THE MORPHOLOGY, TERMINOLOGX, and PATHOGENESIS of ARTERIAL PLAQUES C.Uj
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Documentationand Coding Tips: Peripheral Vascular Disease
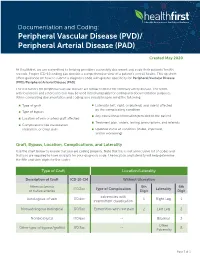
Documentation and Coding: Peripheral Vascular Disease (PVD)/ Peripheral Arterial Disease (PAD) Created May 2020 At Healthfirst, we are committed to helping providers accurately document and code their patients’ health records. Proper ICD-10 coding can provide a comprehensive view of a patient’s overall health. This tip sheet offers guidance on how to submit a diagnosis code with greater specificity for Peripheral Vascular Disease (PVD)/Peripheral Arterial Disease (PAD). The risk factors for peripheral vascular disease are similar to those for coronary artery disease. The terms arteriosclerosis and atherosclerosis may be used interchangeably for coding and documentation purposes. When completing documentation and coding, you should keep in mind the following: Type of graft Laterality (left, right, or bilateral) and side(s) affected by the complicating condition Type of bypass Any educational information provided to the patient Location of vein or artery graft affected Treatment plan, orders, testing, prescriptions, and referrals Complications like claudication, ulceration, or chest pain Updated status of condition (stable, improved, and/or worsening) Graft, Bypass, Location, Complications, and Laterality Use the chart below to ensure that you are coding properly. Note that this is not an inclusive list of codes and that you are required to have six digits for your diagnosis code. The location and laterality will help determine the fifth and sixth digits for the codes. Type of Graft Location/Laterality Description of Graft ICD-10-CM Without -

Association Between Multi-Site Atherosclerotic Plaques and Systemic Arteriosclerosis
Association between multi-site atherosclerotic plaques and systemic arteriosclerosis: results from the BEST study (Beijing Vascular Disease Patients Evaluation Study) huan liu Peking University Shougang Hospital https://orcid.org/0000-0001-6223-7677 Jinbo Liu Peking University Shougang Hospital Wei Huang Peking University Shougang Hospital Hongwei Zhao Peking University Shougang Hospital Na zhao Peking University Shougang Hospital Hongyu wang ( [email protected] ) Research Keywords: arteriosclerosis, atherosclerosis, atherosclerotic plaque, carotid femoral artery pulse wave velocity CF-PWV Posted Date: June 8th, 2020 DOI: https://doi.org/10.21203/rs.3.rs-31641/v1 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License Version of Record: A version of this preprint was published on August 1st, 2020. See the published version at https://doi.org/10.1186/s12947-020-00212-3. Page 1/18 Abstract Background Arteriosclerosis can be reected in various aspect of the artery, including atherosclerotic plaque formation or stiffening on the arterial wall. Both arteriosclerosis and atherosclerosis are important and closely associated with cardiovascular disease (CVD). The aim of the study was to evaluate the association between systemic arteriosclerosis and multi-site atherosclerotic plaques. Methods The study was designed as an observational cross-sectional study. A total of 1178 participants (mean age 67.4 years; 52.2% male) enrolled into the observational study from 2010 to 2017. Systemic arteriosclerosis was assessed by carotid femoral artery pulse wave velocity (CF-PWV) and multi-site atherosclerotic plaques (MAP, >=2 of the below sites) were reected in the carotid or subclavian artery, abdominal aorta and lower extremities arteries using ultrasound equipment. -

