Cell Replacement Therapy for Retinal and Optic Nerve Diseases: Cell Sources, Clinical Trials and Challenges
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Ageing Research Reviews 61 (2020) 101069
Ageing Research Reviews 61 (2020) 101069 Contents lists available at ScienceDirect Ageing Research Reviews journal homepage: www.elsevier.com/locate/arr Review Discovery of new epigenomics-based biomarkers and the early diagnosis of neurodegenerative diseases T Davin Leea,1, Yoon Ha Choib,1, Jinsoo Seoa, Jong Kyoung Kimb,*, Sung Bae Leea,* a Department of Brain & Cognitive Sciences, DGIST, Daegu, Republic of Korea b Department of New Biology, DGIST, Daegu, Republic of Korea ARTICLE INFO ABSTRACT Keywords: Treatment options for many neurodegenerative diseases are limited due to the lack of early diagnostic proce- Neurodegenerative diseases dures that allow timely delivery of therapeutic agents to affected neurons prior to cell death. While notable iPSC advances have been made in neurodegenerative disease biomarkers, whether or not the biomarkers discovered Organoid to date are useful for early diagnosis remains an open question. Additionally, the reliability of these biomarkers Single-cell sequencing has been disappointing, due in part to the large dissimilarities between the tissues traditionally used to source Epigenetic alteration biomarkers and primarily diseased neurons. In this article, we review the potential viability of atypical epige- Transcriptional alteration netic and/or consequent transcriptional alterations (ETAs) as biomarkers of early-stage neurodegenerative disease, and present our perspectives on the discovery and practical use of such biomarkers in patient-derived neural samples using single-cell level analyses, thereby greatly enhancing the reliability of biomarker applica- tion. 1. Introduction diagnostic biomarkers in neurodegenerative disease. Next, we in- troduce an integrative approach to discover these biomarkers by com- Neurodegenerative diseases, characterized by the physical decay of bining patient-derived neural organoids with single-cell level analyses disease-associated target neurons and the eventual loss of surrounding of epigenomic and/or consequent transcriptional profiles. -

Degenerative Disc Disease: a Review of Cell Technologies and Stem Cell Therapy Kaveh Haddadi1 *
Degenerative Disc Disease: A Review of Cell Technologies and Stem Cell Therapy Kaveh Haddadi1 * 1Assistant Professor, Department of Neurosurgery, Imam Khomeini hospital, Orthopedic Research Center, Mazandaran University Of Medical Sciences, Sari, Mazandaran, Iran *Corresponding Author Address: Department of Neurosurgery, Imam Khomeini hospital, Orthopedic Research Center, Mazandaran University Of Medical Sciences, Sari, Mazandaran, Iran. E mail:[email protected], Tel/Fax number: +98-11-33378789, Postal code: 48166-33131 Article Type: Review Article Received: September 2, 2015, Last revised: January 26, 2016, Accepted: March 19, 2016 Abstract Background & Aim: Low back pain is broadly documented as one of the most widespread pathologies in the advanced domain. Although the reasons of low back pain are uncountable, it has been meaningfully related to intervertebral disc degeneration. Present therapies for Intervertebral Disc (IVD) degeneration such as physical therapy and spinal fusion reduce symptoms' severity, but do not treat the source of degeneration. The use of tissue engineering to treat disc degeneration offers a chance to control the pathological course. New methods are presently being examined and have exposed mixed results. One major way of study has been stem cell injections. We go on to define the course of stem cell-mediated modalities in treatment of degenerative lumbar disc herniation Methods & Materials/Patients: Literature search was performed in electronic databases PUBMED and EMBASE by means of Mesh terminologies (Nucleus pulposus, therapeutics, annulus fibrosus, intervertebral disc) and keywords (Degenerative disk disease, Stem Cells, Therapy). Results: The intervertebral disc organization, developing treatments, mesenchymal stem cells, embryonic stem cells, practice in disc degeneration were some sections that were found in analysis for study review design. -

