Preparing for a Colonoscopy Frequently Asked Questions
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Diagnostic Direct Laryngoscopy, Bronchoscopy & Esophagoscopy
Post-Operative Instruction Sheet Diagnostic Direct Laryngoscopy, Bronchoscopy & Esophagoscopy Direct Laryngoscopy: Examination of the voice box or larynx (pronounced “lair-inks”) under general anesthesia. An instrument called a laryngoscope is carefully placed into the mouth and used to visualize the larynx and surrounding structures. Bronchoscopy: Examination of the windpipe below the voice box in the neck and chest under general anesthesia. A long narrow telescope is passed through the larynx and used to carefully inspect the structures of the trachea and bronchi. Esophagoscopy: Examination of the swallowing pipe in the neck and chest under general anesthesia. An instrument called an esophagoscope is passed into the esophagus (just behind the larynx and trachea) and used to visualize the mucus membranes and surrounding structures of the esophagus. Frequently a small biopsy is taken to evaluate for signs of esophageal inflammation (esophagitis). What to Expect: Diagnostic airway endoscopy procedures generally take about 45 minutes to complete. Usually the procedure is well-tolerated and the child is back-to-normal the next day. Mild throat or tongue discomfort may persist for a few days after the procedure and is usually well-controlled with over-the-counter acetaminophen (Tylenol) or ibuprofen (Motrin). Warning Signs: Contact the office immediately at (603) 650-4399 if any of the following develop: • Worsening harsh, high-pitched noisy-breathing (stridor) • Labored breathing with chest retractions or flaring of the nostrils • Bluish discoloration of the lips or fingernails (cyanosis) • Persistent fever above 102°F that does not respond to Tylenol or Motrin • Excessive coughing or respiratory distress during feeding • Coughing or throwing up bright red blood • Excessive drowsiness or unresponsiveness Diet: Resume baseline diet (no special postoperative diet restrictions). -
Laryngeal Endoscopy (Rigid, Flexible, and Stroboscopy)
Laryngeal Endoscopy (Rigid, Flexible, and Stroboscopy) Visualization of the larynx can be performed via several different methods. Special tools are required for laryngeal evaluation. Mirror laryngoscopy (1) o While the patient’s tongue is protruded, a mirror is placed in the posterior oropharynx with gentle pressure on the soft palate while light is reflected caudally into the larynx. o Mirror laryngoscopy can be challenging for both the examiner and the patient, has limited magnification, and may require topical anesthesia. o Mirror laryngoscopy provides the most accurate color representation of laryngeal and pharyngeal tissue because there is no light or digital distortion. Flexible laryngoscopy (2) o A flexible laryngoscope is placed into the nasal cavity, through the naso- and oropharynx and positioned cephalad to the larynx for a full laryngeal assessment. o Nasal anesthesia (lidocaine) and/or nasal decongestants (oxymetazoline/phenylephrine) may be applied to the nose for the purpose of improving patient comfort and tolerance o Supplemental procedures such as dynamic voice assessment (comprehensive laryngeal movement evaluation), functional endoscopic evaluation of swallowing (+/- sensory testing), and other laryngeal procedures (ex. injections, laser surgery, biopsies) can be performed during flexible laryngoscopy. o Flexible laryngoscopy is ideal for evaluating vocal fold weakness, real-time/unencumbered evaluation of task-specific abnormalities (ex. my voice is problematic when I do this), and assessing the intensity of glottal attack. Rigid Laryngoscopy (3) o Rigid laryngoscopy is performed by placing a rigid 70- or 90-degree telescope into the oropharynx during tongue protrusion. o Sometimes, oropharyngeal and/or tongue application of anesthesia (ex. lidocaine, cetacaine) can be helpful for patient tolerance. -
Flexible Sigmoidoscopy – Outpatients