The Level of C.Pneumoniae, Cytomegalovirus, and H.Pylori Antibody in a Patient with Coronary Heart Disease
Vol 11, No 4, October – December 2002 Microorganism antibodies in CHD patient 211 The level of C.pneumoniae, Cytomegalovirus, and H.pylori antibody in a patient with coronary heart disease Dasnan Ismail Abstrak Aterosklerosis sampai saat ini merupakan penyebab utama morbiditas dan mortalitas di negara maju. Meskipun modifikasi faktor risiko di negara maju telah dapat menurunkan kekerapan aterosklerosis namun penurunan ini mulai menunjukkan grafik yang mendatar. Keadaan ini merangsang para peneliti untuk mencari faktor pajanan lingkungan termasuk faktor infeksi yang dapat mempengaruhi proses aterosklerosis. Telah dilakukan penelitian potong lintang dari bulan Maret 1998 sampai Agustus 1998 terhadap 122 orang pasien yang secara klinis menunjukkan penyakit jantung koroner yang menjalani kateterisasi jantung, terdiri dari 92 orang laki-laki dan 30 orang perempuan dengan rerata umur 55 tahun. Pasien diperiksa secara klinis dan laboratorium (gula darah, kolesterol, trigliserida dan antibodi terhadap C.pneumoniae, Cytomegalovirus dan H.pylori). Pada penelitian ini didapatkan perbedaan kadar kolesterol, trigliserida dan HDL antara kelompok stenosis koroner dan non stenosis. Sedangkan kadar antibodi C.pneumoniae, Cytomegalovirus, H.pylori tidak berbeda bermakna. Penelitian ini belum dapat menyimpulkan pengaruh antibodi terhadap aterosklerosis karena pada kelompok non stenosis tidak dapat disingkirkan kemungkinan terjadinya aterosklerosis mengingat rerata umur subyek penelitian 55 tahun. Penelitian mengenai interaksi infeksi dengan risiko tradisional serta gender dan nutrisi diperlukan untuk mendapat jawaban yang lebih jelas tentang pengaruh infeksi terhadap aterosklerosis. (Med J Indones 2002; 11: 211-4) Abstract Atherosclerosis is still the chief cause of morbidity and mortality in developed nations. Even though in developed nations the modification of risk factors is able to reduce the prevalence rate of atherosclerosis, such reduction is starting to slow down. -

Prehypertension Increases the Risk for Renal Arteriosclerosis in Autopsies: the Hisayama Study
JASN Express. Published on June 20, 2007 as doi: 10.1681/ASN.2007010067 CLINICAL EPIDEMIOLOGY www.jasn.org Prehypertension Increases the Risk for Renal Arteriosclerosis in Autopsies: The Hisayama Study Toshiharu Ninomiya,* Michiaki Kubo,* Yasufumi Doi,† Koji Yonemoto,* Yumihiro Tanizaki,* Kazuhiko Tsuruya,† Katsuo Sueishi,‡ Masazumi Tsuneyoshi,§ Mitsuo Iida,† and Yutaka Kiyohara* Departments of *Environmental Medicine, †Medicine and Clinical Science, ‡Pathophysiological and Experimental Pathology, and §Anatomic Pathology, Graduate School of Medical Sciences, Kyushu University, Fukuoka, Japan ABSTRACT Information regarding the association between prehypertension BP level and renal arteriosclerosis is limited. In 652 consecutive population-based autopsy samples without hypertension treatment before death, the relationship between the severity of renal arteriosclerosis and BP levels classified according to the criteria of the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure was examined. The age- and gender-adjusted frequencies of renal arteriosclerosis linearly increased with elevating BP levels; both hypertensive and prehypertensive subjects had significantly higher frequencies of renal arteriosclerosis than subjects with normal BP (normal 11.9%; prehypertension 28.5%; stage 1 hypertension 32.9%; stage 2 hypertension 58.2%; all P Ͻ 0.01 versus normal). In a logistic regression model, prehypertension was significantly associated with renal arteriosclerosis after adjustment for other cardiovascular risk factors (prehyper- tension multivariate-adjusted odds ratio [mOR] 5.99 [95% confidence interval (CI) 2.20 to 15.97]; stage 1 hypertension mOR 6.99 [95% CI 2.61 to 18.72]; stage 2 hypertension mOR 22.21 [95% CI 8.35 to 59.08]). This significant association was observed for all renal arterial sizes. -
Pathophysiology of Peripheral Arterial Disease and Risk Factors for Its Development
JOHN R. BARTHOLOMEW, MD* JEFFREY W. OLIN, DO* Section Head, Vascular Medicine Professor of Medicine and Director of Vascular Medicine Department of Cardiovascular Medicine Zena and Michael A. Wiener Cardiovascular Institute Cleveland Clinic Mt. Sinai School of Medicine Cleveland, OH New York, NY Pathophysiology of peripheral arterial disease and risk factors for its development ■ ABSTRACT ■ PATHOPHYSIOLOGY OF PAD Peripheral arterial disease (PAD) is a systemic Atherosclerosis is a complex process that involves atherosclerotic process for which the major risk endothelial dysfunction, lipid disturbances, platelet factors are similar to those for atherosclerosis in activation, thrombosis, oxidative stress, vascular the carotid, coronary, and other vascular beds. smooth muscle activation, altered matrix metabolism, Among the traditional risk factors for PAD, those remodeling, and genetic factors.2 More recently, the with the strongest associations are advanced age, role of inflammation in all stages of atherosclerosis 3 smoking, and diabetes mellitus. More recently, a development has been widely recognized. number of nontraditional risk factors for PAD have Atherosclerosis frequently develops at arterial bifur- cations and branches where endogenous atheroprotec- also been recognized. This article briefly reviews tive mechanisms are impaired as a result of the effects the pathophysiology of PAD and the evidence sup- of disturbed flow on endothelial cells.2 Risk factors such porting established and emerging risk factors for as increased age, diabetes mellitus, smoking, eleva- its development. tions in total and low-density lipoprotein (LDL) cho- lesterol, and hypertension play important roles in both eripheral arterial disease (PAD) refers to the initiation and the acceleration of this process.2 atherosclerotic and thromboembolic process- es that affect the aorta, its visceral arterial The stages of atherosclerosis branches, and arteries of the lower extremi- Pathologically, the stages of atherosclerosis are divided P1 ties. -

