Spatial, Temporal, and Spatiotemporal Analysis of Malaria in Hubei
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Landscape Analysis of Geographical Names in Hubei Province, China
Entropy 2014, 16, 6313-6337; doi:10.3390/e16126313 OPEN ACCESS entropy ISSN 1099-4300 www.mdpi.com/journal/entropy Article Landscape Analysis of Geographical Names in Hubei Province, China Xixi Chen 1, Tao Hu 1, Fu Ren 1,2,*, Deng Chen 1, Lan Li 1 and Nan Gao 1 1 School of Resource and Environment Science, Wuhan University, Luoyu Road 129, Wuhan 430079, China; E-Mails: [email protected] (X.C.); [email protected] (T.H.); [email protected] (D.C.); [email protected] (L.L.); [email protected] (N.G.) 2 Key Laboratory of Geographical Information System, Ministry of Education, Wuhan University, Luoyu Road 129, Wuhan 430079, China * Author to whom correspondence should be addressed; E-Mail: [email protected]; Tel: +86-27-87664557; Fax: +86-27-68778893. External Editor: Hwa-Lung Yu Received: 20 July 2014; in revised form: 31 October 2014 / Accepted: 26 November 2014 / Published: 1 December 2014 Abstract: Hubei Province is the hub of communications in central China, which directly determines its strategic position in the country’s development. Additionally, Hubei Province is well-known for its diverse landforms, including mountains, hills, mounds and plains. This area is called “The Province of Thousand Lakes” due to the abundance of water resources. Geographical names are exclusive names given to physical or anthropogenic geographic entities at specific spatial locations and are important signs by which humans understand natural and human activities. In this study, geographic information systems (GIS) technology is adopted to establish a geodatabase of geographical names with particular characteristics in Hubei Province and extract certain geomorphologic and environmental factors. -
Adaptive Optimal Allocation of Water Resources Response to Future Water
www.nature.com/scientificreports OPEN Adaptive optimal allocation of water resources response to future water availability and water demand in the Han River basin, China Jing Tian1, Shenglian Guo1*, Lele Deng1, Jiabo Yin1, Zhengke Pan2, Shaokun He1 & Qianxun Li1 Global warming and anthropogenic changes can result in the heterogeneity of water availability in the spatiotemporal scale, which will further afect the allocation of water resources. A lot of researches have been devoted to examining the responses of water availability to global warming while neglected future anthropogenic changes. What’s more, only a few studies have investigated the response of optimal allocation of water resources to the projected climate and anthropogenic changes. In this study, a cascade model chain is developed to evaluate the impacts of projected climate change and human activities on optimal allocation of water resources. Firstly, a large set of global climate models (GCMs) associated with the Daily Bias Correction (DBC) method are employed to project future climate scenarios, while the Cellular Automaton–Markov (CA–Markov) model is used to project future Land Use/Cover Change (LUCC) scenarios. Then the runof simulation is based on the Soil and Water Assessment Tool (SWAT) hydrological model with necessary inputs under the future conditions. Finally, the optimal water resources allocation model is established based on the evaluation of water supply and water demand. The Han River basin in China was selected as a case study. The results show that: (1) the annual runof indicates an increasing trend in the future in contrast with the base period, while the ascending rate of the basin under RCP 4.5 is 4.47%; (2) a nonlinear relationship has been identifed between the optimal allocation of water resources and water availability, while a linear association exists between the former and water demand; (3) increased water supply are needed in the water donor area, the middle and lower reaches should be supplemented with 4.495 billion m3 water in 2030. -
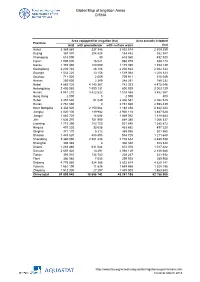
Global Map of Irrigation Areas CHINA