Anti-Aging: Radical Longevity, Environmental Impacts, and Christian Theology
Article Anti-Aging: Radical Longevity, Environmental Impacts, and Christian Theology Anti-Aging: Radical Longevity, Environmental Impacts, and Christian Theology Dorothy Boorse Current biomedical research shows promise for prolonging human life spans. Responses to these possible technologies vary from extreme caution, to exuberance, to a futuristic vision of humanity transforming itself. Bioethicists express concerns about big social and individual costs. Some views are expressed in the rhetoric of a culture war similar to those over cloning, stem cell research, and euthanasia. The possible effect on the environment is unknown. The biggest effect is likely to be on an increase in individual consumption of resources by a few and greater gaps between the rich and the poor. On a number of levels, radical longevity affects our view of self, humans in community, and our role in the natural world. I propose that prolonging human primary life span substantially is not a biblical mandate and is only appropriate when placed in the context of our role as humans and current environmental Dorothy Boorse and social issues. “Our technological abilities have outpaced our moral intuition” —Scholarship applicant, Gordon College 2001. n the 1998 novel The First Immortal,1 to elongate the natural human life span so Understanding Iauthor James Halperin paints a picture that people can live 150 years or longer.3 of a future world in which people rou- aging tinely have themselves frozen cryogenically until the day when scientists have cured can- Science: Why We Age, mechanisms cer and solved degenerative disorders. They Life Expectancy and can then thaw frozen people, solving their Life Span may help us medical problems so they live extremely Life expectancy, the mean likelihood of living long, almost immortal lives. -

Cellular Senescence and the Senescent Secretory Phenotype: Therapeutic Opportunities
Cellular senescence and the senescent secretory phenotype: therapeutic opportunities Tamara Tchkonia, … , Judith Campisi, James L. Kirkland J Clin Invest. 2013;123(3):966-972. https://doi.org/10.1172/JCI64098. Review Series Aging is the largest risk factor for most chronic diseases, which account for the majority of morbidity and health care expenditures in developed nations. New findings suggest that aging is a modifiable risk factor, and it may be feasible to delay age-related diseases as a group by modulating fundamental aging mechanisms. One such mechanism is cellular senescence, which can cause chronic inflammation through the senescence-associated secretory phenotype (SASP). We review the mechanisms that induce senescence and the SASP, their associations with chronic disease and frailty, therapeutic opportunities based on targeting senescent cells and the SASP, and potential paths to developing clinical interventions. Find the latest version: https://jci.me/64098/pdf Review series Cellular senescence and the senescent secretory phenotype: therapeutic opportunities Tamara Tchkonia,1 Yi Zhu,1 Jan van Deursen,1 Judith Campisi,2 and James L. Kirkland1 1Robert and Arlene Kogod Center on Aging, Mayo Clinic, Rochester, Minnesota, USA. 2Buck Institute for Research on Aging, Novato, California, USA. Aging is the largest risk factor for most chronic diseases, which account for the majority of morbidity and health care expenditures in developed nations. New findings suggest that aging is a modifiable risk factor, and it may be feasible to delay age-related diseases as a group by modulating fundamental aging mechanisms. One such mech- anism is cellular senescence, which can cause chronic inflammation through the senescence-associated secretory phenotype (SASP). -

Lumbar Degenerative Disease Part 1
International Journal of Molecular Sciences Article Lumbar Degenerative Disease Part 1: Anatomy and Pathophysiology of Intervertebral Discogenic Pain and Radiofrequency Ablation of Basivertebral and Sinuvertebral Nerve Treatment for Chronic Discogenic Back Pain: A Prospective Case Series and Review of Literature 1, , 1,2, 1 Hyeun Sung Kim y * , Pang Hung Wu y and Il-Tae Jang 1 Nanoori Gangnam Hospital, Seoul, Spine Surgery, Seoul 06048, Korea; [email protected] (P.H.W.); [email protected] (I.-T.J.) 2 National University Health Systems, Juronghealth Campus, Orthopaedic Surgery, Singapore 609606, Singapore * Correspondence: [email protected]; Tel.: +82-2-6003-9767; Fax.: +82-2-3445-9755 These authors contributed equally to this work. y Received: 31 January 2020; Accepted: 20 February 2020; Published: 21 February 2020 Abstract: Degenerative disc disease is a leading cause of chronic back pain in the aging population in the world. Sinuvertebral nerve and basivertebral nerve are postulated to be associated with the pain pathway as a result of neurotization. Our goal is to perform a prospective study using radiofrequency ablation on sinuvertebral nerve and basivertebral nerve; evaluating its short and long term effect on pain score, disability score and patients’ outcome. A review in literature is done on the pathoanatomy, pathophysiology and pain generation pathway in degenerative disc disease and chronic back pain. 30 patients with 38 levels of intervertebral disc presented with discogenic back pain with bulging degenerative intervertebral disc or spinal stenosis underwent Uniportal Full Endoscopic Radiofrequency Ablation application through either Transforaminal or Interlaminar Endoscopic Approaches. Their preoperative characteristics are recorded and prospective data was collected for Visualized Analogue Scale, Oswestry Disability Index and MacNab Criteria for pain were evaluated. -

