'The Mvule Tree Clinic'
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Vote:555 Wakiso District Quarter2
Local Government Quarterly Performance Report FY 2018/19 Vote:555 Wakiso District Quarter2 Terms and Conditions I hereby submit Quarter 2 performance progress report. This is in accordance with Paragraph 8 of the letter appointing me as an Accounting Officer for Vote:555 Wakiso District for FY 2018/19. I confirm that the information provided in this report represents the actual performance achieved by the Local Government for the period under review. Name and Signature: Accounting Officer, Wakiso District Date: 23/01/2019 cc. The LCV Chairperson (District) / The Mayor (Municipality) 1 Local Government Quarterly Performance Report FY 2018/19 Vote:555 Wakiso District Quarter2 Summary: Overview of Revenues and Expenditures Overall Revenue Performance Ushs Thousands Approved Budget Cumulative Receipts % of Budget Received Locally Raised Revenues 1,866,456 2,935,943 157% Discretionary Government Transfers 9,904,329 5,214,920 53% Conditional Government Transfers 49,420,127 26,067,150 53% Other Government Transfers 6,781,008 3,386,269 50% Donor Funding 1,582,182 485,303 31% Total Revenues shares 69,554,103 38,089,585 55% Overall Expenditure Performance by Workplan Ushs Thousands Approved Cumulative Cumulative % Budget % Budget % Releases Budget Releases Expenditure Released Spent Spent Planning 490,348 354,418 330,744 72% 67% 93% Internal Audit 140,357 71,796 59,573 51% 42% 83% Administration 8,578,046 6,260,718 5,539,808 73% 65% 88% Finance 1,133,250 730,592 652,040 64% 58% 89% Statutory Bodies 1,346,111 724,322 650,500 54% 48% 90% Production -
Uganda Community Development
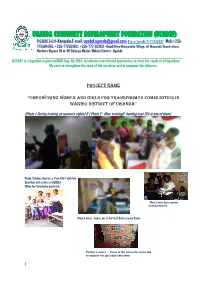
UGANDA COMMUNITY DEVELOPMENT FOUNDATION (UCODEF) P.O.BOX 24211–Kampala:E-mail: [email protected] Face book-UCODEF Mob:+256- 775684045, +256-772831951, +256-772-831921 -Head Office-Nakuwadde Village, off Masanafu Round-about, Northern Bypass Rd or Off Bulenga Market-Wakiso District –Uganda UCODEF is a Ugandan registered NGO Reg. No: 9154, to enhance coordinated approaches to meet the needs of all Ugandans. We exist to strengthen the voice of the voiceless and to empower the citizenry. PROJECT name “EMPOWERING WOMEN AND GIRLS FOR TRANSFORMED COMMUNITIES IN WAKISO DISTRICT OF UGANDA” (Photo 1: During training on women’s rights) & ( Photo 2 : After training& handing over IGA to one of them) Photo 3 below: Harriet, a ‘Pearl Girl’ with her Guardian and sisters at UCODEF Office for Scholastic materials Photo 5 above: Conny receives scholastic materials Photo 4 above : Sophia, one of the Pearl Girls receives Books Picture 6 above : Some of the scholastic materials to support the girl child education 1 1.0. PROJECT Empowering Women and Girls for Transformed Communities in Project Title Wakiso District of Uganda Geographic The project is implemented in Wakiso District of Uganda and in the 6 Sub- Coverage (List Counties; of Makindye –Sabagabo Sub-County, Nangabo S/C, Nsangi S/C, Sub-counties / Busukuma Sub-County, Wakiso Sub-County and Kakiri Town Council Areas) (Town Council). UCODEF : WOMEN AND GIRL EMPOWERMENT MODEL Girls attend formal and regular education with support of fees, Women seen working so hard bursaries and scholastic materials, employing multiple skills and human rights, while the out of school approaches to transform their lives attend vocational for livelihood and and those entrusted in their care, survival skills. -