Flexible sigmoidoscopy – Outpatients You have been referred by your doctor to have a flexible sigmoidoscopy. his information booklet has been written to explain the procedure. This will help you to make an informed decision before consenting to the procedure. If you are unable to attend your appointment please inform us as soon as possible. Please ensure you read this booklet and the enclosed consent form thoroughly. Please also complete the enclosed health questionnaire. You may be contacted by an endoscopy trained nurse before your procedure to go through the admission process and answer any queries you may have. If you are not contacted please come to your appointment at the time stated in your letter. Please note your appointment time is your arrival time on the unit and not the time of your procedure. If you have any mobility issues or if there is a possibility you could be pregnant, please contact the appointment staff on 01284 713551 Please remember there will be other patients in the unit who may arrive after you but are taken in for their procedure before you, this is for medical reasons or they are seeing a different doctor. Due to limited space available and to maintain other patients’ privacy and dignity, we only allow patients (and carers) through to the ward area. Relatives/ escorts will be contacted once you are ready for collection. The Endoscopy Unit endeavours to offer single sex facilities, and we aim to make you stay as comfortable and stress free as possible. Source: Endoscopy Reference No: 5035-14 Issue date: 8/1/21 Review date: 8/1/24 Page 1 of 11 Medication If you are taking WARFARIN, CLOPIDOGREL, RIVAROXABAN or any other anticoagulant (blood thinning medication), please contact the appointment staff on 01284 713551, your GP or anticoagulation nurse, as special arrangements may be necessary. -

SPECIALTY CARE Digestive Health
SPECIALTY CARE Digestive Health Through our Day Kimball Medical Group A lot of people care about your health. Including us. So if you’re 45 or practices and other associated specialty over and due for a colon screening, you should know that Day Kimball physicians, Day Kimball Healthcare has one of the most comprehensive digestive health programs around. provides you access to expert specialized care for virtually every body system Gastroenterology deals with the function, diseases and disorders of and condition, within an integrated and the digestive system, including the esophagus, stomach, pancreas, gall coordinated approach. bladder, bile ducts, liver, small intestine, colon (or large intestine), and rectum. Most everyone will need specialized care at some point in life. It’s good to know Physician Consultations that when that time comes you’ll have Consults for advanced treatment of digestive and liver disorders are access to physicians and facilities focused available through our associated board-certified gastroenterologists solely on providing you with top-notch from Connecticut GI. A referral from your primary care practitioner specialized care, close to home. (PCP) is required. Day Kimball Healthcare offers integrated, comprehensive care Endoscopy Services With our state-of-the-art Doris E. Madeira Endoscopy Suite at Day close to home. To learn more Kimball Hospital and the services of our associated gastroenterologists about all of our specialty from Connecticut GI, we are able to offer comprehensive screening, medical services -

Antibiotic Prophylaxis for GI Endoscopy
GUIDELINE Antibiotic prophylaxis for GI endoscopy This is one of a series of statements discussing the use of procedure. Endoscopy-related bacteremia carries a small GI endoscopy in common clinical situations. The Stan- risk of localization of infection in remote tissues (ie, infec- dards of Practice Committee of the American Society for tive endocarditis [IE]). Endoscopy also may result in local Gastrointestinal Endoscopy (ASGE) prepared this docu- infections in which a typically sterile space or tissue is ment, and it updates a previously issued document on breached and contaminated by an endoscopic accessory this topic.1 In preparing this guideline, MEDLINE and or by contrast material injection. This document is an up- PubMed databases were used to search for publications date of the prior ASGE document on antibiotic prophylaxis between January 1975 and December 2013 pertaining for GI endoscopy,1 discusses infectious adverse events to this topic. The search was supplemented by accessing related to endoscopy, and provides recommendations for the “related articles” feature of PubMed, with articles periprocedural antibiotic therapy. identified on MEDLINE and PubMed as the references. Additional references were obtained from the bibliogra- phies of the identified articles and from recommenda- BACTEREMIA ASSOCIATED WITH tions of expert consultants. When few or no data were ENDOSCOPIC PROCEDURES available from well-designed prospective trials, emphasis was given to results from large series and reports from Bacteremia can occur after endoscopic procedures and has been advocated as a surrogate marker for IE risk. How- recognized experts. Weaker recommendations are indi- fi cated by phrases such as “We suggest.” whereas stronger ever, clinically signi cant infections are extremely rare. -