Global Map of Irrigation Areas CHINA Area equipped for irrigation (ha) Area actually irrigated Province total with groundwater with surface water (ha) Anhui 3 369 860 337 346 3 032 514 2 309 259 Beijing 367 870 204 428 163 442 352 387 Chongqing 618 090 30 618 060 432 520 Fujian 1 005 000 16 021 988 979 938 174 Gansu 1 355 480 180 090 1 175 390 1 153 139 Guangdong 2 230 740 28 106 2 202 634 2 042 344 Guangxi 1 532 220 13 156 1 519 064 1 208 323 Guizhou 711 920 2 009 709 911 515 049 Hainan 250 600 2 349 248 251 189 232 Hebei 4 885 720 4 143 367 742 353 4 475 046 Heilongjiang 2 400 060 1 599 131 800 929 2 003 129 Henan 4 941 210 3 422 622 1 518 588 3 862 567 Hong Kong 2 000 0 2 000 800 Hubei 2 457 630 51 049 2 406 581 2 082 525 Hunan 2 761 660 0 2 761 660 2 598 439 Inner Mongolia 3 332 520 2 150 064 1 182 456 2 842 223 Jiangsu 4 020 100 119 982 3 900 118 3 487 628 Jiangxi 1 883 720 14 688 1 869 032 1 818 684 Jilin 1 636 370 751 990 884 380 1 066 337 Liaoning 1 715 390 783 750 931 640 1 385 872 Ningxia 497 220 33 538 463 682 497 220 Qinghai 371 170 5 212 365 958 301 560 Shaanxi 1 443 620 488 895 954 725 1 211 648 Shandong 5 360 090 2 581 448 2 778 642 4 485 538 Shanghai 308 340 0 308 340 308 340 Shanxi 1 283 460 611 084 672 376 1 017 422 Sichuan 2 607 420 13 291 2 594 129 2 140 680 Tianjin 393 010 134 743 258 267 321 932 Tibet 306 980 7 055 299 925 289 908 Xinjiang 4 776 980 924 366 3 852 614 4 629 141 Yunnan 1 561 190 11 635 1 549 555 1 328 186 Zhejiang 1 512 300 27 297 1 485 003 1 463 653 China total 61 899 940 18 658 742 43 241 198 52 -

COVID-19 Situation Report #7
COVID-19 Situation Report #7 February 27, 2020 Key Updates • The number of new COVID-19 cases outside of China has exceeded number of new cases reported in China for the first time. • More than 14 new countries have reported cases since February 22. • United Airlines and Project HOPE are partnering to procure and deliver 15 ventilators to 11 hospitals in Hubei Province in coming days. • Project HOPE is procuring and preparing for the distribution of critically needed medical equipment including medical air compressors, defibrillators and Staff member of the quarantine unit at patient monitors for hospitals in Wuhan. Shanghai Children's Medical Center • In response to the increase in global cases, HOPE is expanding its response strategy to include pandemic preparedness activities. Response Tracker Situation Overview Facilitated the distribution of PPE and supplies including more than: • 4.2 million face masks Rise in Number of Cases Outside of China • 87,000 isolation gowns On February 25, the number of new cases of COVID-19 reported • 20,300 protective coveralls outside of China exceeded the number of new cases in China for • 273,000 pairs of exam gloves the first time.i The total number of cases globally is now 82,604 and 2,810 deaths. Of these, 4,106 cases and 66 deaths have Supplies delivered to more than 22 hospitals across Hubei been reported outside of mainland China across 49 countries Province (17+), Shanghai, Yunan and territories as well as the Diamond Cruise Ship.ii Province, Jiangsu Province, Anhui Province, Sichuan Province Since February 22, more than 14 new countries have reported cases of COVID-19 including: Lebanon, Israel, Kuwait, Algeria, Upcoming distributions iii • 15 ventilators and 12 medical Austria, Croatia, Switzerland, Brazil , Afghanistan, Denmark, air compressors iv Estonia, Norway, Romania and Iraq. -

Research on Urban Network of Wuhan Metropolitan Area in China Based on Social Network Analysis
International Journal of Culture and History, Vol. 3, No. 1, March 2017 Research on Urban Network of Wuhan Metropolitan Area in China Based on Social Network Analysis Jing-Xin Nie, Ya-Ping Huang, and Pei Chen according to enterprise organizations [22], [23]. Abstract—This article is based on the retrospect of theoretical The essence of urban network is intercity relation, and way and analysis method of town correlation measure, relational data is always applied in urban network research. summarized the advantages and disadvantages. Then the article With the rapid development of information and proposed the social network analysis method with network data of express, in order to analyze the town correlation measure. communication technology, distance of space and time Taking Wuhan metropolitan area in china as practical between cities is greatly compressed, and the connections experiment objects, and found out the network characteristics of between cities are more and more closely. Excavating it, which