Annual Crime Report 2019 Public
P ANDA OLIC UG E PR E OTE RV CT & SE P ANDA OLIC UG E PRO E TEC RV T & SE UGANDA POLICE Annual Crime Report 2019 Annual Crime Report - 2019 Page I 1 P ANDA OLIC UG E PR E OTE RV CT & SE POLICE DA AN G U E V R E C & S PROTE T Annual Crime Report 2019 Annual Crime Report - 2019 P ANDA OLIC UG E PR E OTE RV CT & SE Mandate The Uganda Police Force draws its mandate from the constitution of Uganda Chapter Twelve, Article 212 that stipulates the functions of the force as: (a) to protect life and property; (b) to preserve law and order; (c) to prevent and detect crime; and (d) to cooperate with the civilian authority and other security organs estab- lished under this Constitution and with the population generally. Vision “An Enlightened, Motivated, Community Oriented, Accountable and Modern Police Force; geared towards a Crime free society”. Mission “To secure life and property in a committed and Professional manner, in part- nership with the public, in order to promote development Annual Crime Report - 2019 P ANDA OLIC UG E PR E OTE RV CT & SE ADMINISTRATIVE AND PLANNING MACRO STRUCTURE FOR THE UGANDA POLICE FORCE ADMINISTRATIVE AND PLANNING MACRO STRUCTURE FOR THE UGANDA POLICE FORCE Inspector General of Police Police Authority Deputy Inspector General of Police Chief of Joint Staff Directorate of Police Fire Directorate of Human Rights Directorate of Operations Directorate of Traffic & Prevention and Rescue and Legal Services Road Safety Services Directorate of ICT Directorate of Counter Directorate of Police Health Directorate of INTERPOL -

Local Government Councils' Performance and Public Service
LOCAL GOVERNMENT COUNCILS’ PERFORMANCE AND PUBLIC SERVICE DELIVERY IN UGANDA Wakiso District Council Score-Card Report 2011/2012 Susan Namara - Wamanga Martin Kikambuse Ssali Peninah Kansiime ACODE Public Service Delivery and Accountability Report Series No.3, 2013 LOCAL GOVERNMENT COUNCILS’ PERFORMANCE AND PUBLIC SERVICE DELIVERY IN UGANDA Wakiso District Council Score-Card Report 2011/2012 Susan Namara - Wamanga Martin Kikambuse Ssali Peninah Kansiime ACODE Public Service Delivery and Accountability Report Series No.3, 2013 Published by ACODE P. O. Box 29836, Kampala Email: [email protected]; [email protected] Website: http://www.acode-u.org Citation: Namara-Wamanga, S., et.al., (2013). Local Government Councils’ Performance and Public Service Delivery in Uganda: Wakiso District Council Score-Card Report 2011/12. ACODE Public Service Delivery and Accountability Report Series No.3, 2013. Kampala. © ACODE 2013 All rights reserved. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form or by any means electronic, mechanical, photocopying, recording or otherwise without the prior written permission of the publisher. ACODE policy work is supported by generous donations and grants from bilateral donors and charitable foundations. The reproduction or use of this publication for academic or charitable purposes or for purposes of informing public policy is excluded from this restriction. ISBN 978-9970-07-022-0 Wakiso District Council Score-Card Report 2011/12 Wakiso District Council Score-Card -

Wakiso DLG.Pdf