Toxic Exposure and Life Style Factors on Ageing Brain Neurodegenerative Disease, Alzheimer’S and Parkinson’S: Role of Natural Antioxidants to Ameliorate the Condition
ism and D ol ru h g o lc D Naha et al., J Alcohol Drug Depend 2018, 6:2 e A p f e o n Journal of Alcoholism & Drug l DOI: 10.4172/2329-6488.1000309 d a e n r n c u o e J Dependence ISSN: 2329-6488 Review Article Open Access Toxic Exposure and, Life Style Factors, on Ageing Brain Neurodegenerative Disease, Alzheimer s and Parkinson s: Role of Natural Antioxidants to Ameliorate the Condition Nibedita Naha1*, Moitreyi Das2 and Arnab Banerjee3 1Biochemistry Division, ICMR-National Institute of Occupational Health, (Indian Council of Medical Research), Ahmedabad, Gujarat, India 2Department of Zoology, Goa University, Goa, India 3Department of Biological Sciences, BITS Pilani KK Birla Goa Campus, Goa, India *Corresponding author: Dr Nibedita Naha, Biochemistry Division, ICMR-National Institute of Occupational Health, (Indian Council of Medical Research), Ahmedabad 380016, Gujarat, India, Tel: +91-22688737; E-mail: [email protected] Received date: January 18, 2018; Accepted date: April 24, 2018; Published date: April 27, 2018 Copyright: © 2018 Naha N, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited. Abstract Toxic exposure is a major risk factor for many neurodegenerative diseases in ageing brain such as, Alzheimer’s (AD) and Parkinson’s (PD), where decline of biological activities in cellular microenvironment render the organism more susceptible to either endogenous or exogenous stressors especially free radical damage, leading to pathological conditions. -

Nanomedicine Further to Reduce Mortality in Developed Asks for Our Patience
major public investments are directed at only in the longer term. While it makes a References cancer treatments and thus at attempts compelling case for these promises, it also 1 Nanobiotechnology: Responsible Action on Issues in Society and Ethics: http://nanobio-raise.org/ 2 Mauro Magnani Eythrocyte Engineering for Drug Delivery and Targeting. New York: Kluwer, 2003. Nanomedicine further to reduce mortality in developed asks for our patience. And as with all basic 3 Volker Wagner and Axel Zweck Nanomedizin: Innovationspotenziale in Hessen für Medizintechnik und societies where it is already comparatively research, something is bound to come of Pharmazeutische Industrie Wiesbaden: Hessisches Ministerium für Wirtschaft, 2006. • A Brief History of Nanomedicine low. it, though not perhaps the full mastery of 4 Robert A. Freitas (1999): Nanomedicine, Volume I: Basic Capabilities, Georgetown, TX: Landes Bioscience. • Theranostics 5 physiological complexities that is envisioned Cancer NANOTECHNOLOGY: Going Small for Big Advances – Using Nanotechnology to Advance Cancer Diagnosis, • Targeted Drug-Delivery Prevention and Treatment. Washington, DC: U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES, National Nanomedical ethics should not serve to in the name of theranostics, individualised Institutes of Health, National Cancer Institute, 2004. • Polymer Therapeutics validate an uncertain future, for example, medicine, and cell repair. Some of its 6 Nanomedicine: Nanotechnology for Health – European Technology Platform. Brussels: European Commission, • Regenerative Medicine by assuming too readily an increase of most important contributions will consist Research DG, 2006, p. 12. • Ethical and societal issues 7 Ibid., p. 10, see also p. 6 and especially p. 12. diagnostic powers or an impact on life- of progress in instrumentation and analytic 8 Nanomedicine: An ESF – European Medical Research Councils (EMRC) Forward Look report. -

