Assessment on Clinical Management of Rape in Low Resource Settings
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Conflict Uganda
Health workers’ career paths, livelihoods and coping strategies in conflict and post- conflict Uganda Justine Namakula, Sophie Witter, Freddie Ssengooba and Sarah Ssali (2013) Acknowledgement This work was supported by UK Department for International Development (DFID) through the ReBUILD Consortium. The authors are deeply grateful for the financial support to carry out this work. This work draws on the life histories and experiences of health workers at different levels of the health system in Gulu, Amuru, Kitgum and Pader. We thank health workers for their patience, time, cooperation, insights and experiences shared during the research process without which this work would not have been possible. We also appreciate the contribution Ms. Adongo Jennifer, Mrs Sarah Auma Ssempebwa, Mr. Deo Tumusange, Mr. Tenywa Ronald, Ms. Resty Nakayima and Ms Eunice Kyomugisha for their hard work and contribution to the data collection and transcription of the interviews. We pray and hope that these research findings make a concrete contribution towards improving subsequent incentive interventions that can make a difference to the lives of health workers in Northern Uganda and other post conflict areas. 2 | P a g e Contents Acknowledgement ..................................................................................................................... 2 Contents ..................................................................................................................................... 3 Executive summary ................................................................................................................... -

Vote: 611 Agago District 2012/13 Quarter 2 Structure of Quarterly Performance Report Summary
Local Government Quarterly Performance Report Vote: 611 Agago District 2012/13 Quarter 2 Structure of Quarterly Performance Report Summary Quarterly Department Workplan Performance Cumulative Department Workplan Performance Location of Transfers to Lower Local Services and Capital Investments Submission checklist I hereby submit _________________________________________________________________________. This is in accordance with Paragraph 8 of the letter appointing me as an Accounting Officer for Vote:611 Agago District for FY 2012/13. I confirm that the information provided in this report represents the actual performance achieved by the Local Government for the period under review. Name and Signature: Chief Administrative Officer, Agago District Date: 6/6/2013 cc. The LCV Chairperson (District)/ The Mayor (Municipality) Page 1 Local Government Quarterly Performance Report Vote: 611 Agago District 2012/13 Quarter 2 Summary: Overview of Revenues and Expenditures Overall Revenue Performance Cumulative Receipts Performance Approved Budget Cumulative % Receipts Budget UShs 000's Received 1. Locally Raised Revenues 194,861 107,000 55% 2a. Discretionary Government Transfers 3,402,834 1,349,642 40% 2b. Conditional Government Transfers 13,006,953 6,266,062 48% 2c. Other Government Transfers 1,627,157 389,240 24% 3. Local Development Grant 934,301 443,793 48% 4. Donor Funding 789,893 160,548 20% Total Revenues 19,955,999 8,716,286 44% Overall Expenditure Performance Cumulative Releases and Expenditure Perfromance Approved Budget Cumulative Cumulative -

