国 コースID データ名 サーキット名 1 Asia Bahrain 69 BRN-BIC Bahrain International Circuit Chengdu International Circuit 2 Asia China 83 CHN-CDIC (成都國際賽車場) Macau Coloane Karting Track 3 Asia China 84 CHN-CKT (澳門路環小型賽車場) Guangdong International Circuit 4 Asia China 85 CHN-GIC (廣東國際賽車場) Beijing Goldenport Park Circuit 5 Asia China 86 CHN-GOLD (北京金港國際賽車場) Macau Guia Circuit 6 Asia China 87 CHN-GUIA (澳門東望洋賽道) Hunting Beijing Shunyi Circuit 7 Asia China 88 CHN-HTBS (豪庭北京順義賽車場) Hunting Huizhou Fugang Motor Speedway 8 Asia China 611 CHN-HTHF (豪霆惠州福岗赛车场) Guizhou Junchi International Circuit 9 Asia China 620 CHN-JCIC (贵州骏驰国际赛车场) Ningbo International Speedway 10 Asia China 621 CHN-NBIS (宁波国际赛车场) Ordos International Circuit 11 Asia China 89 CHN-OIC (鄂爾多斯國際賽車場) Qinhuangdao Shougang GT Circuit 12 Asia China 640 CHN-QSC (秦皇岛首钢赛车场) Beijing Ruisiclub Circuit 13 Asia China 90 CHN-RUS (北京銳思賽車場) Shanghai International Circuit 14 Asia China 91 CHN-SHIC (上海國際賽車場) Shanghai Tianma Circuit 15 Asia China 92 CHN-TIAN (上海天馬山賽車場) Jiangsu Wantrack International Circuit 16 Asia China 93 CHN-WAN (江蘇萬馳國際賽車場) Xi'an Lintong Circuit 17 Asia China 2067 CHN-XLC (西安臨潼國際賽車場) Yunnan Trading Xiongfeng International Kart Field 18 Asia China 1062 CHN-YUN (雲南交投雄風卡丁車場) ZIC-Zhuhai International Circuit 19 Asia China 94 CHN-ZIC (珠海國際賽車場) Zhe Jiang Circuit 20 Asia China 95 CHN-ZJC (浙江国际赛车场) 21 Asia Indonesia 251 INA-SEN Sentul International Circuit 22 Asia Indonesia 252 INA-SENK Sentul Int'l Karting circuit 23 Asia India 253 IND-BUD Buddh International Circuit 24 Asia India 254 IND-KMS Kari Motor Speedway 25 Asia India 255 IND-MMS Madras Motor Sports Race Track 26 Asia Israel 713 ISR-PEZA Pezael Circuit Anti-Clockwise 1 Continent Country Track ID File Name Track Name NO.