Report. an Update on Effective Approaches for Gender-Integrated
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Tostan and the Sustainable Development Goals
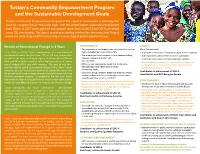
Tostan’s Community Empowerment Program and the Sustainable Development Goals Tostan’s Community Empowerment Program (CEP) supports communities in achieving their vision for a brighter future. That vision aligns with the United Nations Sustainable Development Goals (SDGs). In 2017 Tostan gathered and analyzed results from its 2013-2016 CEP implemented across 150 communities. This data is providing an exciting window into the impact that Tostan’s model and community-led efforts are having on a wide range of globally significant issues. Results of Generational Change in 3 Years GOVERNANCE HEALTH » The proportion of participants who now know their human More than doubled: From 2013 to 2016, Tostan implemented its transformational rights multiplied by 5 from 13% to 70%. » % of women who discuss family planning with their husbands development model, the three-year CEP, in 150 new communities » There were significant increases in joint decision-making » # of respondents whose children receive vaccinations in some of the most challenging regions of Guinea, Guinea Bissau, between husband and wife in all » % of respondents who used oral rehydration solution four countries. Mali, and Mauritania; countries with a high prevalence of female “ We have a health center here…; now when a child gets sick, genital cutting (FGC) and child marriage. The goal of this four- » 90% of survey respondents stated that Community we bring him to the health center. That is because of the country initiative, called ‘Generational Change in Three Years', was to Management Committees (CMCs) satisfy teaching Tostan gave us.” – MALI community needs. empower girls and women and significantly expand the movement Contributes to achievement of SDG 3: » CMC focus group members stated that they had helped for positive social norms change through the abandonment of these Good Health and Well-Being for People harmful traditional practices. -

TODAY. TOMORROW. TOGETHER. TOSTAN ANNUAL REPORT 2014 Table of Contents
TODAY. TOMORROW. TOGETHER. TOSTAN ANNUAL REPORT 2014 Table of Contents Message From the Founder and CEO .................................. 4 Tostan Training Center .................................. 18 Setting the Stage to Share the Tostan Model Letter from the Board .................................. 5 Child Protection Project .................................. 20 Mission and Vision .................................. 6 Modernizing Daaras for a Future Without Forced Begging Approach, Methodology, Strategy .................................. 6 Empowered Communities Network .................................. 22 2014 Highlights .................................. 8 Creating Connections to Achieve a Vision Generational Change in Three Years .................................. 10 Obstetric Fistula Project .................................. 24 A New Model for Social Transformation Raising Awareness for Prevention and Response Peace and Security .................................. 12 Building a Bridge to Peace Prison Project .................................. 26 Reinforcement of Parental Practices .................................. 14 Working Toward Reintegration Parents Who Invest in Early Childhood, Invest in the Future Spotlight on our Supporters .................................. 28 Monitoring, Evaluation, Research & Learning .................................. 16 Donors .................................. 32 Building a Solid Foundation for Tostan’s Future Special Thanks .................................. 33 Financials ................................. -

Resilience Beyond COVID-19 March–September 2020 Report Primary Action Taken
Resilience Beyond COVID-19 March–September 2020 Report Primary Action Taken In March 2020, due to the COVID-19 pandemic, Tostan made the difficult decision to suspend all field activities in its five focus countries (The Gambia, Guinea, Guinea-Bissau, Mali, Senegal) for the duration of the emergency. All field staff had to leave the partner communities where they were living and return home. Tostan rapidly implemented a COVID-19 response contingency plan aimed at providing community members with life-saving information on the virus, delivered in the local languages and in a culturally appropriate manner. The ultimate goal of the contingency plan was to curb the virus spread and to protect lives through the measures outlined below: 1. Developed and distributed COVID-19 informational brochures in 13 languages Tostan developed two brochures with key COVID-19 prevention messages. Illustrations depicted local housing, practices, and dress and advice was tailored to address any social norms that may be affected by the virus. One brochure offers culturally relevant information and illustrations about the virus transmission and prevention; and one discussing an Islamic perspective on the virus. Both versions of the brochures have been widely distributed to partner communities and are also available free to download from Tostan’s website. 2. Broadcasted radio programs to inform Tostan partner communities In addition to providing basic information on coronavirus transmission and prevention, Tostan radio programs covered topics such as community-government collaboration during the pandemic, religious texts that reinforce public health measures, and education in the time of COVID. 3. Collected data to inform programming Working with IDinsight, a global analytics organization, Tostan gathered data to better understand the knowledge, attitudes, and practices around COVID in the areas where Tostan is working. -

