Auricular Vagus Neuromodulation – a Systematic Review on Quality of Evidence and Clinical Effects
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Instruction Sheet: Otitis Externa
University of North Carolina Wilmington Abrons Student Health Center INSTRUCTION SHEET: OTITIS EXTERNA The Student Health Provider has diagnosed otitis externa, also known as external ear infection, or swimmer's ear. Otitis externa is a bacterial/fungal infection in the ear canal (the ear canal goes from the outside opening of the ear to the eardrum). Water in the ear, from swimming or bathing, makes the ear canal prone to infection. Hot and humid weather also predisposes to infection. Symptoms of otitis externa include: ear pain, fullness or itching in the ear, ear drainage, and temporary loss of hearing. These symptoms are similar to those caused by otitis media (middle ear infection). To differentiate between external ear infection and middle ear infection, the provider looks in the ear with an instrument called an otoscope. It is important to distinguish between the two infections, as they are treated differently: External otitis is treated with drops in the ear canal, while middle ear infection is sometimes treated with an antibiotic by mouth. MEASURES YOU SHOULD TAKE TO HELP TREAT EXTERNAL EAR INFECTION: 1. Use the ear drops regularly, as directed on the prescription. 2. The key to treatment is getting the drops down into the canal and keeping the medicine there. To accomplish this: Lie on your side, with the unaffected ear down. Put three to four drops in the infected ear canal, then gently pull the outer ear back and forth several times, working the medicine deeper into the ear canal. Remain still, good-ear-side-down for about 15 minutes. -

Ear Infections
EAR INFECTIONS How common are ear infections in cats? Infections of the external ear canal (outer ear) by bacteria or yeast are common in dogs but not as common in cats. Outer ear infections are called otitis externa. The most common cause of feline otitis externa is ear mite infestation. What are the symptoms of an ear infection? Ear infection cause pain and discomfort and the ear canals are sensitive. Many cats will shake their head and scratch their ears attempting to remove the debris and fluid from the ear canal. The ears often become red and inflamed and develop an offensive odor. A black or yellow discharge is commonly observed. Don't these symptoms usually suggest ear mites? Ear mites can cause several of these symptoms including a black discharge, scratching and head shaking. However, ear mite infections generally occur in kittens. Ear mites in adult cats occur most frequently after a kitten carrying mites is introduced into the household. Sometimes ear mites will create an environment within the ear canal which leads to a secondary infection with bacteria or yeast. By the time the cat is presented to the veterinarian the mites may be gone but a significant ear infection remains. Since these symptoms are similar can I just buy some ear drops? No, careful diagnosis of the exact cause of the problem is necessary to enable selection of appropriate treatment. There are several kinds of bacteria and fungi that might cause an ear infection. Without knowing the kind of infection present, we do not know which drug to use. -

ANATOMY of EAR Basic Ear Anatomy
ANATOMY OF EAR Basic Ear Anatomy • Expected outcomes • To understand the hearing mechanism • To be able to identify the structures of the ear Development of Ear 1. Pinna develops from 1st & 2nd Branchial arch (Hillocks of His). Starts at 6 Weeks & is complete by 20 weeks. 2. E.A.M. develops from dorsal end of 1st branchial arch starting at 6-8 weeks and is complete by 28 weeks. 3. Middle Ear development —Malleus & Incus develop between 6-8 weeks from 1st & 2nd branchial arch. Branchial arches & Development of Ear Dev. contd---- • T.M at 28 weeks from all 3 germinal layers . • Foot plate of stapes develops from otic capsule b/w 6- 8 weeks. • Inner ear develops from otic capsule starting at 5 weeks & is complete by 25 weeks. • Development of external/middle/inner ear is independent of each other. Development of ear External Ear • It consists of - Pinna and External auditory meatus. Pinna • It is made up of fibro elastic cartilage covered by skin and connected to the surrounding parts by ligaments and muscles. • Various landmarks on the pinna are helix, antihelix, lobule, tragus, concha, scaphoid fossa and triangular fossa • Pinna has two surfaces i.e. medial or cranial surface and a lateral surface . • Cymba concha lies between crus helix and crus antihelix. It is an important landmark for mastoid antrum. Anatomy of external ear • Landmarks of pinna Anatomy of external ear • Bat-Ear is the most common congenital anomaly of pinna in which antihelix has not developed and excessive conchal cartilage is present. • Corrections of Pinna defects are done at 6 years of age. -