The Pathobiology of the Saccular Cerebral Artery Aneurysm Rupture
To those of us carrying saccular cerebral artery aneurysms, - and to my family Th e Neurosurgery Research Group, Biomedicum Helsinki Department of Neurosurgery, University of Helsinki Department of Neurosurgery, University of Kuopio Transplantation Laboratory, University of Helsinki The Pathobiology of Saccular Cerebral Artery Aneurysm Rupture and Repair -a Clinicopathological and Experimental Approach Juhana Frösen ACADEMIC DISSERTATION To be publicly discussed by the permission of the Medical Faculty of the University of Helsinki in the lecture hall of Töölö Hospital on the 15th of September 2006 at 12 o’clock noon. Helsinki 2006 Supervised by Professor Juha Jääskeläinen Department of Neurosurgery Kuopio University Hospital and Marjukka Myllärniemi, MD PhD University of Helsinki Reviewed by Docent Timo Kumpulainen Department of Neurosurgery Oulu University Central Hospital and Docent Anne Räisänen-Sokolowski Department of Pathology University of Helsinki Discussed with Associate Professor Robert M Friedlander Department of Neurosurgery Harvard Medical School ISBN 952-92-0787-5 (paperback) ISBN 952-10-3330-4 (PDF) Abbreviations 15-LOX 15-lipoxygenase enzyme AAA Abdominal aortic aneurysm ACA Anterior cerebral artery AcomA Anterior communicating artery AICA Anterior inferior cerebellar artery APKD Autosomal polycystic kidney disease ApoB Apolipoprotein B ApoE Apolipoprotein E BA Basilar artery bFGF-R Receptor for basic fi broblast growth factor EEL External elastic lamina ELISA Enzyme immunoabsorbent assay eNOS Endothelial nitric oxide -
Foam Cells”, a Hallmark of Atheromas
The Biology of Atherosclerotic Cardiovascular Disease FYI Venous & Arterial Systems Hey, how you doin’? Venous blood The 4 Chamber Heart from upper body Lung Mitral valve Rt. Lt. atrium atrium Pulm. Aorta Artery Tricuspid valve Right Left Aortic valve ventricle ventricle Venous blood Pulmonic from lower valve body Small Veins & Capillaries To heart, neck, arms Superior Vena Cava Pulm. v. Pulm. a. Rt. Atrium Aorta Lungs Rt. ventricle Lt. ventricle To abd., kidneys, Inferior pelvis, legs Vena Cava Small Veins & Capillaries FYI Anatomy of the Heart Blood Vessels Adventitia Media Intima Veins & Arteries have 3 layers. Intima: endothelial cells in contact with the blood. The internal elastic lamina forms the barrier between the intima and the underlying “tunica media.” The media has multiple layers of smooth muscle cells. The outer layer of connective tissue is the adventitia. Veins • Have thinner walls; less media. • Have a lower lumen pressure. • Have valves that direct blood back toward the heart Artery Vein Magnitude of the Problem • Despite changes in lifestyle and “statins” to lower cholesterol, & angioplasty, cardiovascular disease is FYI the #1 cause of death in the world. • Atherosclerosis kills 800,000/year in US. • Worldwide mortality is 12 million/year. Atherosclerosis Atherosclerosis is a disease process that produces blockages in arteries, mainly large and medium-sized arteries and can lead to ischemia (inadequate blood flow) of the heart, brain, or extremities. When severe, it can produce “infarction,” death of the tissue being supplied by the blocked artery. Adventitia Media Intima Lipoproteins Transport Fatty Substances Since high blood concentrations of cholesterol (especially in LDL), are a strong risk factor for atherosclerosis, many have believed that atherosclerosis is simply due to accumulation of lipids in the arterial wall. -