Comboni's Holiness in His Followers
COMBONI’S HOLINESS IN HIS FOLLOWERS Fr. Lorenzo Carraro, MCCJ COMBONI’S HOLINESS IN HIS FOLLOWERS Fr. Lorenzo Carraro, MCCJ Manila, August 2018 1 TABLE OF CONTENTS Opening Essay: Comboni’s Holiness in his followers…………… pag. 3 Patient Vision: Archbishop Agostino Baroni…………………………….8 Blue Eyes: Bro. Vittorio Fanti……………………………………………..11 Fugitive for God: Sr. Lucia Careddu……………………… …………… 14 Double Impact: Fr. Fulvio Cristoforetti …………… ………………… 19 The Wars of a Man of Peace: Fr. Giuseppe Ambrosoli……………….. 24 Mission Accomplished: Bishop Cesare Mazzolari… ………………….29 Fr. Lele’s Legacy: Fr. Ezechiel Ramin………………………………… .. 35 Singing through Life: Bro. Bernard Pratt………………………………….39 Dom Franco’s Bicycle: Bishop Gianfranco Masserdotti… ……………..42 Lifeblood of Africa: Fr. Tarcisio Agostoni………………… …………48 Letters from the dead: Srs. Cesarina Borghesi & Federica Bettari…… …55 A Life for Ethiopia: Bishop Armido Gasparini…………………………….58 Note: The Opening Essay was written on the occasion of Bishop Comboni’s Canonization ((2003). The 13 profiles were published in World Mission or in Friends of the Missions Newsletter (Fr. Lorenzo Carraro, MCCJ). &&&&&& 2 COMBONI’S HOLINESS IN HIS FOLLOWERS Comboni’s canonization is a gift for each one of us, Comboni missionaries, and a challenge to understand the inner logic in this happening that God has prepared for us. What strikes me lately is the quality of witness of the sons and daughters of Comboni as it stands out from the profiles of the confreres and con-sisters who reach the end of their lives on earth and whom I have known. What follows is the presentation of one of them, but in the background of the call of for holiness and in connection with the example of Comboni himself. -
ICRC ASSISTANCE PROGRAMMES Projection for 2009 in Northern Uganda Pascal Jequier /ICRC Pascal
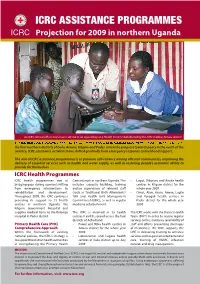
ICRC ASSISTANCE PROGRAMMES Projection for 2009 in northern Uganda Pascal Jequier /ICRC Pascal An ICRC clinical offi cer and a nurse attend to an injured boy at a Health Centre rehabilitated by the ICRC in Bibia, Amuru district the four northern districts of Gulu, Amuru, Kitgum and Pader. Given the progress towards peace in the north of the country, ICRC assistance activities have shifted gradually from emergency response to livelihood support. The aim of ICRC assistance programmes is to promote self-reliance among aff ected communities, improving the delivery of essential services such as health and water supply, as well as restoring people’s economic ability to provide for themselves. ICRC Health Programmes ICRC health programmes aim at Care network in northern Uganda. This • Lagot, Dibolyec and Anaka health bridging gaps during a period shifting includes capacity building, training centres in Kitgum district for the from emergency interventions to and/or supervision of relevant staff whole year 2009 rehabilitation and development. (such as Traditional Birth Attendants/ • Omot, Alim, Arum, Awere, Lagile Throughout 2009, the ICRC continues TBA and Health Unit Management and Porogali health centres in providing its support to 13 health Committees/HUMC), as well as regular Pader district for the whole year centres in northern Uganda, the medicine refurbishment. 2009 Kitgum Government Hospital and supplies medical items to the Kalongo The ICRC is involved in 13 health The ICRC works with the District Health Hospital in Pader district. centres II and III, spread across the four Team (DHT) in order to secure regular districts of Acholiland: services to the structures (availability of Primary Health Care (PHC) • Pawel and Bibia health centres in staff and eff orts preventing shortages Comprehensive Approach Amuru district for the whole year of medicines). -

Joint Press Release
JOINT PRESS RELEASE FACING COVID-19 AT KALONGO HOSPITAL. THE ITALIAN AGENCY FOR DEVELOPMENT COOPERATION SUPPORTS THE HOSPITAL EFFORTS IN DEALING WITH NEGATIVE IMPACT OF COVID-19 ON HEALTH SERVICES. Thanks to the support of the Italian Agency for Development Cooperation (AICS), Dr. Ambrosoli Memorial Hospital in Kalongo (Uganda) has received blood bags and other material necessary for emergency and life saving blood transfusions. This support is part of the ongoing efforts of the AICS Nairobi Regional office to support local health systems in the Region that, under the extraordinary circumstances brought about by the Covid-19 pandemic, are facing constraints to provide also a more effective and timely life-saving response. Dr. Ambrosoli Memorial Hospital is the only hospital in Agago district, serving as head of sanitary district. Within this mandate, the hospital was appointed by the Ministry of Health as the official Covid hub for Agago district, with the laboratory coordinating sample collection in the district, and the hospital CEO being member of the District Committee for Covid-19. The adverse effects of the pandemic have severely affected the delivery of basic health services in the hospital, with patients delaying access to medical care due to fear of contagion, thus reaching the hospital in critical conditions, some of which require emergency and life saving blood transfusions. Normally the hospital relies on Gulu Blood bank for transfusions, however the closure of schools and universities created a sudden vacuum in availability of blood which has heavily affected the entire country, as students are the main source of blood donations. Blood shortages can have lethal consequences, particularly for under-5 paediatric patients and for obstetric complications. -