dominance and polarization coexisted, axes and relational data has become a new trend in research of urban corridors gathered in space. In the view of social network, the network. Social Network Analysis, SNA for short, is a urban system of Wuhan metropolitan area has not been methodology which describes the whole form, characteristics completed, though the inner core group has formed, but the connection between the low-level nodes is not strong enough. and structure of network. SNA has obvious advantage in relation expression; a network can be regarded either as a Index Terms—Express network, social network analysis, whole or a part, so that reveals the integration and hierarchy of Wuhan metropolitan area, urban network. -

Analysis of the Maternal and Child Health Care Status in Suizhou City, Hubei Province, China, from 2005 to 2011
Analysis of the Maternal and Child Health Care Status in Suizhou City, Hubei Province, China, from 2005 to 2011 Cui-Ling Li1, Tao Jiang2, Xiu-Zhen Hu2, Kai Zhao1, Qiong Yu1, Hui-Ping Zhang1* 1 Family Planning Research Institute, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, China, 2 Suizhou Maternal and Child Health-care Hospital, Suizhou, Hubei, China Abstract Background: Improving the health and well-being of women and children has long been a common goal throughout the world. From 2005 to 2011, Suizhou City had an annual average of 22,405 pregnant and parturient women (1.04% of the population) and 98,811 children under 5 years old (4.57% of the population). Understanding the status of maternal and child health care in Suizhou City during such period can provide the local health administrative department valid scientific bases upon which to construct effective policies. Methods: Various types of annual reports on maternal and child health care were collected and analyzed retrospectively. Results: Mortality rates for infants and children under 5 years showed a declining trend, while the rates of newborn home visiting, maternal health service coverage, and children health systematic management increased annually in Suizhou City from 2005 to 2011. The incidence of birth defect increased from 2.42‰ in 2005 to 3.89‰ in 2011. The maternal mortality ratio (MMR) fluctuated from 8.39/100,000 to 28.77/100,000, which was much lower than the national MMR (30.0/100,000 in 2010). The rates of hospitalized delivery and births attended by trained health personnel for pregnant women increased to more than 90% in the past five years. -

Environmental Impact Assessment Public Disclosure Authorized Public Disclosure Authorized
Wol ank Financed Project E584 Volume 3 Public Disclosure Authorized Xiaogan-Xiangfan Expressway Project Environmental Impact Assessment Public Disclosure Authorized Public Disclosure Authorized Hubei Provincial I Comm unications Departmeut Public Disclosure Authorized Marc. .2002 W uhan Cihina FILE COPY Envi-onmentalnImpact Assessment of Aiaogan-,Xiangfan Erpressway Table of Contents Chapter] Introduction ...................................... 1.1 Project Background ..................................... 1 1.2 Environmental Assessment ..................................... I 1.3 Purpose of EA .................................... 2 1.4 Bases of Assessment ..................................... 3 1.5 EA Management and Procedure ..................................... 5 1.6 Scope of Assessment ..................................... 7 1.7 Methodology ..................................... 7 Chapter 2 Environmental Assessment Team .................................... 11 2.1 Brief Introduction of SSSRI .................................... 1 2.2 Team Members .................................... 1I Chapter 3 Project Description .................................... 12 3.1 Directly Impacted Areas .................................... 12 3.2 Location .................................... 12 3.3 Alignment Corridor and Main Control Points .................................... 12 3.4 Traffic Volume Prediction ................................... 13 3.5 Key Technical Standards and Construction Scale ..................................... 13 3.6 Accessory Facilities -

Natural City Growth in the People's