Local Government Performance Contract FY 2016/17 Vote: 555 Wakiso District Structure of Performance Contract PART A: PERFORMANCE REQUIREMENTS OF ACCOUNTING OFFICERS PART B: SUMMARY OF DEPARTMENT PERFORMANCE AND WORKPLANS Pursuant to the Public Financial Management Act of 2015, Part VII – Accounting and Audit, Section 45 (3), the Accounting Officer shall enter into an annual budget performance contract with the Permanent Secretary/Secretary to the Treasury. The performance contract consists of two parts – Part A and Part B. Part A outlines the core performance requirements against which my performance as an Accounting Officer will be assessed, in two areas: 1. Budgeting, Financial Management and Accountability, which are common for all Votes; and 2. Achieving Results in five Priority Programmes and Projects identified for the specific Vote I understand that Central Government Accounting Officers will communicate their 5 priorities of the vote within three months of the start of the Financial Year and the priorities for local governments will be established centrally. Part B sets out the key results that a Vote plans to achieve in 2016/17. These take the form of summaries of Ministerial Policy Statement (MPS) for central government AOs and budget narrative summaries for Local government AOs. I hereby undertake, as the Accounting Officer, to achieve the performance requirements set out in Part A of this performance contract and to deliver on the outputs and activities specified in the work plan of the Vote for FY 2016/17 subject to the availability of budgeted resources set out in Part B. I, as the Accounting Officer, shall be responsible and personally accountable to Parliament for the activities of this Vote. -

LG Budget Estimates 201213 Wakiso.Pdf
Local Government Budget Estimates Vote: 555 Wakiso District Structure of Budget Estimates A: Overview of Revenues and Expenditures B: Detailed Estimates of Revenue C: Detailed Estimates of Expenditure D: Status of Arrears Page 1 Local Government Budget Estimates Vote: 555 Wakiso District A: Overview of Revenues and Expenditures Revenue Performance and Plans 2011/12 2012/13 Approved Budget Receipts by End Approved Budget June UShs 000's 1. Locally Raised Revenues 3,737,767 3,177,703 7,413,823 2a. Discretionary Government Transfers 5,373,311 4,952,624 5,648,166 2b. Conditional Government Transfers 28,713,079 27,512,936 32,601,298 2c. Other Government Transfers 6,853,215 4,532,570 10,697,450 3. Local Development Grant 1,757,586 1,949,046 1,756,183 Total Revenues 46,434,958 42,124,880 58,116,921 Expenditure Performance and Plans 2011/12 2012/13 Approved Budget Actual Approved Budget Expenditure by UShs 000's end of June 1a Administration 1,427,411 1,331,440 3,894,714 1b Multi-sectoral Transfers to LLGs 5,459,820 4,818,229 0 2 Finance 679,520 658,550 2,623,938 3 Statutory Bodies 1,017,337 885,126 1,981,617 4 Production and Marketing 3,060,260 3,015,477 3,522,157 5 Health 4,877,837 4,807,510 6,201,655 6 Education 21,144,765 19,753,179 24,948,712 7a Roads and Engineering 6,161,280 4,538,877 11,151,699 7b Water 802,836 631,193 1,063,321 8 Natural Resources 427,251 238,655 659,113 9 Community Based Services 610,472 678,202 1,175,071 10 Planning 630,334 302,574 560,032 11 Internal Audit 135,835 117,414 334,893 Grand Total 46,434,958 41,776,425 58,116,922 Wage Rec't: 22,456,951 21,702,872 24,924,778 Non Wage Rec't: 16,062,717 13,930,979 23,191,011 Domestic Dev't 7,915,291 6,142,574 10,001,133 Donor Dev't 0 0 0 Page 2 Local Government Budget Estimates Vote: 555 Wakiso District B: Detailed Estimates of Revenue 2011/12 2012/13 Approved Budget Receipts by End Approved Budget of June UShs 000's 1. -