Overview of Endoscopy and Laparoscopy
Overview of Endoscopy and Laparoscopy Hideto Yokoi Department of Medical Informatics Kagawa University Hospital Two types of image interpretation • Interpretation retrospectively – Many of Radiology images – Capsule endoscopy – Pathology? • Interpretation based on real time motion picture – Flexible Endoscopy, Laparoscopy – Ultrasonography – Pathology? – Some of Radiology images (Cardiac Intervention) – Observation modalities of Ophthalmology / Otorhinolaryngology / Gynecology… What is “gold standard” in endoscopy diagnosis • In screening endoscopy, we often perform biopsies. – Get specimens from lesion. – Pathological study will be performed after biopsy. – It is “gold standard” of distinguishing between benign and malignant. The Workflow of Radiology Radiologist Ordering RIS PACS Report System DB Order for Report Study Rd Physician Radiological Technician Pt Pt Pt Order and Reservation Image Acquisition Outpatient Service after the study The Workflow of Endoscopy Pathology Dpt. Pathology Ordering Endoscopy PACS Report System System DB System Order for Order of Pathological Study Study Result Ns Physician Endoscopist Pt Pt Pt Pt Order and Outpatient Service Pre-medication Endoscopy Study Reservation after the study Difference between Endoscopy and Laparoscopy • The difference depends on – presence or absence of “idea of original scene”. • Endoscopists do not know “original scene” of lumen of GI tracts because they cannot observe the “live lumen” of GI tracts directly with their eyes – When we cut and open the tracts, they may not be “live”. • Surgeons can observe the organs directly at open surgery. – Thus, they can discuss the “original scene”. Difference between Two Gastroenterological Endoscopies • Flexible endoscopy – Endoscopist can observe a lesion with real time image, using some invasive devices. • To check an elasticity of a lesion • To see a shape change of a lesion, using devices • Capsule endoscopy – Image interpretation is completely retrospective. -

Icd-9-Cm (2010)
ICD-9-CM (2010) PROCEDURE CODE LONG DESCRIPTION SHORT DESCRIPTION 0001 Therapeutic ultrasound of vessels of head and neck Ther ult head & neck ves 0002 Therapeutic ultrasound of heart Ther ultrasound of heart 0003 Therapeutic ultrasound of peripheral vascular vessels Ther ult peripheral ves 0009 Other therapeutic ultrasound Other therapeutic ultsnd 0010 Implantation of chemotherapeutic agent Implant chemothera agent 0011 Infusion of drotrecogin alfa (activated) Infus drotrecogin alfa 0012 Administration of inhaled nitric oxide Adm inhal nitric oxide 0013 Injection or infusion of nesiritide Inject/infus nesiritide 0014 Injection or infusion of oxazolidinone class of antibiotics Injection oxazolidinone 0015 High-dose infusion interleukin-2 [IL-2] High-dose infusion IL-2 0016 Pressurized treatment of venous bypass graft [conduit] with pharmaceutical substance Pressurized treat graft 0017 Infusion of vasopressor agent Infusion of vasopressor 0018 Infusion of immunosuppressive antibody therapy Infus immunosup antibody 0019 Disruption of blood brain barrier via infusion [BBBD] BBBD via infusion 0021 Intravascular imaging of extracranial cerebral vessels IVUS extracran cereb ves 0022 Intravascular imaging of intrathoracic vessels IVUS intrathoracic ves 0023 Intravascular imaging of peripheral vessels IVUS peripheral vessels 0024 Intravascular imaging of coronary vessels IVUS coronary vessels 0025 Intravascular imaging of renal vessels IVUS renal vessels 0028 Intravascular imaging, other specified vessel(s) Intravascul imaging NEC 0029 Intravascular -

Adverse Events of Upper GI Endoscopy
