Testing and Serological Markers of Hepatitis B Virus
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Inhibition of HIV-1 by an Anti-Integrase Single-Chain Variable
Gene Therapy (1999) 6, 660–666 1999 Stockton Press All rights reserved 0969-7128/99 $12.00 http://www.stockton-press.co.uk/gt Inhibition of HIV-1 by an anti-integrase single-chain variable fragment (SFv): delivery by SV40 provides durable protection against HIV-1 and does not require selection M BouHamdan1, L-X Duan1, RJ Pomerantz1 and DS Strayer1,2 1The Dorrance H Hamilton Laboratories, Center for Human Virology, Division of Infectious Diseases, Department of Medicine; and 2Department of Pathology, Anatomy and Cell Biology, Jefferson Medical College, Thomas Jefferson University, Philadelphia, PA, USA Human immunodeficiency virus type I (HIV-1) encodes the SFv-IN was confirmed by Western blotting and several proteins that are packaged into virus particles. Inte- immunofluorescence staining, which showed that Ͼ90% of grase (IN) is an essential retroviral enzyme, which has SupT1 T-lymphocytic cells treated with SV(Aw) expressed been a target for developing agents to inhibit virus repli- the SFv-IN protein without selection. When challenged, cation. In previous studies, we showed that intracellular HIV-1 replication, as measured by HIV-1 p24 antigen expression of single-chain variable antibody fragments expression and syncytium formation, was potently inhibited (SFvs) that bind IN, delivered via retroviral expression vec- in cells expressing SV40-delivered SFv-IN. Levels of inhi- tors, provided resistance to productive HIV-1 infection in bition of HIV-1 infection achieved using this approach were T-lymphocytic cells. In the current studies, we evaluated comparable to those achieved using murine leukemia virus simian-virus 40 (SV40) as a delivery vehicle for anti-IN (MLV) as a transduction vector, the major difference being therapy of HIV-1 infection. -

Evolution of Hepatitis B Serological Markers in HIV Coinfected Patients: a Case Study
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Cadernos Espinosanos (E-Journal) Rev Saúde Pública 2017;51:24 Artigo Original http://www.rsp.fsp.usp.br/ Evolution of hepatitis B serological markers in HIV coinfected patients: a case study Ana Luiza de Castro Conde ToscanoI,II, Maria Cássia Mendes CorrêaII,III I Instituto de Infectologia Emílio Ribas. São Paulo, SP, Brasil II Departamento de Doenças Infecciosas. Faculdade de Medicina. Universidade de São Paulo. São Paulo, SP, Brasil III Instituto de Medicina Tropical de São Paulo. Laboratório de Investigação Médica 52. São Paulo, SP, Brasil ABSTRACT OBJECTIVE: To describe the evolution of serological markers among HIV and hepatitis B coinfected patients, with emphasis on evaluating the reactivation or seroreversion of these markers. METHODS: The study population consisted of patients met in an AIDS Outpatient Clinic in São Paulo State, Brazil. We included in the analysis all HIV-infected and who underwent at least two positive hepatitis B surface antigen serological testing during clinical follow up, with tests taken six months apart. Patients were tested with commercial kits available for hepatitis B serological markers by microparticle enzyme immunoassay. Clinical variables were collected: age, sex, CD4+ T-cell count, HIV viral load, alanine aminotransferase level, exposure to antiretroviral drugs including lamivudine and/or tenofovir. RESULTS: Among 2,242 HIV positive patients, we identified 105 (4.7%) patients with chronic hepatitis B. Follow up time for these patients varied from six months to 20.5 years. All patients underwent antiretroviral therapy during follow-up. Among patients with chronic hepatitis B, 58% were hepatitis B “e” antigen positive at the first assessment. -
Covalent Protein Display on Hepatitis B Core-Like Particles in Plants
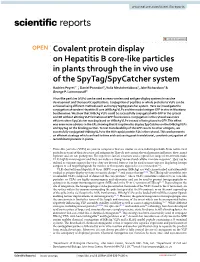
www.nature.com/scientificreports OPEN Covalent protein display on Hepatitis B core‑like particles in plants through the in vivo use of the SpyTag/SpyCatcher system Hadrien Peyret1*, Daniel Ponndorf1, Yulia Meshcheriakova1, Jake Richardson2 & George P. Lomonossof1 Virus‑like particles (VLPs) can be used as nano‑carriers and antigen‑display systems in vaccine development and therapeutic applications. Conjugation of peptides or whole proteins to VLPs can be achieved using diferent methods such as the SpyTag/SpyCatcher system. Here we investigate the conjugation of tandem Hepatitis B core (tHBcAg) VLPs and the model antigen GFP in vivo in Nicotiana benthamiana. We show that tHBcAg VLPs could be successfully conjugated with GFP in the cytosol and ER without altering VLP formation or GFP fuorescence. Conjugation in the cytosol was more efcient when SpyCatcher was displayed on tHBcAg VLPs instead of being fused to GFP. This efect was even more obvious in the ER, showing that it is optimal to display SpyCatcher on the tHBcAg VLPs and SpyTag on the binding partner. To test transferability of the GFP results to other antigens, we successfully conjugated tHBcAg VLPs to the HIV capsid protein P24 in the cytosol. This work presents an efcient strategy which can lead to time and cost saving post‑translational, covalent conjugation of recombinant proteins in plants. Virus-like particles (VLPs) are protein complexes that are similar or even indistinguishable from native viral particles in terms of their structure and antigenicity. Tey do not contain the viral genome and hence, they cannot replicate and are not pathogenic. Te repetitive surface structure and a typical size range of 20–200 nm make VLPs highly immunogenic and they can induce a strong humoral and cellular immune response1. -