Anatomy of the Ear ANATOMY & Glossary of Terms
Anatomy of the Ear ANATOMY & Glossary of Terms By Vestibular Disorders Association HEARING & ANATOMY BALANCE The human inner ear contains two divisions: the hearing (auditory) The human ear contains component—the cochlea, and a balance (vestibular) component—the two components: auditory peripheral vestibular system. Peripheral in this context refers to (cochlea) & balance a system that is outside of the central nervous system (brain and (vestibular). brainstem). The peripheral vestibular system sends information to the brain and brainstem. The vestibular system in each ear consists of a complex series of passageways and chambers within the bony skull. Within these ARTICLE passageways are tubes (semicircular canals), and sacs (a utricle and saccule), filled with a fluid called endolymph. Around the outside of the tubes and sacs is a different fluid called perilymph. Both of these fluids are of precise chemical compositions, and they are different. The mechanism that regulates the amount and composition of these fluids is 04 important to the proper functioning of the inner ear. Each of the semicircular canals is located in a different spatial plane. They are located at right angles to each other and to those in the ear on the opposite side of the head. At the base of each canal is a swelling DID THIS ARTICLE (ampulla) and within each ampulla is a sensory receptor (cupula). HELP YOU? MOVEMENT AND BALANCE SUPPORT VEDA @ VESTIBULAR.ORG With head movement in the plane or angle in which a canal is positioned, the endo-lymphatic fluid within that canal, because of inertia, lags behind. When this fluid lags behind, the sensory receptor within the canal is bent. -
Audiometric Findings with Voluntary Tensor Tympani Contraction Brandon Wickens1 , Duncan Floyd2 and Manohar Bance3*
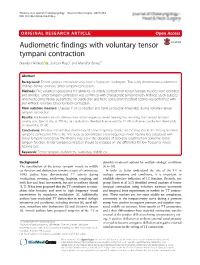
Wickens et al. Journal of Otolaryngology - Head and Neck Surgery (2017) 46:2 DOI 10.1186/s40463-016-0182-y ORIGINALRESEARCHARTICLE Open Access Audiometric findings with voluntary tensor tympani contraction Brandon Wickens1 , Duncan Floyd2 and Manohar Bance3* Abstract Background: Tensor tympani contraction may have a "signature" audiogram. This study demonstrates audiometric findings during voluntary tensor tympani contraction. Methods: Five volunteers possessing the ability to voluntarily contract their tensor tympani muscles were identified and enrolled. Tensor tympani contraction was confirmed with characteristic tympanometry findings. Study subjects underwent conventional audiometry. Air conduction and bone conduction threshold testing was performed with and without voluntary tensor tympani contraction. Main outcome measure: Changes in air conduction and bone conduction thresholds during voluntary tensor tympani contraction. Results: Audiometric results demonstrate a low frequency mixed hearing loss resulting from tensor tympani contraction. Specifically, at 250 Hz, air conduction thresholds increased by 22 dB and bone conduction thresholds increased by 10 dB. Conclusions: Previous research has demonstrated a low frequency conductive hearing loss in the setting of tensor tympanic contraction. This is the first study to demonstrate a low frequency mixed hearing loss associated with tensor tympani contraction. This finding may aid in the diagnosis of disorders resulting from abnormal tensor tympani function. Tensor tympani contraction -

Otosclerosis and Stapes Surgery | How to Prepare and What to Expect |
UW MEDICINE | PATIENT EDUCATION | | Otosclerosis and Stapes Surgery | How to prepare and what to expect | This handout explains otosclerosis, an ear problem that causes hearing loss. It also describes stapes surgery, which is done to improve hearing. What is otosclerosis? Otosclerosis (oh-toh-skleh-ROH-sis) is abnormal growth on the tiny stapes (stirrup) bone in your middle ear. This growth keeps the stapes from vibrating in response to sound. Otosclerosis is the most common cause of conductive hearing loss in adults. Conductive hearing loss is when sound waves cannot move normally in the ear (see DRAFTpage 3). At first, otosclerosis does not cause any symptoms. Hearing loss begins when the bone growth starts to affect how the stapes works. As the bone keeps growing, the Otosclerosis affects the stapes, a tiny hearing loss gets worse. bone in your middle ear. The good news is that hearing loss occurs in only 10% of people (10 out of 100) who have otosclerosis. Profound (severe) hearing loss and deafness are very rare. What causes otosclerosis? Otosclerosis can be hereditary, which means it may be passed from parents to their children. Someone in your family may have had the condition and passed it down to you. If you have otosclerosis, your children may inherit it. Hearing loss may not occur in all generations. The measles virus may affect whether or not you develop otosclerosis, but measles alone do not cause it. How is it treated? Your doctor may advise hearing aids or that you have stapes surgery to treat otosclerosis. Sometimes, both surgery and a hearing aid are needed. -