Role of NF-Κb in Ageing and Age-Related Diseases: Lessons from Genetically Modified Mouse Models
cells Review Role of NF-κB in Ageing and Age-Related Diseases: Lessons from Genetically Modified Mouse Models Verónica A. García-García 1,2, Josefa P. Alameda 1,2,3, Angustias Page 1,2,3 and María Llanos Casanova 1,2,3,* 1 Molecular and Translational Oncology Unit, Centro de Investigaciones Energéticas, Medioambientales y Tecnológicas (CIEMAT), 28040 Madrid, Spain; [email protected] (V.A.G.-G.); [email protected] (J.P.A.); [email protected] (A.P.) 2 Biomedical Research Institute I+12, 12 de Octubre University Hospital, 28040 Madrid, Spain 3 Centro de Investigación Biomédica en Red de Cáncer (CIBERONC), 28029 Madrid, Spain * Correspondence: [email protected] Abstract: Ageing is a complex process, induced by multifaceted interaction of genetic, epigenetic, and environmental factors. It is manifested by a decline in the physiological functions of organisms and associated to the development of age-related chronic diseases and cancer development. It is considered that ageing follows a strictly-regulated program, in which some signaling pathways critically contribute to the establishment and maintenance of the aged state. Chronic inflammation is a major mechanism that promotes the biological ageing process and comorbidity, with the transcription factor NF-κB (nuclear factor kappa-light-chain-enhancer of activated B cells) as a crucial mediator of inflammatory responses. This, together with the finding that the activation or inhibition of NF- κ B can induce or reverse respectively the main features of aged organisms, has brought it under consideration as a key transcription factor that acts as a driver of ageing. In this review, we focused on the data obtained entirely through the generation of knockout and transgenic mouse models of Citation: García-García, V.A.; Alameda, J.P.; Page, A.; Casanova, either protein involved in the NF-κB signaling pathway that have provided relevant information M.L. -

Average Lifespan Almost Doubled During the Last Century, While The
The Politics of Dying: Does the End of Life have to be Hell? Guy C. Brown & Sarah A. Radcliffe Average lifespan almost doubled during the last century, while the rate at which we age remained the same, resulting in dramatic changes in the nature of old age and death. The last few years of life before death are increasingly consumed by chronic disease, disability, dementia and extreme aging. We argue that this bleak fate is not inevitable, but rather the consequence of our past social and medical culture, and therefore can and should be changed. Is it inevitable that dying and the last few years of life are horrors? Does it have to be this way? It is tempting to think that aging and chronic death from old age are ‘natural’, while acute death of the young is somehow unnatural. However, the exact opposite is the case. Significant aging and degenerative disease are rare in wild animals, and were uncommon in humans up until two hundred years ago. Why? Because they died comparatively young, before they had time to age significantly. The average human lifespan was about 30 years before 1800, but since then has been increasing at about 2 years per decade in the UK. So that current life expectancy is about 80 in the UK, and should reach 100 years by the end of the century. Only in the unnatural conditions of modern society and medicine can the exotic diseases and deaths of old age flourish. Death is certainly not what it was. Life in the past was once described as “nasty, brutish and short”, but this would be a better description of Death throughout most of history. -
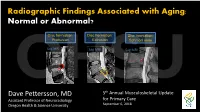
Radiographic Findings Associated with Aging: Normal Or Abnormal?
Radiographic Findings Associated with Aging: Normal or Abnormal? Disc herniation: Disc herniation: Disc herniation: Protrusion Extrusion Schmorl node OHSUSag MRI Sag MRI Sag MRI Dave Pettersson, MD 5th Annual Musculoskeletal Update Assistant Professor of Neuroradiology for Primary Care Oregon Health & Science University September 6, 2018 Spine Imaging and Aging: Disclosures: Outline: Nothing to disclose Spine degenerative changes on imaging: • Prevalence • Appearance on MRI, CT, radiographs Low back pain • When to image OHSU• “Red flag” conditions Age-related changes on brain MRI Spine Imaging and Aging: Question What percentage of asymptomatic 20-year-olds have degenerative disc findings on lumbar spine MRI? A. 5 % B. 15 % C. 25 % D. 35 % OHSUE. 45% Spine Imaging and Aging: Question What percentage of asymptomatic 80-year-olds have degenerative disc findings on lumbar spine MRI? A. 35 % B. 55 % C. 75 % OHSUD. 95% Spine Imaging and Aging: Answers Disc protrusion OHSU Prevalence of degenerative findings on Lumbar MRI: • 148 volunteers • All asymptomatic at time of MRI • 46% reported never having back pain AgeOHSU under 40 years: Age under 40-60 years: Age over 60 years: Disc herniation: Disc herniation: Diffuse disc Disc herniation: Protrusion Extrusion bulge Schmorl node Sag MRI Sag MRI Sag MRI Sag MRI Axial MRI Axial MRI AxialOHSU MRI Axial MRI To qualify as a disc extrusion A disc protrusion (red) involves (red) the neck of the disc An intravertebral disc less than 25% of the disc A diffusely bulging disc (red) material must be narrower herniation (red) aka circumference and has a wide involves greater than 25% of the than the material outside the base of attachment. -