Natural City Growth in the People’s Republic of China Peter H. Egger,Gabriel Loumeau, and Nicole Püschel∗ This paper analyzes the growth of Metropolitan Statistical Areas in the PRC between 1992 and 2013 by focusing on the night-light radiance—a measure of economic activity—of connected subcity places that we refer to as a natural city. This paper documents the rapid growth of natural cities in the PRC between 1992 and 2009 that was followed by a slight reduction in the size of some natural cities between 2010 and 2013 in the aftermath of the recent global financial crisis. Institutional factors—such as the location of places near Special Economic Zones, the ramifications of legal migration from rural to urban areas following reforms to the hukou (household registration) system, and infrastructure accessibility—are found to be important drivers of the integration of peripheral places into natural cities. Keywords: city growth, Metropolitan Statistical Areas, People’s Republic of China JEL codes: O20, R12, R40 I. Introduction With the increase in global population, the change in urbanization rates around the world is a dynamic phenomenon. While in 1994 only about 30% of the world’s population lived in cities, as defined by national statistical offices, about 54% did in 2014.1 In the People’s Republic of China (PRC), which has been among the most dynamic economies in the world over the last quarter of a century, almost 25% of the population has moved to urban areas during the past 2 decades. The PRC’s National New-Type Urbanization Plan, 2014–2020 targets an urbanization rate of 60% by 2020. -

World Bank Document
RECEIVEDR. 960CTi7 PM41i 4 v6>i.9 Public Disclosure Authorized Connection Road of National Road Project III in Hubei Province Statement of EnvironmentalImpact Assessment Public Disclosure Authorized Public Disclosure Authorized Research Institute of Highways, Ministry of Communications September 1996 Public Disclosure Authorized I I Contents CHAPTER 1 INTRODUCTION I CHAPTER 2 GENERAL PRINCIPLES OF ASSESSMENT 2 2.1 Assessment purpose 2 2.2 Basic Materials and Documents for the EIA Report 2 2.3 Assessment Scope and Standards 2 2.4 AssessmentMethod 2 2.5 AssessmentTime Period 3 CHAPTER3 ENGINEERINGBRIEF 4 3.1 Traffic Forecast 4 3.2 Construction Scale 4 3.3 Alignmentand Major Control Point 4 3.4 Major Engineering Work 6 3.5 Main EnvironmentalImpact Analysis 6 CHAPTER 4 CURRENT ENVIRONMENT CONDITION AND 8 ASSESSMENT 4.1 Current Status and Assessment of Acoustic Environment 8 4.2 Current Status and Assessment of Air Environment 9 4.3 Current Status and Assessment of Water Envirorunent 9 CHAPTER 5 ENVIRONMENTAL IMPACT FORECAST AND 11 ASSESSMENT 5.1 EcologicalEnvironmental impact assessment I1 5.2 Social EnvironmnentImpact Forecast and Assessment 12 5.3 Acoustic EnvironmentImpact Forecast and Assessment 13 5.4 Air Environment Impact Forecast and Assessment 16 CHAPTER 6 ENVIRONMENT PROTECTION MEASURES AND 26 RECOMMENDATIONS 6.1 EnvironmentalProtection Measures in Design Period 26 6.2 EnvironmentalProtection Measures in ConstructionPeriod 26 6.3 EnvironmentalProtection Measures in Operation Period 28 CHAPTER 7 ENVIRONMENTAL MONITOR AND MANAGEMENT 29 7.1 EnvironmentalMonitor 29 7.2 EnvironmentalManagement 30 7.3 EnvironmentalAction Plan and Cost Estimation 31 CHAPTER 8 CONCLUSIONS 33 I CHAPTER 1 INTRODUCTION Beijing-Zhuhai national trunk road is part of the "Two Longitudinal and Two Lateral" national trunk roads, which shall be built by the year of 2000 planned by the State Council. -
Natural City Growth in the People's Republic of China
Natural City Growth in the People’s Republic of China Peter H. Egger,Gabriel Loumeau, and Nicole Püschel∗ This paper analyzes the growth of Metropolitan Statistical Areas in the PRC between 1992 and 2013 by focusing on the night-light radiance—a measure of economic activity—of connected subcity places that we refer to as a natural city. This paper documents the rapid growth of natural cities in the PRC between 1992 and 2009 that was followed by a slight reduction in the size of some natural cities between 2010 and 2013 in the aftermath of the recent global financial crisis. Institutional factors—such as the location of places near Special Economic Zones, the ramifications of legal migration from rural to urban areas following reforms to the hukou (household registration) system, and infrastructure accessibility—are found to be important drivers of the