Annual Report 2011
Annual Report 2011 Front cover photograph: CEP participant during the 3rd Annual Youth Caravan in The Gambia Community members of Saam Njaay welcome Tostan during the 2011 Annual Retreat Contents 5 Letter from the Executive Director 6 2011 at a Glance 8 Overview 12 Country Updates 23 Our Offices 27 Strategic Update 30 Financials 33 List of Supporters 34 Glossary of Key Terms Contents 3 4 Tostan Annual Report 2011 CEP participant during the 3rd Annual Youth Caravan in The Gambia Letter from the Executive Director Dear Friends and Supporters, 2011 was a landmark year for Tostan as we celebrated our 20th anniversary. When we first began implementing the Community Empowerment Program (CEP) in Senegal all those years ago, I could never have dreamed that now, 20 years later, over 200,000 people in eight countries would have participated in our program, and millions more reached. Even though we have grown significantly, I am proud that we are still the same organization at heart, dedicated to African communities and our vision of human dignity for all. As we were 20 years ago, we remain grateful to our tireless local staff, especially our community facilitators, supervisors, and regional and national teams whose dedication creates the circle in which our community partners dance. We are also incredibly thankful to our long term donors and supporters and in particular to UNICEF, who has been with this from the very beginning. In our report, you will see updates from each of the eight countries in which we work across West and East Africa, as well as news from our vital family members in Tostan International and our sister organizations in Canada, France, and Sweden. -
Costs and Considerations
COSTS AND CONSIDERATIONS Volunteer Program Tostan Volunteer Program – Costs and Considerations 1 TABLE OF CONTENTS The purpose of this document is to provide some basic information about the Tostan Volunteer Program and associated costs and considerations to prospective volunteers. It was created to help prospective volunteers estimate the finances, resources, and general preparations they will need to volunteer for Tostan. The information it contains is for guidance only, and it should not be considered complete, or completely accurate, for any particular individual. Please see our responsibility waiver for further information and direct all specific questions to the Volunteer Coordinator. Prices are estimates and are given in US dollars and Euros. Volunteer program overview………………………………….3 Cultural considerations……………………………………….4 Initial trip preparations ………………………………………5 Preparing to go………………………………………………..8 In-country living expenses…………………………………...12 Important Tostan contact information………………………15 Tostan Volunteer Program – Costs and Considerations 2 VOLUNTEER PROGRAM OVERVIEW TYPES OF VOLUNTEERS Tostan currently accepts 3 main types of volunteers for commitments of at least one year: Full-time University or Fellowship Volunteers: Tostan has a partnership with several university and fellowship programs that allow students to earn credit while volunteering at Tostan. We also accept applications from undergraduate students wishing to volunteer on an independent basis. If you or your university would like to make arrangements or get more information, please contact us at [email protected] for details on program structure. Full-time Volunteers: Tostan accepts highly qualified and motivated college students, graduates and career professionals into the Tostan for a minimum 12-month stay. Part-time Volunteers: In general, Tostan does not accept part-time volunteers. -