Atherosclerosisatherosclerosis
AtherosclerosisAtherosclerosis Atherosclerotic Cardiovascular Disease (ASCVD) Smooth m. proliferation Endothelial injury Lipids (cholesterol) Pathogenesis of atherosclerosis 1 Normal Artery Structure Lipoprotein particle 2 XX 60,00060,000 xx 180,000180,000 Robert Hamilton, Ph.D. EM: Negative staining Cardiovascular Research Inst., UCSF 3 The cholesterol in LDL accounts for ©Medscape approx. 70% of the plasma cholesterol Arteriosclerosis (Hardening of the arteries) Arterial wall thickening + loss of elasticity Monckeberg medial Arteriolosclerosis Atherosclerosis calcific sclerosis hyaline hyper- plastic ¾Age 50 -small arteries/arterioles -aorta & branches + ¾Radiologic calcif. -hyaline type / hyperplastic coronary arteries ¾Lumen intact -hypertension / diabetes -ASCVD causes 38% of ¾Clinically insignif. all deaths in N. America 4 ATHEROSCLEROSIS: response-to-injury model Atherosclerosis is a chronic inflammatory response of the arterial wall to endothelial injury. 1. Chronic endothelial injury 2. Accumulation of lipoproteins (LDL mainly) basic tenets 3. Monocyte adhesion to endothelium 4. Platelet adhesion 5. Factors releasedÆSMC recruitment 6. SMC proliferation and ECM production 7. Lipid accumulation: extracellular/mac-SMC Risk Factors for Atherosclerosis •Hyperlipidemia •Smoking •Hypertension •Turbulence •Genetics 5 Endothelial injury Early Chronic—repetitive injury non- denuding endothelial dysfunction -cig. smoke toxins -homocysteine -?? Infectious agents -cytokinesÆgenes for Endothelial injury Early Chronic—repetitive injury non- -

The Impact of Estrogen Receptor in Arterial and Lymphatic Vascular Diseases
International Journal of Molecular Sciences Review The Impact of Estrogen Receptor in Arterial and Lymphatic Vascular Diseases Coralie Fontaine 1, Florent Morfoisse 1, Florence Tatin 1, Audrey Zamora 1, Rana Zahreddine 1 , 2 1 1, 1, , Daniel Henrion , Jean-François Arnal , Françoise Lenfant y and Barbara Garmy-Susini * y 1 INSERM-UPS UMR U1048, Institut des Maladies Métaboliques et Cardiovasculaires, Université de Toulouse, BP 84225, 31 432 Toulouse cedex 04, France; [email protected] (C.F.); fl[email protected] (F.M.); fl[email protected] (F.T.); [email protected] (A.Z.); [email protected] (R.Z.); [email protected] (J.-F.A.); [email protected] (F.L.) 2 INSERM U1083 CNRS UMR 6015, CHU, MITOVASC Institute and CARFI Facility, Université d’Angers, 49933 ANGERS Cedex 09, France; [email protected] * Correspondence: [email protected] These authors contributed equally to this work. y Received: 1 April 2020; Accepted: 29 April 2020; Published: 4 May 2020 Abstract: The lower incidence of cardiovascular diseases in pre-menopausal women compared to men is well-known documented. This protection has been largely attributed to the protective effect of estrogens, which exert many beneficial effects against arterial diseases, including vasodilatation, acceleration of healing in response to arterial injury, arterial collateral growth and atheroprotection. More recently, with the visualization of the lymphatic vessels, the impact of estrogens on lymphedema and lymphatic diseases started to be elucidated. These estrogenic effects are mediated not only by the classic nuclear/genomic actions via the specific estrogen receptor (ER) α and β, but also by rapid extra-nuclear membrane-initiated steroid signaling (MISS). -

Erlanger Southeast Regional Stroke Center Ischemic & Hemorrhagic Stroke Education Booklet
Erlanger Southeast Regional Stroke Center Ischemic & Hemorrhagic Stroke Education Booklet Stroke_Booklet_AB179_2-20.indd 1 2/6/20 2:11 PM B.E. F.A.S.T. for Stroke Stroke is a sudden disorder of the blood supply to the brain, which can cause irreversible damage and disability. Time is critical when treating strokes. It is always important to identify when the symptoms started. Sometimes treatment may cause harm if given too late. Because treatment is time sensitive and there are many causes of stroke, always ask to be treated at a certified stroke treatment center. Sudden loss BALANCE of balance? Loss of vision in EYES one or both eyes? FACE Face look uneven? Arm or leg weak or ARM hanging down? Speech slurred? PEECH Trouble speaking S or seem confused? Time to IME T call 911. Stroke_Booklet_AB179_2-20.indd 2 2/6/20 2:11 PM B.E. F.A.S.T. for Stroke Table of Contents Introduction ...................................................................................................... 1 What is Stroke? ............................................................................................2-5 Stroke is a sudden disorder of the blood supply to the brain, which can cause irreversible Blood Supply to the Brain ..................................................................................2 damage and disability. Motor and Sensory Function.............................................................................3 Time is critical when treating strokes. It is always important to identify when the symptoms Left and Right Sides of the Brain -