integration of peripheral places into natural cities. Keywords: city growth, Metropolitan Statistical Areas, People’s Republic of China JEL codes: O20, R12, R40 I. Introduction With the increase in global population, the change in urbanization rates around the world is a dynamic phenomenon. While in 1994 only about 30% of the world’s population lived in cities, as defined by national statistical offices, about 54% did in 2014.1 In the People’s Republic of China (PRC), which has been among the most dynamic economies in the world over the last quarter of a century, almost 25% of the population has moved to urban areas during the past 2 decades. The PRC’s National New-Type Urbanization Plan, 2014–2020 targets an urbanization rate of 60% by 2020. -
Chinese Mainland
Address List of Special Warehousing Service Note: The address marked in red are newly added address. (Effective date:October 1, 2021) Province / Directly- controlled City District/county Town, Sub-district and House Number Municipality / Autonomous Region/SAR B4-25, Gate 1, ProLogis Logistics Park, No.1 Tiedi Road, Anhui Province Hefei Shushan District High-tech Zone No.18 Tianzhushan Road, Longshan Sub-district, Wuhu Anhui Province Wuhu Jiujiang District Economic and Technological Development Zone Anhui Province Chuzhou Langya District Longji Leye Photovoltaic Co., Ltd., No.19 Huai'an Road 3/F, No.8 Building, South Area, Lixiang Innovation Park, Anhui Province Chuzhou Nanqiao District Chuzhou, 018 Township Road Anhui Province Chuzhou Nanqiao District No.19 Huai'an Road Yuanrong New Material Holding Co., Ltd., 50 Meters Anhui Province Hefei Shushan District Westward of Bridge of Intersection of Changning Avenue and Ningxi Road Anhui Province Hefei Yaohai District No.88 Dayu Road Anhui Province Hefei Yaohai District No.2177 Dongfang Avenue Beijing BOE Vision-Electronic Technology Co., Ltd., No. Anhui Province Hefei Yaohai District 2177 Dongfang Avenue Anhui Province Hefei Yaohai District No.668 Longzihu Road Anhui Province Hefei Yaohai District No. 668 Longzihu Road Anhui Province Hefei Yaohai District No.2177 Tongling North Road Anhui Province Hefei Yaohai District No.3166 Tongling North Road Anhui Province Hefei Yaohai District No.8 Xiangwang Road Anhui Province Wuhu Jiujiang District No. 8 Anshan Road Anhui Province Wuhu Jiujiang District -

A Survey of the Birds of the Dabie Shan Range, Central China
FORKTAIL 24 (2008): 80–91 A survey of the birds of the Dabie Shan range, central China YANG LIU, ZHENG-WANG ZHANG, JIAN-QIANG LI, YU ZHANG, SHAN LU and XIANG-FENG RUAN The Dabie Shan (Dabie Mountains) range, straddling Henan, Hubei and Anhui provinces in central China, harbours a rich bird diversity, representing a transition between Palaearctic and Oriental realms. Although historical information is available on the avifauna of this region, no recent comprehensive bird survey has been carried out. In this paper we present a bird inventory study for the Dabie Shan range based on ornithological surveys conducted between 2004 and 2006. We recorded 238 bird species during these surveys. Species of conservation significance include Falcated Duck Anas falcata, Reeves’s Pheasant Syrmaticus reevesii, Baer’s Pochard Aythya baeri, Fairy Pitta Pitta nympha, and Brown-chested Jungle Flycatcher Rhinomyias brunneata. Ten species are new records for the Dabie Shan range. This region is notable as a transition zone, in that most winter visitors and migrants are Palaearctic and a large proportion of summer breeders are Oriental species. It is also the northernmost part of the range of a number of subtropical breeders in China. The avifauna is threatened by extensive habitat loss outside the protected areas of the range, and we discuss conservation recommendations for the whole region. INTRODUCTION information on species of conservation concern to inform reserve managers at the regional level, and to improve our The Dabie Shan (Dabie Mountains) range (30°02′– knowledge about the distribution of these species. The 32°20′N 114°30′–117°05′E) lies in a transition zone third purpose of our investigation was to document the between the Palaearctic and Oriental regions in China, avifauna of a few places which had received little or no and so is crucial to our understanding of biogeography of prior ornithological attention.