Cahiers De La Méditerranée, 88 | 2014 Catholic Italy and Post-Colonial Africa: the New Subjects of an Informal Comm
Cahiers de la Méditerranée 88 | 2014 Le rapport au monde de l'Italie de la première guerre mondiale à nos jours Catholic Italy and Post-Colonial Africa: the New Subjects of an Informal Commitment in the 1960s Paolo Borruso Electronic version URL: http://journals.openedition.org/cdlm/7489 ISSN: 1773-0201 Publisher Centre de la Méditerranée moderne et contemporaine Printed version Date of publication: 30 June 2014 Number of pages: 99-111 ISSN: 0395-9317 Electronic reference Paolo Borruso, « Catholic Italy and Post-Colonial Africa: the New Subjects of an Informal Commitment in the 1960s », Cahiers de la Méditerranée [Online], 88 | 2014, Online since 31 October 2014, connection on 08 September 2020. URL : http://journals.openedition.org/cdlm/7489 This text was automatically generated on 8 September 2020. © Tous droits réservés Catholic Italy and Post-Colonial Africa: the New Subjects of an Informal Comm... 1 Catholic Italy and Post-Colonial Africa: the New Subjects of an Informal Commitment in the 1960s Paolo Borruso Vatican II, Italy and the “new Africa” 1 This paper focuses on an important aspect of Italy’s relations with Africa. In the early 1960s, the independence process in Africa posed new challenges to Italian foreign policy and also favored non-institutional actors who provided renewed momentum to the Vatican and a growing presence throughout the continent. Both traditional missions and the Catholic laity showed their commitment, and they worked together or individually, with different or shared inspirations and objectives. As the seat of the papacy, Italy as a “Catholic nation” has its own specificity and a noticeable presence of Catholicism throughout society. -

UG-08 24 A3 Fistula Supported Preventive Facilities by Partners
UGANDA FISTULA TREATMENT SERVICES AND SURGEONS (November 2010) 30°0'0"E 32°0'0"E 34°0'0"E Gulu Gulu Regional Referral Hospital Agago The Republic of Uganda Surgeon Repair Skill Status Kalongo General Hospital Soroti Ministry of Health Dr. Engenye Charles Simple Active Surgeon Repair Skill Status Dr. Vincentina Achora Not Active Soroti Regional Referral Hospital St. Mary's Hospital Lacor Surgeon Repair Skill Status 4°0'0"N Dr. Odong E. Ayella Complex Active Dr. Kirya Fred Complex Active 4°0'0"N Dr. Buga Paul Intermediate Active Dr. Bayo Pontious Simple Active SUDAN Moyo Kaabong Yumbe Lamwo Koboko Kaabong Hospital qÆ DEM. REP qÆ Kitgum Adjumani Hospital qÆ Kitgum Hospital OF CONGO Maracha Adjumani Hoima Hoima Regional Referral Hospital Kalongo Hospital Amuru Kotido Surgeon Repair Skill Status qÆ Arua Hospital C! Dr. Kasujja Masitula Simple Active Arua Pader Agago Gulu C! qÆ Gulu Hospital Kibaale Lacor Hospital Abim Kagadi General Hospital Moroto Surgeon Repair Skill Status Dr. Steven B. Mayanja Simple Active qÆ Zombo Nwoya qÆ Nebbi Otuke Moroto Hospital Nebbi Hospital Napak Kabarole Oyam Fort Portal Regional Referral Hospital Kole Lira Surgeon Repair Skill Status qÆ Alebtong Dr. Abirileku Lawrence Simple Active Lira Hospital Limited Amuria Dr. Charles Kimera Training Inactive Kiryandongo 2°0'0"N 2°0'0"N Virika General Hospital Bullisa Amudat HospitalqÆ Apac Dokolo Katakwi Dr. Priscilla Busingye Simple Inactive Nakapiripirit Amudat Kasese Kaberamaido Soroti Kagando General Hospital Masindi qÆ Soroti Hospital Surgeon Repair Skill Status Amolatar Dr. Frank Asiimwe Complex Visiting qÆ Kumi Hospital Dr. Asa Ahimbisibwe Intermediate Visiting Serere Ngora Kumi Bulambuli Kween Dr. -