Population by Parish
Total Population by Sex, Total Number of Households and proportion of Households headed by Females by Subcounty and Parish, Central Region, 2014 District Population Households % of Female Males Females Total Households Headed HHS Sub-County Parish Central Region 4,672,658 4,856,580 9,529,238 2,298,942 27.5 Kalangala 31,349 22,944 54,293 20,041 22.7 Bujumba Sub County 6,743 4,813 11,556 4,453 19.3 Bujumba 1,096 874 1,970 592 19.1 Bunyama 1,428 944 2,372 962 16.2 Bwendero 2,214 1,627 3,841 1,586 19.0 Mulabana 2,005 1,368 3,373 1,313 21.9 Kalangala Town Council 2,623 2,357 4,980 1,604 29.4 Kalangala A 680 590 1,270 385 35.8 Kalangala B 1,943 1,767 3,710 1,219 27.4 Mugoye Sub County 6,777 5,447 12,224 3,811 23.9 Bbeta 3,246 2,585 5,831 1,909 24.9 Kagulube 1,772 1,392 3,164 1,003 23.3 Kayunga 1,759 1,470 3,229 899 22.6 Bubeke Sub County 3,023 2,110 5,133 2,036 26.7 Bubeke 2,275 1,554 3,829 1,518 28.0 Jaana 748 556 1,304 518 23.0 Bufumira Sub County 6,019 4,273 10,292 3,967 22.8 Bufumira 2,177 1,404 3,581 1,373 21.4 Lulamba 3,842 2,869 6,711 2,594 23.5 Kyamuswa Sub County 2,733 1,998 4,731 1,820 20.3 Buwanga 1,226 865 2,091 770 19.5 Buzingo 1,507 1,133 2,640 1,050 20.9 Maziga Sub County 3,431 1,946 5,377 2,350 20.8 Buggala 2,190 1,228 3,418 1,484 21.4 Butulume 1,241 718 1,959 866 19.9 Kampala District 712,762 794,318 1,507,080 414,406 30.3 Central Division 37,435 37,733 75,168 23,142 32.7 Bukesa 4,326 4,711 9,037 2,809 37.0 Civic Centre 224 151 375 161 14.9 Industrial Area 383 262 645 259 13.9 Kagugube 2,983 3,246 6,229 2,608 42.7 Kamwokya -

The Uganda Gazette, General Notice No. 425 of 2021
LOCAL GOVERNMENT COUNCIL ELECTIONS, 2021 SCHEDULE OF ELECTION RESULTS FOR DISTRICT/CITY DIRECTLY ELECTED COUNCILLORS DISTRICT CONSTITUENCY ELECTORAL AREA SURNAME OTHER NAME PARTY VOTES STATUS ABIM LABWOR COUNTY ABIM KIYINGI OBIA BENARD INDEPENDENT 693 ABIM LABWOR COUNTY ABIM OMWONY ISAAC INNOCENT NRM 662 ABIM LABWOR COUNTY ABIM TOWN COUNCIL OKELLO GODFREY NRM 1,093 ABIM LABWOR COUNTY ABIM TOWN COUNCIL OWINY GORDON OBIN FDC 328 ABIM LABWOR COUNTY ABUK TOWN COUNCIL OGWANG JOHN MIKE INDEPENDENT 31 ABIM LABWOR COUNTY ABUK TOWN COUNCIL OKAWA KAKAS MOSES INDEPENDENT 14 ABIM LABWOR COUNTY ABUK TOWN COUNCIL OTOKE EMMANUEL GEORGE NRM 338 ABIM LABWOR COUNTY ALEREK OKECH GODFREY NRM Unopposed ABIM LABWOR COUNTY ALEREK TOWN COUNCIL OWINY PAUL ARTHUR NRM Unopposed ABIM LABWOR COUNTY ATUNGA ABALLA BENARD NRM 564 ABIM LABWOR COUNTY ATUNGA OKECH RICHARD INDEPENDENT 994 ABIM LABWOR COUNTY AWACH ODYEK SIMON PETER INDEPENDENT 458 ABIM LABWOR COUNTY AWACH OKELLO JOHN BOSCO NRM 1,237 ABIM LABWOR COUNTY CAMKOK ALOYO BEATRICE GLADIES NRM 163 ABIM LABWOR COUNTY CAMKOK OBANGAKENE POPE PAUL INDEPENDENT 15 ABIM LABWOR COUNTY KIRU TOWN COUNCIL ABURA CHARLES PHILIPS NRM 823 ABIM LABWOR COUNTY KIRU TOWN COUNCIL OCHIENG JOSEPH ANYING UPC 404 ABIM LABWOR COUNTY LOTUKEI OBUA TOM INDEPENDENT 146 ABIM LABWOR COUNTY LOTUKEI OGWANG GODWIN NRM 182 ABIM LABWOR COUNTY LOTUKEI OKELLO BISMARCK INNOCENT INDEPENDENT 356 ABIM LABWOR COUNTY MAGAMAGA OTHII CHARLES GORDON NRM Unopposed ABIM LABWOR COUNTY MORULEM OKELLO GEORGE ROBERT NRM 755 ABIM LABWOR COUNTY MORULEM OKELLO MUKASA -

Office of the Auditor General the Republic of Uganda Report of the Auditor General on the Financial Statements of Wakiso Distric