GUIDELINE Adverse events of upper GI endoscopy This is one of a series of statements discussing the use of lications rely on self-reporting, and most reported data GI endoscopy in common clinical situations. The Stan- collected only from the immediate periprocedure period, dards of Practice Committee of the American Society for thus the rate of late adverse events and mortality may be Gastrointestinal Endoscopy (ASGE) prepared this text. underestimated.8,9 Major adverse events related to diag- In preparing this document, a search of the medical liter- nostic UGI endoscopy are rare and include cardiopulmo- ature was performed by using PubMed. Additional refer- nary adverse events, infection, perforation, and bleeding. ences were obtained from the bibliographies of the identi- Adverse events of ERCP and EUS are discussed in separate fied articles and from recommendations of expert ASGE documents.10,11 consultants. When few or no data exist from well-designed prospective trials, emphasis is given to results of large series and reports from recognized experts. This document is ADVERSE EVENTS ASSOCIATED WITH based on a critical review of the available data and expert DIAGNOSTIC UGI ENDOSCOPY consensus at the time that the document was drafted. Further controlled clinical studies may be needed to clar- Cardiopulmonary adverse events ify aspects of this document. This document may be re- Most UGI procedures in the United States and Europe vised as necessary to account for changes in technology, are performed with patients under sedation (moderate or 12 new data, or other aspects of clinical practice. deep). Cardiopulmonary adverse events related to seda- This document is intended to be an educational device tion and analgesia account for as much as 60% of UGI 1-4,7 to provide information that may assist endoscopists in endoscopy adverse events. -

Automatic Classification of Digestive Organs in Wireless Capsule
Automatic Classification of Digestive Organs in Wireless Capsule Endoscopy Videos Jeongkyu Lee1, JungHwan Oh2, Subodh Kumar Shah1, Xiaohui Yuan2, Shou Jiang Tang3 1Dept. Comp. Sci. & Eng. 2Dept. Comp. Sci. & Eng. 3Division of Digestive Diseases University of Bridgeport University of North Texas UTSW Medical Center Bridgeport, CT 06604 Denton, TX 76203 Dallas, TX 75390 fjelee,[email protected] fjhoh,[email protected] [email protected] ABSTRACT A human digestive system consists of a series of several Wireless Capsule Endoscopy (WCE) allows a physician to di®erent organs including the esophagus, stomach, small in- examine the entire small intestine without any surgical op- testinal (i.e., duodenum, jejunum, and ileum) and colon. eration. With the miniaturization of wireless and camera Standard endoscopy has been playing a very important role technologies the ability comes to view the entire gestational as a diagnostic tool for the digestive tract. For example, track with little e®ort. Although WCE is a technical break- various endoscopies such as gastroscopy, push enteroscopy through that allows us to access the entire intestine without colonoscopy have been used for the visualization of digestive surgery, it is reported that a medical clinician spends one system. However, all methods mentioned above are limited or two hours to assess a WCE video. It limits the number in viewing small intestine. To address the problem, Wire- of examinations possible, and incur considerable amount of less Capsule Endoscopy (WCE) was ¯rst proposed in 2000, costs. To reduce the assessment time, it is critical to develop which integrates wireless transmission with image and video a technique to automatically discriminate digestive organs technology [13, 2, 1, 12, 14, 8]. -

Endoscopy on a Human Cadaver: a Feasibility Study As a Training Tool Avinash Bhat Balekuduru, Amit Kumar Dutta1, Satyaprakash Bonthala Subbaraj
Published online: 2019-09-24 Original Article Endoscopy on a Human Cadaver: A Feasibility Study as a Training Tool Avinash Bhat Balekuduru, Amit Kumar Dutta1, Satyaprakash Bonthala Subbaraj Department of Background: Simulation device and porcine models are increasingly being Gastroenterology, MS CT A used for training in gastrointestinal endoscopy. However reports on the use of Ramaiah Memorial Hospitals, Bengaluru, human cadaver for training in diagnostic or therapeutic endoscopy are limited. BSTR 1 Method: Human cadavers were preserved at our center in a customized non Karnataka, Department A of Gastroenterology, formalin based solution which retains organoleptic properties (preserves the Christian Medical College colour, feel, inflation of gut). We studied the feasibility of using these cadavers for and Hospitals, Vellore, training in endoscopy. Endoscopy was performed using PENTAX/ EP 2940 with Tamil Nadu, India a light source processor PENTAX/EPM 3500. Participants performed endoscopy and submucosal injection on cadaver as well as simulator. Before and after simulator and cadaver training, attendees completed a questionnaire