International Criminal Court 1 Trial Chamber IX 2 Situation: Republic Of
ICC-02/04-01/15-T-102-Red-ENG WT 11-09-2017 1/88 NB T Trial Hearing (Open Session) ICC-02/04-01/15 1 International Criminal Court 2 Trial Chamber IX 3 Situation: Republic of Uganda 4 In the case of The Prosecutor v. Dominic Ongwen - ICC-02/04-01/15 5 Presiding Judge Bertram Schmitt, Judge Péter Kovács and 6 Judge Raul Cano Pangalangan 7 Trial Hearing - Courtroom 3 8 Monday, 11 September 2017 9 (The hearing starts in open session at 9.32 a.m.) 10 THE COURT USHER: [9:32:21] All rise. 11 The International Criminal Court is now in session. 12 PRESIDING JUDGE SCHMITT: [9:32:44] Good morning, everyone, and welcome 13 again in the courtroom after the longer break, so to speak. 14 Would the court officer please call the case. 15 THE COURT OFFICER: [9:32:56] Good morning, Mr President, your Honours. 16 Situation in the Republic of Uganda, in the case of The Prosecutor versus Dominic 17 Ongwen, case reference ICC-02/04-01/15. 18 And for the record we are in open session. 19 PRESIDING JUDGE SCHMITT: [9:33:13] Thank you very much. 20 I call for the appearances of the parties, Mr Bradfield. 21 MR BRADFIELD: [9:33:18] Good morning, Mr President and your Honours. 22 Appearing today for the Prosecution are Sanyu Ndagire, Benjamin Gumpert, 23 Colin Black, Yulia Nuzban, Colleen Gilg, Hai Do Duc, Yya Aragon, Shahriar Yeasin 24 Khan, Ramu Fatima Bittaye, and myself Paul Bradfield. 25 PRESIDING JUDGE SCHMITT: [9:33:41] Thank you. -

The Hydrogeology of Northern Agago County in Pader District, Uganda
The Hydrogeology of Northern Agago County in Pader District, Uganda Groundwater Programme Open Report OR/08/040 BRITISH GEOLOGICAL SURVEY GROUNDWATER PROGRAMME OPEN REPORT OR/08/040 The Hydrogeology of Northern Agago County in Pader District, Uganda Keywords M T Graham Groundwater; Uganda; Pader; Agago; hydrogeology; weathered basement. Latitude, Longitude SW corner 33.1305E, 2.7182N NE corner 33.6596E, 3.2992N Front cover View looking NNE from Parabong mountain, towards NE Parabongo and Paimol sub- counties Bibliographical reference GRAHAM, M. 2008. The Hydrogeology of Northern Agago County in Pader District, Uganda. British Geological Survey Internal Report, OR/08/040. 30pp. Copyright in materials derived from the British Geological Survey’s work is owned by the Natural Environment Research Council (NERC) and/or the authority that commissioned the work. You may not copy or adapt this publication without first obtaining permission. Contact the BGS Intellectual Property Rights Section, British Geological Survey, Keyworth, e-mail [email protected]. You may quote extracts of a reasonable length without prior permission, provided a full acknowledgement is given of the source of the extract. Maps and diagrams in this book use topography based on Ordnance Survey mapping. © NERC 2008. All rights reserved Keyworth, Nottingham British Geological Survey 2008 BRITISH GEOLOGICAL SURVEY The full range of our publications is available from BGS shops at British Geological Survey offices Nottingham, Edinburgh, London and Cardiff (Welsh publications only) see contact details below or shop online at www.geologyshop.com BGS Central Enquiries Desk 0115 936 3143 Fax 0115 936 3276 The London Information Office also maintains a reference email [email protected] collection of BGS publications including maps for consultation. -

Homestead Hygiene in Rural Uganda
HOMESTEAD HYGIENE IN RURAL UGANDA Erin Stephenson Masters of Science in Nursing Leadership Specialization in Public Health Nursing Northern Uganda- January 8-21, 2017 • St. Mary’s School of Midwifery • Kalongo, Uganda • January 12-18 • Ocer Campion Jesuit College • Gulu, Uganda • January 18-20 Uganda total population: 39,032,0005 I would like to thank Sister Carmel and Tutor Polly from St. Mary’s School of Midwifery and Father Tony and Nurse Susan from Ocer Campion for hosting our group and providing such excellent, immersive educational opportunities. Uganda Healthcare System • The Village Health Team Health Centre 1 (VHT) (VHT) concept was introduced in Uganda in Health Centre 2 2001 as part of a national health strategic plan. Health Centre 3 Health Centre 4 • VHTs are intended to bridge the gap between Regional un-served households and Hospital the formal health system. National They form the first level of Hospital Ugandan healthcare. Preparation Activities Immersion Activities • Developed Individual • VHT let community education Objectives session • Postpartum home visit • Group Meetings • Kalongo hospital rotations • Culture Hour • Community Development • Student Health Travel Officer interview Consultation • VHT presentation • Meeting with Tutor Polly • Homestead hygiene visit • Women’s waiting shelter visit • Literature Review • Maternal mortality lecture • Novels • Paimol Health Center 3 visit • Movies/Documentaries • Ocer Campion school • St. Jude’s orphanage Community Education Attendees at a community health education lesson -