(12) Patent Application Publication (10) Pub. No.: US 2004/0253327 A1 Niazi Et Al
US 2004O253327A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2004/0253327 A1 Niazi et al. (43) Pub. Date: Dec. 16, 2004 (54) COMPOSITIONS AND METHODS FOR Publication Classification REDUCING OR CONTROLLING BLOOD CHOLESTEROL, LIPOPROTEINS, (51) Int. Cl." ....................... A61K 35/78; A61K 31/695; TRIGLYCERIDES, AND SUGAR AND A61K 31/555 PREVENTING OR TREATING (52) U.S. Cl. ......................... 424/738; 424/757; 424/748; CARDOWASCULAR DISEASES 514/54; 514/63; 514/184 (76) Inventors: Sarfaraz K. Niazi, Deerfield, IL (US); (57) ABSTRACT Anjum Niazi, Deerfield, IL (US) This invention provides compositions and methods related Correspondence Address: to the administration of psyllium husk, f-sitosterol, guggul SARFARAZ, K. NAZI tree extract, guar gum and chromium as a combination to 20 RIVERSIDE DRIVE reduce or control blood cholesterol, triglycerides, low den DEERFIELD, IL 60015 (US) sity lipoproteins, blood Sugar or increasing or controlling high density lipoproteins in a mammal, to reduce arterial (21) Appl. No.: 10/250, 197 plaque build-up, atherosclerosis, in a mammal which may be asSociated with cardiovascular, cerebrovascular, peripheral (22) Filed: Jun. 12, 2003 vascular, or intestinal vascular disorders. US 2004/0253327 A1 Dec. 16, 2004 COMPOSITIONS AND METHODS FOR REDUCING emergency medical and/or Surgical procedures, and Signifi OR CONTROLLING BLOOD CHOLESTEROL, cant disability or death. Alternatively, the arterial wall can be LIPOPROTEINS, TRIGLYCERIDES, AND SUGAR severely weakened by the infiltration of the muscular layer AND PREVENTING OR TREATING with the lipid (cholesterol), inflammatory white blood cells, CARDIOVASCULAR DISEASES connective tissue and calcium, resulting in Soft and/or brittle areas which can become Segmentally dilated (aneurysmal) BACKGROUND OF INVENTION and rupture or crack leading to organ, limb or even life threatening hemorrhage. -

Peripheral Vascular Disease Becomes Increasingly Prevalent with by the Symptom Or Complication (E.G
SePTeMBer 2010 Informative and educational updates for providers FOCUS ON: PerIPherAl Always… • Document the cause of the peripheral arterial disease, VASCUlAr DISeASe if known, as well as the complication (e.g. PAD due to diabetes with ulcer lower leg). • Document arteriosclerosis as “arteriosclerosis of” and the site, “arteriosclerotic” or “arteriosclerosis with,” followed Peripheral vascular disease becomes increasingly prevalent with by the symptom or complication (e.g. arteriosclerosis of age. As such this is a growing concern in the United States given the the lower extremities with rest pain, arteriosclerosis of growing proportion of older adults. Based on a NhANeS report the the lower extremities with ulceration), not the symptom incidence can be as high as 15 to 17% in the population aged 70 and or complication alone. over. Documentation and Coding Tips4 The concern around peripheral vascular disease is several fold: Only a minority of patients may present with the classic symptoms of • “Peripheral arterial disease,” “peripheral vascular disease” limb claudication or ischemia. In one study only about 11 percent of and “intermittent claudication” are coded to 443.9 – the patients with PVD presented with classic symptoms.1 In another Peripheral vascular disease, unspecified. study as many as 28 percent of patients with peripheral vascular • Atherosclerosis of the native arteries of the extremities is disease were found to be physically inactive sometimes due to other coded based on documentation of the condition with the illness thereby precluding the development of symptoms.2 There is a symptom or complication: significant overlap of peripheral vascular disease with coronary artery 440.20 – Atherosclerosis of the extremities, unspecified disease, cerebrovascular disease and abdominal aortic aneurysms.