OFFICE OF THE AUDITOR GENERAL THE REPUBLIC OF UGANDA REPORT OF THE AUDITOR GENERAL ON THE FINANCIAL STATEMENTS OF WAKISO DISTRICT LOCAL GOVERNMENT FOR THE YEAR ENDED 30TH JUNE, 2015 REPORT AND OPINION OF THE AUDITOR GENERAL ON THE FINANCIAL STATEMENTS OF WAKISO DISTRICT LOCAL GOVERNMENT FOR THE YEAR ENDED 30th JUNE 2015 THE HON. SPEAKER OF PARLIAMENT Introduction I have audited the accompanying financial statements of Wakiso District for the year ended 30thJune, 2015. These Financial statements comprise the Statement of Financial Position as at 30thJune, 2015, Statement of Financial Performance, Statement of Changes in Equity, Cash flow Statement together with other accompanying statements, notes and accounting policies. Management’s responsibility for the Financial Statements Under Article 164 of the Constitution of the Republic Of Uganda, 1995, and Section 45 of the Public Finance Management Act, 2015, the Accounting Officer is accountable to Parliament for the funds and resources of Wakiso district. The Accounting Officer is also responsible for the preparation of financial statements in accordance with the requirements of the Local Governments Financial and Accounting Manual, 2007, and for such internal control as management determines necessary to enable the preparation of financial statements that are free from material misstatement whether due to fraud or error. Auditor’s Responsibility My responsibility as required by Article 163 of the Constitution of the Republic of Uganda, Section 87 of the Local Governments Act and Sections 13, 16 and 19 of the National Audit Act,2008 is to express an opinion on these financial statements based on my audit. I conducted the audit in accordance with International Standards on Auditing (ISA)/International Standards of Supreme Audit Institutions (ISSAIs). -

The “Uganda Gazettepublished
The ns tm biic or vgam» \ Published by “Uganda Gazette Authority Vol. XCIII No. 17 10th March, 2000 Price: Shs. 700 CONTENTS 11. CWH Importer Unknown/Capt 2 Dozs Men’s Shirts (New) 19 Dozs Boy’s Trousers The Customs Management Act— Notice................ 87-88 (New) 3 Pcs Gambling The Companies Act—Notice...................................... 88 Machines Display Screens 7 Dozs + 11 Pcs Perfumes The Advocates Act—Notices.............. 88 12. CWH Importer Unknown/Capt 1 Pkg Cloth, Toys, The Privatisation Unit—Notice.................................. 89 Windsrecn-Protectors Pottie Paraa Lodges Limited—Notice .......................... 89 13. CWH Assorted Importers (Capt) 8 Pkgs Assorted The Money Lenders Act—Notice .......................... 89 Personal Effects 14 CWH C. Drezen (Copt) 1 Pkg Assorted Spares The Trade Marks Act—Registration of applications 90-92 (Air Toulouse) and 20 Tins Turbo Oil Advertisements ................................................ 92-94 2350 940 ML 15. CWH Assorted Importers (Capt) 11 Pkgs Assorted Personal Effects 17 Pcs Toner Cartridges General Notice No. 95 of 2000. 1 Pc Used TV 1 Pkg Shower Fittings THE CUSTOMS MANAGEMENT ACT. 16. CWH Mukasa (EN) 1 Pc Fridge (Cap. 27). 1 Pc Washing Machine NOTICE OF SALE BY PUBLIC AUCTION. 2 Pcs Cleaner and Walker 1 Pc Fan Notice is hereby given for general information that 17. CWH Importer Unknown (EN) 47 Ctns Tassenburg Wine Uganda Revenue Authority will conduct a sale by public 18. CWH Nakascro Blood 2 Pkgs Tube Sealer auction for goods whose particulars appear in the Schedule Bank (EN) MDL ACS-152 hereto at lhe Customs Warehouse. 19. CWH Importer Unknown (EN) 4 Pkgs Assorted Garments 37 Rolls Textile Material Time: After one calendar month. -