Let's Talk About . . . Otosclerosis
LET’S TALK ABOUT . OTOSCLEROSIS diagnosed with otosclerosis. Pregnancy can cause Key points otosclerosis to advance more quickly. • Otosclerosis affects the bones of the middle Otosclerosis is rare, affecting about 3 in 1,000 ear that conduct sound. people. Research suggests between 25 to 50% of people with otosclerosis have a family history of the • It is one of the most common causes of conductive hearing loss in young adults. condition. • How quickly, or to what extent, hearing will The word otosclerosis comes from Greek. It means be affected is unpredictable. abnormal hardening of body tissue (sclerosis) of the ear (oto). • If otosclerosis goes into the inner ear, you may be troubled by ringing in the ears, dizziness and balance problems. How do we hear? • Hearing aids are usually the preferred first treatment choice. To understand why otosclerosis causes hearing loss, it is important to have a basic understanding of how we hear. For hearing to function normally a What is otosclerosis? sound has to travel through all three parts of the Otosclerosis (oh-toe-skler-OH-suhs) a complex ear: outer, middle and inner. The first two are air disorder of abnormal bone growth in the middle ear. filled; the latter is fluid filled. It most often happens when the tiny stapes (“STAY- The outer ear is made up of the part you can see peez”) bone knits with surrounding bone. on the side of your head (pinna) and the funnel- Otosclerosis usually results in slow, shaped external ear canal. The pinna gathers progressive conductive hearing loss. sound waves (vibrations) and channels them When the stapes is unable to vibrate, hearing through the ear canal to the eardrum (tympanic becomes impaired. -
Endoscopic Treatment of Middle Ear Myoclonus with Stapedius and Tensor Tympani Section: a New Minimally-Invasive Approach
British Journal of Medicine & Medical Research 4(17): 3398-3405, 2014 SCIENCEDOMAIN international www.sciencedomain.org Endoscopic Treatment of Middle Ear Myoclonus with Stapedius and Tensor Tympani Section: A New Minimally-Invasive Approach Natasha Pollak1*, Roya Azadarmaki2 and Sidrah Ahmad1 1Department of Otolaryngology–Head and Neck Surgery, Temple University School of Medicine, Philadelphia, Pennsylvania, USA. 2Metropolitan NeuroEar Group, Rockville, Maryland, USA. Authors’ contributions This work was carried out in collaboration between all authors. Author NP designed study, performed surgery, literature review, writing, reviewing. Author RA literature review, writing, reviewing. Author SA performed surgery, writing, reviewing. All authors read and approved the final manuscript. Received 26th January 2014 th Case Study Accepted 11 March 2014 Published 27th March 2014 ABSTRACT Aims: We describe a new, entirely endoscopic surgical technique for treatment of middle ear myoclonus. Case Presentation: In our patient, the stapedius and tensor tympani tendons were sectioned to control chronic middle ear myoclonus. The procedure was performed using endoscopic ear surgery techniques, with the aid of rigid Hopkins rod endoscopes. Control of the pulsatile tinnitus was achieved after endoscopic tenotomy of the stapedius and tensor tympani, without any complications. Discussion and Conclusion: Endoscopic tensor tympani and stapedius tendon section is a new, minimally invasive treatment option for middle ear myoclonus that should be considered as a first line surgical approach in patients who fail medical therapy. The use of an endoscopic approach allows for easier access and vastly superior visualization of the relevant anatomy, which in turn allows the surgeon to minimize dissection of healthy tissue for exposure. The entire operation, including raising the tympanomeatal flap and tendon section can be safely completed under visualization with a rigid endoscope with good control of the pulsatile tinnitus. -

Anatomy of the Ear
Lakeshore Ear, Nose & Throat Center, PC (586) 779-7610 www.lakeshoreent.com Anatomy of the Ear The temporal bone houses the structure commonly known as the ear. The temporal bone consists of an outer bony structure that is part of the skull and part of the skull base. It meets with several other bones that are part of the skull and the skull base. Within the temporal bone and at its varied boundaries are noted the carotid artery which goes up into the base of the temporal bone, courses through it and exits up at the front of the temporal bone to proceed on to give blood to the central nervous system. The jugular vein which takes the blood back from the brain area exits at the temporal bone lower level and courses through and indents a portion of the temporal bone (see figure 1). In regard to what is commonly felt to be the ear, there is an outer ear, a middle ear and an inner ear. Taking the outer ear first, we see the pinna or the ear cosmetically speaking, which resides on the lateral temporal bone. It leads to the external auditory canal which is part of the outer ear structure. That canal is skin lined and ends at the Lakeshore Ear, Nose & Throat Center, PC (586) 779-7610 www.lakeshoreent.com tympanic membrane, or eardrum, the outer surface of which is skin lined. The tympanic membrane has a middle portion, which is fibrous tissue and an inner layer which is mucous membrane, the same sort of mucous membrane, generally speaking, as occurs in the rest of the airway, including the sinuses and the lungs. -