Advances in Nanotechnology-Based Strategies for the Treatments of Amyotrophic Lateral Sclerosis
Materials Today Bio 6 (2020) 100055 Contents lists available at ScienceDirect Materials Today Bio journal homepage: www.journals.elsevier.com/materials-today-bio Advances in nanotechnology-based strategies for the treatments of amyotrophic lateral sclerosis G.Y. Wang a,b, S.L. Rayner b, R. Chung b, B.Y. Shi b,c,**, X.J. Liang d,* a Huaihe Hospital, Henan University, Kaifeng, Henan, 475004, China b Centre for Motor Neuron Disease Research, Department of Biomedical Sciences, Faculty of Medicine & Health Sciences, Macquarie University, Sydney, NSW 2109, Australia c Henan-Macquarie University Joint Centre for Biomedical Innovation, School of Life Sciences, Henan University, Kaifeng, Henan, 475004, China d Key Laboratory for Biological Effects of Nanomaterials and Nanosafety, National Center for Nanoscience and Technology, Chinese Academy of Sciences, Beijing, 100190, China ARTICLE INFO ABSTRACT Keywords: Amyotrophic lateral sclerosis (ALS), also known as motor neuron disease (MND), is a progressive neurodegen- Nanotechnology erative disease that affects both upper and lower motor neurons, which results in loss of muscle control and Amyotrophic lateral sclerosis (ALS) eventual paralysis [1]. Currently, there are as yet unresolved challenges regarding efficient drug delivery into the Blood-brain barrier central nervous system (CNS). These challenges can be attributed to multiple factors including the presence of the Neurodegenerative diseases blood-brain barrier (BBB), blood-spinal cord barrier (BSCB), as well as the inherent characteristics of the drugs Central nervous system (CNS) themselves (e.g. low solubility, insufficient bioavailability/bio-stability, 'off-target' effects) etc. As a result, con- ventional drug delivery systems may not facilitate adequate dosage of the required drugs for functional recovery in ALS patients. -

Fibroblasts As a Practical Alternative to Mesenchymal Stem Cells Thomas E
Ichim et al. J Transl Med (2018) 16:212 https://doi.org/10.1186/s12967-018-1536-1 Journal of Translational Medicine REVIEW Open Access Fibroblasts as a practical alternative to mesenchymal stem cells Thomas E. Ichim1*†, Pete O’Heeron1† and Santosh Kesari2 Abstract Mesenchymal stem cell (MSC) therapy ofers great potential for treatment of disease through the multifunctional and responsive ability of these cells. In numerous contexts, MSC have been shown to reduce infammation, modulate immune responses, and provide trophic factor support for regeneration. While the most commonly used MSC source, the bone marrow provides relatively little starting material for cellular expansion, and requires invasive extraction means, fbroblasts are easily harvested in large numbers from various biological wastes. Additionally, in vitro expan- sion of fbroblasts is signifcantly easier given the robustness of these cells in tissue culture and shorter doubling time compared to typical MSC. In this paper we put forward the concept that in some cases, fbroblasts may be utilized as a more practical, and potentially more efective cell therapy than mesenchymal stem cells. Anti-infammatory, immune modulatory, and regenerative properties of fbroblasts will be discussed in the context of regenerative medicine. Keywords: Stem cell therapy, Regenerative medicine, Disc degenerative disease, Fibroblasts, Mesenchymal stem cells Introduction to other bone marrow mononuclear cells, specifcally, Friedenstein and colleagues were the frst to describe 1:10,000 to 1:100,000 [14]. Te physiological role of MSC mesenchymal stem cells (MSC) as adherent cells derived still remains to be fully elucidated, with one hypoth- from bone marrow that were capable of forming colonies esis being that bone marrow MSC act as precursors for and comprising the radioresistant fraction of cells associ- stromal cells that make up the hematopoietic stem cell ated with hematopoiesis [1, 2].