Uganda National Roads Network
UGANDA NATIONAL ROADS NETWORK REPUBLIC OF SOUTH SUDAN Musingo #" !P Kidepo a w K ± r i P !P e t Apoka gu a K m #" lo - g - L a o u k - #" g u P i #" n d Moyo!P g o i #"#" - t #"#" N i k #" KOBOKO M e g a #" #" #" l Nimule o #"!P a YUMBE #" u!P m ng m o #" e #" Laropi i #" ro ar KAABONG #" !P N m K #" (! - o - te o e om Kaabong#"!P g MOYO T c n o #" o #" L be Padibe !P - b K m !P LAMWO #" a oboko - Yu Yumbe #" om r K #" #" #" O #" Koboko #" #" - !P !P o Naam REGIONS AND STATIONS Moy n #" Lodonga Adjumani#" Atiak - #" Okora a #" Obongi #" !P #" #" a Loyoro #" p #" Ob #" KITGUM !P !P #" #" ong !P #" #" m A i o #" - #" - K #" Or u - o lik #" m L Omugo ul #" !P u d #" in itg o i g Kitgum t Maracha !P !P#" a K k #" !P #" #"#" a o !P p #" #" #" Atiak K #" e #" (!(! #" Kitgum Matidi l MARACHA P e - a #" A #"#" e #" #" ke d #" le G d #" #" i A l u a - Kitgum - P l n #" #" !P u ADJUMANI #" g n a Moyo e !P ei Terego b - r #" ot Kotido vu #" b A e Acholibur - K o Arua e g tr t u #" i r W #" o - O a a #" o n L m fe di - k Atanga KOTIDO eli #" ilia #" Rh #" l p N o r t h #"#" B ino Rhino !P o Ka Gulu !P ca #" #"#" aim ARUA mp - P #" #" !P Kotido Arua #" Camp Pajule go #" !P GULU on #" !P al im #" !PNariwo #" u #" - K b A ul r A r G de - i Lira a - Pa o a Bondo #" Amuru Jun w id m Moroto Aru #" ctio AMURU s ot !P #" n - A o #" !P A K i !P #" #" PADER N o r t h E a s t #" Inde w Kilak #" - #" e #" e AGAGO K #"#" !P a #" #" #" y #" a N o #" #" !P #" l w a Soroti e #"#" N Abim b - Gulu #" - K d ilak o b u !P #" Masindi !P i um !P Adilang n - n a O e #" -

Vote:555 Wakiso District Quarter4
Local Government Quarterly Performance Report FY 2019/20 Vote:555 Wakiso District Quarter4 Terms and Conditions I hereby submit Quarter 4 performance progress report. This is in accordance with Paragraph 8 of the letter appointing me as an Accounting Officer for Vote:555 Wakiso District for FY 2019/20. I confirm that the information provided in this report represents the actual performance achieved by the Local Government for the period under review. Kuruhiira Godfrey MA Date: 21/08/2020 cc. The LCV Chairperson (District) / The Mayor (Municipality) 1 Local Government Quarterly Performance Report FY 2019/20 Vote:555 Wakiso District Quarter4 Summary: Overview of Revenues and Expenditures Overall Revenue Performance Ushs Thousands Approved Budget Cumulative Receipts % of Budget Received Locally Raised Revenues 13,602,663 9,569,528 70% Discretionary Government 9,854,702 9,817,429 100% Transfers Conditional Government Transfers 48,179,822 50,024,180 104% Other Government Transfers 8,611,925 6,424,194 75% External Financing 1,396,943 1,753,891 126% Total Revenues shares 81,646,055 77,589,222 95% Overall Expenditure Performance by Workplan Ushs Thousands Approved Cumulative Cumulative % Budget % Budget % Releases Budget Releases Expenditure Released Spent Spent Administration 13,387,970 18,993,488 18,521,164 142% 138% 98% Finance 4,360,851 943,148 839,842 22% 19% 89% Statutory Bodies 2,713,350 1,429,852 1,417,423 53% 52% 99% Production and Marketing 2,170,674 1,701,953 1,649,885 78% 76% 97% Health 12,469,202 10,688,625 9,935,968 86% 80% 93% Education