Spotlight on Our Partner Communities
Four Weeks, Four Countries, Four Public Declarations: Guinea, Mali, Senegal, and The Tostan’s Image of the Gambia Month Tostan partner communities in four countries in West Africa build momentum for the movement to abandon female genital cutting (FGC) and child/forced marriage as they publicly declare their abandonment of these practices. Read More » However Long the Night receives positive At a public declaration for reviews and press abandonment in The Gambia The new book about Tostan Founder, Molly Melching, and th Tostan's work has received positive reviews from Melinda on June 16 , Day of the African Child, community Gates on the Impatient Optimists' blog and in the Stanford members of all ages Social Innovation Review among others. In the last two celebrated the day's theme to months, Molly Melching has also made appearances in the promote the end of social US and Canada sharing the story of Tostan including media and cultural practices that are spots on PBS NewsHour and Leonard Lopate, harmful to children. Read More » Tostan Launches New Campaign: Generational Change in Three Years Over the next three years, Tostan will partner with 1,000 communities to reach more than 1.6 million people in six West African countries. This campaign presents a unique opportunity to end FGC in Senegal and expand the movement in West Africa, greatly reduce child/forced marriage and violence against women and girls, and transform education for a generation of parents and children. Read More » Spotlight on our Partner Communities Communities from Mauritania and Senegal Discuss Solutions to Gender-Based Violence Representatives from 25 Community Management Committees in Mauritania crossed the river into Senegal to participate in a cross-border meeting to discuss solutions to gender-based violence and the impacts of the Tostan program on their communities. -

Insights from Tostan
Social Norms Change at Scale: Insights from Tostan By Diane Gillespie, Gannon Gillespie, and Molly Melching The Approach Tostan, which means “breakthrough” in the Wolof language, is an international nonprofit organization founded in 1991 and headquartered in Dakar, Senegal. Tostan is currently offering its 30-month program in five West African countries. We are dedicated to empowering African communities to bring about sustainable development and positive social transformation based on respect for human rights. At Tostan, we believe that development is most effective and sustainable when brought about by communities themselves. In this community-led approach to social change, we see our role as a facilitator—to share resources, skills, and knowledge that will empower communities to set their own goals and create change on their own terms. Through a holistic, human rights-based education program, the Community Empowerment Program, we ignite community dialogue on a wide range of topics through modules focused on democracy, human rights, hygiene and health, and problem-solving. We then reinforce these topics while providing training in literacy, numeracy, and project-management skills. We currently deliver the Community Empowerment Program in five West African countries: Guinea, Guinea-Bissau, Mali, Senegal, and The Gambia. (It has also been implemented in Mauritania, Somalia, and Djibouti). Participants represent the community at large, including women and men, elders and youth, from various ethnic groups and social strata. Most have never received formal schooling or dropped out at an early age. Sessions last for two hours, three times a week. Participating communities must house and feed the facilitator and create the classroom space. -

The Tostan FGM Program in Senegal, Mali and the Sudan
Kansas State University Libraries New Prairie Press 2006 Conference Proceedings (Minneapolis, Adult Education Research Conference MN) Transformative Learning on the Desert’s Edge: The Tostan FGM Program in Senegal, Mali and the Sudan Peter Easton Kristen Molyneaux Florida State University Follow this and additional works at: https://newprairiepress.org/aerc Part of the Adult and Continuing Education Administration Commons This work is licensed under a Creative Commons Attribution-Noncommercial 4.0 License Recommended Citation Easton, Peter and Molyneaux, Kristen (2006). "Transformative Learning on the Desert’s Edge: The Tostan FGM Program in Senegal, Mali and the Sudan," Adult Education Research Conference. https://newprairiepress.org/aerc/2006/papers/19 This is brought to you for free and open access by the Conferences at New Prairie Press. It has been accepted for inclusion in Adult Education Research Conference by an authorized administrator of New Prairie Press. For more information, please contact [email protected]. Transformative Learning on the Desert’s Edge: The Tostan FGM Program in Senegal, Mali and the Sudan Peter Easton and Kristen Molyneaux Florida State University Keywords: Empowerment, transformative learning, female genital mutilation Abstract: This paper examines strategies of the Tostan Village Empowerment Program in Senegal for promoting abandonment of female genital mutilation as an example of transformative learning; and it draws lessons for the refinement of that theory. Female genital cutting (FGC) or female genital mutilation (FGM)--less accurately termed “female circumcision”--is a centuries-old cultural practice in parts of sub-Saharan Africa and in a few contiguous areas of the Muslim world, such as Egypt and Yemen. -