A Rapid Immunochromatographic Method Based on a Secondary Antibody-Labelled Magnetic Nanoprobe for the Detection of Hepatitis B Pres2 Surface Antigen
biosensors Article A Rapid Immunochromatographic Method Based on a Secondary Antibody-Labelled Magnetic Nanoprobe for the Detection of Hepatitis B preS2 Surface Antigen Yangyang Cai 1,2,3, Jun Yan 1,2,3, Li Zhu 4, Hengliang Wang 4 and Ying Lu 1,2,3,* 1 College of Food Science and Technology, Shanghai Ocean University, Shanghai 201306, China; [email protected] (Y.C.); [email protected] (J.Y.) 2 Laboratory of Quality & Safety Risk Assessment for Aquatic Products on Storage and Preservation (Shanghai), Ministry of Agriculture, Shanghai 201306, China 3 Shanghai Engineering Research Center of Aquatic-Product Processing and Preservation, Shanghai 201306, China 4 Beijing Institute of Biotechnology, Beijing 100071, China; [email protected] (L.Z.); [email protected] (H.W.) * Correspondence: [email protected]; Tel.: +86-021-6190-0503 Received: 24 September 2020; Accepted: 27 October 2020; Published: 31 October 2020 Abstract: Hepatitis B is a globally prevalent viral infectious disease caused by the hepatitis B virus (HBV). In this study, an immunochromatographic assay (ICA) for the rapid detection of hepatitis B preS2 antigen (preS2Ag) was established. The magnetic nanoparticles (MNPs) indirectly labelled with goat anti-mouse (GAM) secondary antibody were applied as a nanoprobe for free preS2 antibody (preS2Ab) capturing and signal amplification. By employing sample pre-incubation processing as well, preS2Ag-preS2Ab was sufficiently caught by the GAM-MNPs probe in 5 min. A qualitative sensitivity of 625 ng/mL was obtained by naked-eye observation within 15–20 min. A standard curve (0–5000 ng/mL) was established, with a quantitative limit of detection (LOD) of 3.6 ng/mL, based on the stability and penetrability of the magnetic signal characteristics. -

Herpes Simplex Virus Type 1 Oril Is Not Required for Virus Infection In
JOURNAL OF VIROLOGY, Nov. 1987, p. 3528-3535 Vol. 61, No. 11 0022-538X/87/113528-08$02.00/0 Copyright C 1987, American Society for Microbiology Herpes Simplex Virus Type 1 oriL Is Not Required for Virus Replication or for the Establishment and Reactivation of Latent Infection in Mice MARYELLEN POLVINO-BODNAR, PAULO K. ORBERG, AND PRISCILLA A. SCHAFFER* Laboratory of Tumor Virus Genetics, Dana-Farber Cancer Institute, and Department of Microbiology and Molecular Genetics, Harvard Medical School, Boston, Massachusetts 02115 Received 11 May 1987/Accepted 31 July 1987 During the course of experiments designed to isolate deletion mutants of herpes simplex virus type 1 in the gene encoding the major DNA-binding protein, ICP8, a mutant, d61, that grew efficiently in ICP8-expressing Vero cells but not in normal Vero cells was isolated (P. K. Orberg and P. A. Schaffer, J. Virol. 61:1136-1146, 1987). d61 was derived by cotransfection of ICP8-expressing Vero cells with infectious wild-type viral DNA and a plasmid, pDX, that contains an engineered 780-base-pair (bp) deletion in the ICP8 gene, as well as a spontaneous -55-bp deletion in OriL. Gel electrophoresis and Southern blot analysis indicated that d61 DNA carried both deletions present in pDX. The ability of d61 to replicate despite the deletion in OriL suggested that a functional OriL is not essential for virus replication in vitro. Because d61 harbored two mutations, a second mutant, ts+7, with a deletion in oriL-associated sequences and an intact ICP8 gene was constructed. Both d61 and ts+7 replicated efficiently in their respective permissive host cells, although their yields were slightly lower than those of control viruses with intact oriL sequences. -