Senses Sensory Receptors • Part of the Nervous System That Detects A
Topic 11: Senses Sensory Receptors Part of the nervous system that detects a stimulus A sensory receptor could be: o o o Types of Sensory Receptors: o Chemoreceptors: detects chemicals ( ) o Photoreceptors: detects light (found in ) o Thermoreceptors: detects changes in . Bulb of Krause: sensitive to temperatures o Mechanoreceptors: detect movement ( ) . Meissner’s corpuscles: sensitive to . Pacinian corpuscles: sensitive to . Ruffini corpuscles: senses changes in o Pain receptors ( ): detects tissue damage o Osmoreceptors: detects changes in the Sense of Touch: o Tactile corpuscles: touch receptors found in the of skin and around hair follicles Senses of pressure: located in tissues beneath the skin, near joints, muscles and other deep tissues Sense of Temperature: free nerve endings found distributed within the skin o Separate receptors for hot and cold Sense of Position o Propioceptors: receptors that maintain muscle tone and good posture in order to coordinate movements Sense of Pain o o o o o How Pain is Perceived How to Manage Pain Endorphins: naturally released chemicals that impair the flow of pain signals Aspirin: slows the production of pain signaling molecules Morphine: mimics endorphins Sense of Taste Taste: chemoreceptors that detect chemicals dissolved in fluid (tastebuds) Five Main Flavors: o o o o o Sense of Smell (Olfaction) Chemoreceptors that bind to specific substances Olfactory nerve carries impulses from the smell receptors to the and Vomeronasal organ: sensitive to Sense of Sight Protected by: o o o o o Structure of the Eye o Outer layer: . Sclera: . Cornea: o Middle layer: . Pupil: . Iris: . Cilary body: . Choroid: o Inner layer: . Lens: . -

The Physics of Hearing: Fluid Mechanics and the Active Process of the Inner Ear
The physics of hearing: fluid mechanics and the active process of the inner ear Tobias Reichenbach* and A. J. Hudspeth Howard Hughes Medical Institute and Laboratory of Sensory Neuroscience, The Rockefeller University, New York, NY 10065-6399, USA E-mail: [email protected] and [email protected] Running head: The physics of hearing Abstract Most sounds of interest consist of complex, time-dependent admixtures of tones of diverse frequencies and variable amplitudes. To detect and process these signals, the ear employs a highly nonlinear, adaptive, real-time spectral analyzer: the cochlea. Sound excites vibration of the eardrum and the three miniscule bones of the middle ear, the last of which acts as a piston to initiate oscillatory pressure changes within the liquid-filled chambers of the cochlea. The basilar membrane, an elastic band spiraling along the cochlea between two of these chambers, responds to these pressures by conducting a largely independent traveling wave for each frequency component of the input. Because the basilar membrane is graded in mass and stiffness along its length, however, each traveling wave grows in magnitude and decreases in wavelength until it peaks at a specific, frequency-dependent position: low frequencies propagate to the cochlear apex, whereas high frequencies culminate at the base. The oscillations of the basilar membrane deflect hair bundles, the mechanically sensitive organelles of the ear's sensory receptors, the hair cells. As mechanically sensitive ion channels open and close, each hair cell responds with an electrical signal that is chemically transmitted to an afferent nerve fiber and thence into the brain. -

A Multisensory Effect on the Mechanics of Hearing
The eardrums move when the eyes move: A PNAS PLUS multisensory effect on the mechanics of hearing Kurtis G. Grutersa,b,c,1, David L. K. Murphya,b,c,1, Cole D. Jensona,b,c, David W. Smithd, Christopher A. Sherae,f, and Jennifer M. Groha,b,c,2 aDepartment of Psychology and Neuroscience, Duke University, Durham, NC 27708; bDepartment of Neurobiology, Duke University, Durham, NC 27708; cDuke Institute for Brain Sciences, Duke University, Durham, NC 27708; dProgram in Behavioral and Cognitive Neuroscience, Department of Psychology, University of Florida, Gainesville, FL 32611; eCaruso Department of Otolaryngology, University of Southern California, Los Angeles, CA 90033; and fDepartment of Physics and Astronomy, University of Southern California, Los Angeles, CA 90033 Edited by Peter L. Strick, University of Pittsburgh, Pittsburgh, PA, and approved December 8, 2017 (received for review October 19, 2017) Interactions between sensory pathways such as the visual and (reviewed in refs. 18–20), allowing the brain to adjust the cochlear auditory systems are known to occur in the brain, but where they encoding of sound in response to previous or ongoing sounds in first occur is uncertain. Here, we show a multimodal interaction either ear and based on global factors, such as attention (21–27). evident at the eardrum. Ear canal microphone measurements in The collective action of these systems can be measured in real humans (n = 19 ears in 16 subjects) and monkeys (n = 5earsin time with a microphone placed in the ear canal (28). We used this three subjects) performing a saccadic eye movement task to visual technique to study whether the brain sends signals to the auditory targets indicated that the eardrum moves in conjunction with the periphery concerning eye movements, the critical information eye movement.