on intubation, manoeuvring esophagus, stomach and duodenum for diagnostic endoscopy and scope positioning, needle out, submucosal injection and elevation of mucosa and needle in. The steps of ESD- marking, precut and submucosal dissection were attempted on the stomach of human cadaver. Results: Ten participants with very little prior experience of endoscopy felt the cadaver based training more beneficial in obtaining the sub mucosal plane and positioning the needle for four quadrant injection as compared to the endoscopic simulator (ES). The attendees felt that while ES has the advantage of providing feedback for the procedure, training on cadaver gave more realistic tactile experience and feel of the elasticity of the gut wall. -
ENDOSCOPY We Provide Comprehensive Care to You and Your Pet Through the Integration of Science, Compassion, and Integrity
ENDOSCOPY We provide comprehensive care to you and your pet through the integration of science, compassion, and integrity. CAMPBELL 907 Dell Avenue Phone: (408) 343-7243 Fax: (408) 385-3680 CONCORD SAGE doctors use rhinoscopy to remove foxtails and other foreign bodies from the nose. 1410 Monument Boulevard Phone: (925) 627-7243 Fax: (925) 771-1181 Rhinoscopy/Laryngoscopy DUBLIN Rhinoscopy and laryngoscopy may be recommended by 7121 Amador Plaza Road specialists to evaluate the nose and/or larynx. Phone: (925) 574-7243 Our rhinoscopes enable extensive evaluation of the nasal Fax: (925) 771-3043 passages for inflammation, fungal disease, and tumors— especially in conjunction with a CT scan. SAGE doctors also are able to remove inhaled foreignShoulder bodies, arthroscopy such as REDWOOD CITY foxtails, using these scopes. 934 Charter Street Phone: (650) 417-7243 Fax: (650) 344-4714 Other Types of Endoscopy: Cystoscopy Rigid cystoscopes allow our doctors to evaluate the Endoscopy urinary tract, including the bladder and urethra. Cystoscopy can be used to look for polyps, stones, tumors, and even ectopic ureters. Vaginoscopy SAGE doctors use a rigid scope to evaluate the vaginal tract for abnormalities or disease. They can even perform transcervical inseminations for breeding patients. www.sagecenters.com Bronchoscopy/Tracheoscopy What is endoscopy? Endoscopy utilizes an endoscope, or fiber-optic tubular instrument, to evaluate the internal Bronchoscopy and structures of the body via a lighted miniature camera. It is a minimally invasive procedure performed tracheoscopy allow SAGE by doctors who have undergone specialized training with this equipment. Our specialists are able to specialists to view and visualize structures, such as body cavities or organs, in magnified form through an eyepiece or on a evaluate a pet’s lower and monitor. -
Understanding Flexible Sigmoidoscopy
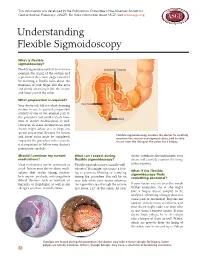
This information was developed by the Publications Committee of the American Society for Gastrointestinal Endoscopy (ASGE). For more information about ASGE, visit www.asge.org. Understanding Flexible Sigmoidoscopy What is flexible sigmoidoscopy? Flexible sigmoidoscopy lets your doctor SIGMOID COLON examine the lining of the rectum and a portion of the colon (large intestine) by inserting a flexible tube about the thickness of your finger into the anus and slowly advancing it into the rectum and lower part of the colon. What preparation is required? Your doctor will tell you what cleansing RECTUM routine to use. In general, preparation consists of one or two enemas prior to the procedure but could include laxa- ANUS tives or dietary modifications as well. However, in some circumstances your doctor might advise you to forgo any special preparation. Because the rectum Flexible sigmoidoscopy enables the doctor to carefully and lower colon must be completely examine the rectum and sigmoid colon, and to take empty for the procedure to be accurate, tissue from the lining of the colon for a biopsy. it is important to follow your doctor’s instructions carefully. Should I continue my current What can I expect during doctor withdraws the instrument, your medications? flexible sigmoidoscopy? doctor will carefully examine the lining Most medications can be continued as Flexible sigmoidoscopy is usually well- of the intestine. usual. Inform your doctor about medi- tolerated. You might experience a feel- What if the flexible cations that you’re taking, particu- ing of pressure, bloating or cramping sigmoidoscopy finds larly aspirin products, anti-coagulants during the procedure.