Direct Acting Antivirals for the Treatment of Chronic Viral Hepatitis
Hindawi Publishing Corporation Scienti�ca Volume 2012, Article ID 478631, 22 pages http://dx.doi.org/10.6064/2012/478631 Review Article Direct Acting Antivirals for the Treatment of Chronic Viral Hepatitis Peter Karayiannis Section of Hepatology and Gastroenterology, Department of Medicine, Imperial College, St Mary’s Campus, London W2 1PG, UK Correspondence should be addressed to Peter Karayiannis; [email protected] Received 17 September 2012; Accepted 8 October 2012 Academic Editors: M. Clementi and W. Vogel Copyright © 2012 Peter Karayiannis. is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. e development and evaluation of antiviral agents through carefully designed clinical trials over the last 25 years have heralded a new dawn in the treatment of patients chronically infected with the hepatitis B and C viruses, but not so for the D virus (HBV, HCV, and HDV). e introduction of direct acting antivirals (DDAs) for the treatment of HBV carriers has permitted the long- term use of these compounds for the continuous suppression of viral replication, whilst in the case of HCV in combination with the standard of care [SOC, pegylated interferon (PegIFN), and ribavirin] sustained virological responses (SVRs) have been achieved with increasing frequency. Progress in the case of HDV has been slow and lacking in signi�cant breakthroughs.is paper aims to summarise the current state of play in treatment approaches for chonic viral hepatitis patients and future perspectives. 1. Introduction recombinant subsequently, both of which have more recently been superceded by the pegylated form (PegIFN), which Conservative estimates of the number of individuals world- requires intramuscular injection only once a week as opposed wide who are thought to be chronically infected with either to three times a week with the previous forms. -

Topological Analysis of the Gp41 MPER on Lipid Bilayers Relevant to the Metastable HIV-1 Envelope Prefusion State
Topological analysis of the gp41 MPER on lipid bilayers relevant to the metastable HIV-1 envelope prefusion state Yi Wanga,b, Pavanjeet Kaurc,d, Zhen-Yu J. Sune,1, Mostafa A. Elbahnasawya,b,2, Zahra Hayatic,d, Zhi-Song Qiaoa,b,3, Nhat N. Buic, Camila Chilea,b,4, Mahmoud L. Nasre,5, Gerhard Wagnere, Jia-Huai Wanga,f, Likai Songc, Ellis L. Reinherza,b,6, and Mikyung Kima,g,6 aLaboratory of Immunobiology, Department of Medical Oncology, Dana-Farber Cancer Institute, Boston, MA 02115; bDepartment of Medicine, Harvard Medical School, Boston, MA 02115; cNational High Magnetic Field Laboratory, Florida State University, Tallahassee, FL 32306; dDepartment of Physics, Florida State University, Tallahassee, FL 32306; eDepartment of Biological Chemistry and Molecular Pharmacology, Harvard Medical School, Boston, MA 02115; fDepartment of Cancer Biology, Dana-Farber Cancer Institute, Boston, MA 02215; and gDepartment of Dermatology, Harvard Medical School, Boston, MA 02215 Edited by Peter Palese, Icahn School of Medicine at Mount Sinai, New York, NY, and approved September 23, 2019 (received for review July 18, 2019) The membrane proximal external region (MPER) of HIV-1 envelope immunologically vulnerable epitopes targeted by several of the most glycoprotein (gp) 41 is an attractive vaccine target for elicitation of broadly neutralizing antibodies (bNAbs) developed during the broadly neutralizing antibodies (bNAbs) by vaccination. However, course of natural HIV-1 infection (10–13). Insertion, deletion, current details regarding the quaternary structural organization of and mutations of residues in the MPER defined the functional the MPER within the native prefusion trimer [(gp120/41)3] are elu- importance of the MPER in Env incorporation, viral fusion, and sive and even contradictory, hindering rational MPER immunogen infectivity (14–16). -