Covid-19 Vaccination Sites by District In
COVID-19 VACCINATION SITES BY DISTRICT IN UGANDA Serial Number District/Division Service point Abim hospital Alerek HCIII 1 Abim Marulem HCIII Nyakwae HCIII Orwamuge HCIII Adjumani Hospital Dzaipi HCII 2 Adjumani Mungula HC IV Pakele HCIII Ukusijoni HC III Kalongo Hospital Lirakato HC III 3 Agago Lirapalwo HCIII Patongo HC III Wol HC III Abako HCIII Alebtong HCIV 4 Alebtong Amogo HCIII Apala HCIII Omoro HCIII Amolatar HC IV Aputi HCIII 5 Amolatar Etam HCIII Namasale HCIII Amai Hosp Amudat General Hospital Kalita HCIV 6 Amudat Loroo HCIII Cheptapoyo HC II Alakas HC II Abarilela HCIII Amuria general hospital 7 Amuria Morungatuny HCIII Orungo HCIII Wera HCIII Atiak HC IV Kaladima HC III 8 Amuru Labobngogali HC III Otwee HC III Pabo HC III Akokoro HCIII Apac Hospital 9 Apac Apoi HCIII Ibuje HCIII Page 1 of 16 COVID-19 VACCINATION SITES BY DISTRICT IN UGANDA Serial Number District/Division Service point Teboke HCIII AJIA HCIII Bondo HCIII 10 Arua Logiri HCIII Kuluva Hosp Vurra HCIII Iki-Iki HC III Kamonkoli HC III 11 Budaka Lyama HC III Budaka HC IV Kerekerene HCIII Bududa Hospital Bukalasi HCIII 12 Bududa Bukilokolo HC III Bulucheke HCIII Bushika HC III Bugiri Hospital BULESA HC III 13 Bugiri MUTERERE HC III NABUKALU HC III NANKOMA HC IV BUSEMBATYA HCIII BUSESA HC IV 14 Bugweri IGOMBE HC III LUBIRA HCIII MAKUUTU HC III Bihanga HC III Burere HC III 15 Buhweju Karungu HC III Nganju HC III Nsiika HC IV Buikwe HC III Kawolo Hospital 16 Buikwe Njeru HCIII Nkokonjeru Hospital Wakisi HC III Bukedea HC IV Kabarwa HCIII 17 Bukedea Kachumbala HCIII -

September 2020 Edition No. 2
September 2020 Edition no. 2 NEWS NO/NO 1 COMMA 1, ART. N.46) 27/02/2004 L. IN (CONV. 353/2003 D.L. – POSTALE ABBONAMENTO IN SPEDIZIONE – S.P.A. “We just have to stay here to share ITALIANE and to help as many people as POSTE possible." Father Giuseppe Ambrosoli EDITORIAL DEAR FRIENDS, As you can imagine, the past few months have been very demanding for us. Kalongo hospital has been suddenly “Africa is a land involved in the Covid-19 emergency. We immediately had to face the operational difficulties caused by the emergency. The of challanges that blockade of transports and shipping delayed the delivery of come one after medical materials and devices, necessary to face not only a possible Covid-19 epidemic, but above all the many daily another without emergencies, such as pneumonia, airborne infectious diseases and certainly malaria, which is affecting once again the little interruption and ones. In Uganda, the positive cases of Covid-19 are constantly that push us not to growing, even if they are much less compared to other give up, certain that countries. By the 2nd of September 3,037 confirmed infections and 32 deceased were registered. But the side effects of the we are doing the right emergency are what really scare us. thing. That is what In recent months in Kalongo the number of hospitalizations Father Giuseppe dropped dramatically. Due to the restrictive measures imposed by the government which made it difficult to reach the hospital, taught us to believe and to the fear of the population to contract the virus, the cases arriving at the hospital are serious and often fatal.