Viroporins: Structures and Functions Beyond Cell Membrane Permeabilization
Editorial Viroporins: Structures and Functions beyond Cell Membrane Permeabilization José Luis Nieva 1,* and Luis Carrasco 2,* Received: 17 September 2015 ; Accepted: 21 September 2015 ; Published: 29 September 2015 Academic Editor: Eric O. Freed 1 Biophysics Unit (CSIC, UPV/EHU) and Biochemistry and Molecular Biology Department, University of the Basque Country (UPV/EHU), P.O. Box 644, 48080 Bilbao, Spain 2 Centro de Biología Molecular Severo Ochoa (CSIC, UAM), c/Nicolás Cabrera, 1, Universidad Autónoma de Madrid, Cantoblanco, 28049 Madrid, Spain * Correspondence: [email protected] (J.L.N.); [email protected] (L.C.); Tel.: +34-94-601-3353 (J.L.N.); +34-91-497-8450 (L.C.) Viroporins represent an interesting group of viral proteins that exhibit two sets of functions. First, they participate in several viral processes that are necessary for efficient production of virus progeny. Besides, viroporins interfere with a number of cellular functions, thus contributing to viral cytopathogenicity. Twenty years have elapsed from the first review on viroporins [1]; since then several reviews have covered the advances on viroporin structure and functioning [2–8]. This Special Issue updates and revises new emerging roles of viroporins, highlighting their potential use as antiviral targets and in vaccine development. Viroporin structure. Viroporins are usually short proteins with at least one hydrophobic amphipathic helix. Homo-oligomerization is achieved by helix–helix interactions in membranes rendering higher order structures, forming aqueous pores. Progress in viroporin structures during the last 2–3 years has in some instances provided a detailed knowledge of their functional architecture, including the fine definition of binding sites for effective inhibitors. -

How Influenza Virus Uses Host Cell Pathways During Uncoating
cells Review How Influenza Virus Uses Host Cell Pathways during Uncoating Etori Aguiar Moreira 1 , Yohei Yamauchi 2 and Patrick Matthias 1,3,* 1 Friedrich Miescher Institute for Biomedical Research, 4058 Basel, Switzerland; [email protected] 2 Faculty of Life Sciences, School of Cellular and Molecular Medicine, University of Bristol, Bristol BS8 1TD, UK; [email protected] 3 Faculty of Sciences, University of Basel, 4031 Basel, Switzerland * Correspondence: [email protected] Abstract: Influenza is a zoonotic respiratory disease of major public health interest due to its pan- demic potential, and a threat to animals and the human population. The influenza A virus genome consists of eight single-stranded RNA segments sequestered within a protein capsid and a lipid bilayer envelope. During host cell entry, cellular cues contribute to viral conformational changes that promote critical events such as fusion with late endosomes, capsid uncoating and viral genome release into the cytosol. In this focused review, we concisely describe the virus infection cycle and highlight the recent findings of host cell pathways and cytosolic proteins that assist influenza uncoating during host cell entry. Keywords: influenza; capsid uncoating; HDAC6; ubiquitin; EPS8; TNPO1; pandemic; M1; virus– host interaction Citation: Moreira, E.A.; Yamauchi, Y.; Matthias, P. How Influenza Virus Uses Host Cell Pathways during 1. Introduction Uncoating. Cells 2021, 10, 1722. Viruses are microscopic parasites that, unable to self-replicate, subvert a host cell https://doi.org/10.3390/ for their replication and propagation. Despite their apparent simplicity, they can cause cells10071722 severe diseases and even pose pandemic threats [1–3]. -
Assembly Lecture 11 Biology W3310/4310 Virology Spring 2014
Assembly Lecture 11 Biology W3310/4310 Virology Spring 2014 “Anatomy is des.ny.” --SIGMUND FREUD All virions complete a common set of assembly reac3ons * common to all viruses common to many viruses ©Principles of Virology, ASM Press The structure of a virus parcle determines how it is formed ©Principles of Virology, ASM Press Assembly is dependent on host cell machinery • Cellular chaperones • Transport systems • Secretory pathway • Nuclear import and export machinery Concentrang components for assembly: Nothing happens fast in dilute solu1ons • Viral components oSen visible by light microscopy (‘factories’ or ‘inclusions’) • Concentrate proteins on internal membranes (poliovirus) • Negri bodies (rabies virus) Viral proteins have ‘addresses’ built into their structure • Membrane targeYng: Signal sequences, fa\y acid modificaons • Membrane retenYon signals • Nuclear localizaYon sequences (NLS) • Nuclear export signals 414 Localiza3on of viral proteins to the nucleus CHAPTER 12 Golgi apparatus Ribosome Rough endoplasmic reticulum Plasma membrane Py(VP1) + VP2/3 Ad hexon + 5 100 kDa Nuclear envelope: Outer nuclear membrane Inner nuclear membrane Nucleus Nuclear pore complex Mitochondrion Cytoskeleton: Influenza virus NP Intermediate filament Microtubule Actin filament bundle Extracellular matrix ©Principles of Virology, ASM Press Figure 12.1 Localization of viral proteins to the nucleus. The nucleus and major membrane-bound compartments of the cytoplasm, as well as components of the cytoskeleton, are illustrated schematically and not to scale. Viral proteins destined for the nucleus are synthesized by cytoplasmic polyribosomes, as illustrated for the infl uenza virus NP protein. They engage with the cytoplasmic face of the nuclear pore complex and are translocated into the nucleus by the protein import machinery of the host cell. -

Producing Vaccines Against Enveloped Viruses in Plants: Making the Impossible, Difficult
Review Producing Vaccines against Enveloped Viruses in Plants: Making the Impossible, Difficult Hadrien Peyret , John F. C. Steele † , Jae-Wan Jung, Eva C. Thuenemann , Yulia Meshcheriakova and George P. Lomonossoff * Department of Biochemistry and Metabolism, John Innes Centre, Norwich NR4 7UH, UK; [email protected] (H.P.); [email protected] (J.F.C.S.); [email protected] (J.-W.J.); [email protected] (E.C.T.); [email protected] (Y.M.) * Correspondence: [email protected] † Current address: Piramal Healthcare UK Ltd., Piramal Pharma Solutions, Northumberland NE61 3YA, UK. Abstract: The past 30 years have seen the growth of plant molecular farming as an approach to the production of recombinant proteins for pharmaceutical and biotechnological uses. Much of this effort has focused on producing vaccine candidates against viral diseases, including those caused by enveloped viruses. These represent a particular challenge given the difficulties associated with expressing and purifying membrane-bound proteins and achieving correct assembly. Despite this, there have been notable successes both from a biochemical and a clinical perspective, with a number of clinical trials showing great promise. This review will explore the history and current status of plant-produced vaccine candidates against enveloped viruses to date, with a particular focus on virus-like particles (VLPs), which mimic authentic virus structures but do not contain infectious genetic material. Citation: Peyret, H.; Steele, J.F.C.; Jung, J.-W.; Thuenemann, E.C.; Keywords: alphavirus; Bunyavirales; coronavirus; Flaviviridae; hepatitis B virus; human immunode- Meshcheriakova, Y.; Lomonossoff, ficiency virus; Influenza virus; newcastle disease virus; plant molecular farming; plant-produced G.P. -

Virus-Host Interaction: the Multifaceted Roles of Ifitms And
Virus-Host Interaction: The Multifaceted Roles of IFITMs and LY6E in HIV Infection DISSERTATION Presented in Partial Fulfillment of the Requirements for the Degree Doctor of Philosophy in the Graduate School of The Ohio State University By Jingyou Yu Graduate Program in Comparative and Veterinary Medicine The Ohio State University 2018 Dissertation Committee: Shan-Lu Liu, MD, PhD, Advisor Patrick L. Green, PhD Jianrong Li, DVM., PhD Jesse J. Kwiek, PhD Copyrighted by Jingyou Yu 2018 Abstract With over 1.8 million newly infected people each year, the worldwide HIV-1 epidemic remains an imperative challenge for public health. Recent work has demonstrated that type I interferons (IFNs) efficiently suppress HIV infection through induction of hundreds of interferon stimulated genes (ISGs). These ISGs target distinct infection stages of invading pathogens and shape innate immunity. Among these, interferon induced transmembrane proteins (IFITMs) and lymphocyte antigen 6 complex, locus E (LY6E) have been shown to differentially modulate viral infections. However, their effects on HIV are not fully understood. In my thesis work, I provided evidence in Chapter 2 showing that IFITM proteins, particularly IFITM2 and IFITM3, specifically antagonize the HIV-1 envelope glycoprotein (Env), thereby inhibiting viral infection. IFITM proteins interacted with HIV-1 Env in viral producer cells, leading to impaired Env processing and virion incorporation. Notably, the level of IFITM incorporation into HIV-1 virions did not strictly correlate with the extent of inhibition. Prolonged passage of HIV-1 in IFITM-expressing T lymphocytes led to emergence of Env mutants that overcome IFITM restriction. The ability of IFITMs to inhibit cell-to-cell infection can be extended to HIV-1 primary isolates, HIV-2 and SIVs; however, the extent of inhibition appeared to be virus- strain dependent.