121 Communities in Senegal Declare Abandonment of Female Genital Cutting and Child/Forced Marriage Education Key to Protecting C
121 Communities in Senegal Declare Abandonment of Female Genital Cutting and Child/Forced Marriage On December 21st, 121 communities from the department of Ranerou in Northern Senegal came together to publicly declare their abandonment of female genital cutting and child/forced marriage! Read to learn more about the communities' journey to making such an historic decision. Education Key to Protecting Child Rights in West Africa On International Human Rights Day, the Christian Science Monitor published an inspiring piece by Mouhamed Chérif Diop--Imam and child protection specialist at Tostan--on how to protect the rights of children using education and community-led dialogue. Read the full article here. Michelle Obama Champions Tostan's Approach During a speech given at the Brookings Institution on girls' education, Michelle Obama applauded the work of Tostan, highlighting the need to work with communities, in accordance with their values. Read the coverage on Voice of America here, or you can watch the clip here (the Tostan reference specifically starts around 1:38). converted by Web2PDFConvert.com Spotlight on our Partner Communities Portrait of Mah Cissé - Orchid Project Mah Cissé, a native of Mali, spoke as the guest of honor at an international FGC conference, co-hosted by the Orchid Project and the Danish Parliament. In the presence of many dignitaries, including the Crown Princess of Denmark, Mah delivered an impassioned speech that touched the hearts of all those present. Read More » Youth Caravan from Gambia Hits the Road to Share Knowledge on Human Rights Tostan's Youth Caravan in the Gambia, including representatives from 187 communities, traveled from one community to another, sharing what they had learned about human rights during the Community Empowerment Program (CEP). -
ANNUAL REPORT Through Tostan's Community Empowerment Program and by Serving on Community Management Committees
click a tab to view From the CEO Passing the Torch From a Spark to a Fire 2017 Achievements SDGs and the Community Empowerment Program Tostan Training Center Sustaining and Renewing the Flame Your Support Financials Join the Movement Voice from the Leadership Circle Voice from the Board With Gratitude Two national councilors from the Basse region of The Gambia, featured at left, learned leadership skills 2017 ANNUAL REPORT through Tostan's Community Empowerment Program and by serving on Community Management Committees. tostan.org click a tab Letter from the CEO to view From the CEO Dear Tostan Community, I believe that what Tostan does at its very core is uncover the tremendous, often-hidden light that is present in Passing the Torch all humans — the energy to contribute to something better. In partner communities going through our education programs, that energy can quite literally illuminate an From a Spark to a Fire entirely new world, for themselves and so many whom they influence. For participants in our training programs, that energy can fuel a new way of working to make change in so many places. In our organization, hundreds of facilitators, staff, leaders, and volunteers ignite themselves everyday to make our programs possible, and this 2017 Achievements year they have strengthened our organization itself during a transitional period. This is kindled by the passion ELENA BONOMETTI and action of partners and Global Mobilizers around the world who find creative new ways to apply Tostan's SDGs and the Community model in their own lives and work. Empowerment Program As you might imagine, it has been a true joy and a deep honor for me to join Founder Molly Melching and the Tostan Training Center entire Tostan community, to both draw from this energy and contribute my own, as Tostan's CEO. -

Management of Health Complications from Female Genital Mutilation I
WHO guidelines on the management of health complications from female genital mutilation i WHO guidelines on the management of health complications from female genital mutilation WHO guidelines on the management of health complications from female genital mutilation WHO Library Cataloguing-in-Publication Data WHO guidelines on the management of health complications from female genital mutilation. I. World Health Organization. ISBN 978 92 4 154964 6 Subject headings are available from WHO institutional repository © World Health Organization 2016 All rights reserved. Publications of the World Health Organization are available on the WHO website (http:// www.who.int) or can be purchased from WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; email: [email protected]). Requests for permission to reproduce or translate WHO publications – whether for sale or for non- commercial distribution – should be addressed to WHO Press through the WHO website (http://www.who. int/about/licensing/copyright_form/index.html). The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted and dashed lines on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. -

Female Genital Cutting in the Gambia: a Case Study of Tostan by Sarah Kopper MPP Essay Submitted to Oregon State University in P
Female Genital Cutting in The Gambia: A Case Study of Tostan by Sarah Kopper MPP Essay submitted to Oregon State University in partial fulfillment of the requirements for the degree of Master of Public Policy Presented June 1, 2010 Commencement June 2010 Master of Public Policy essay of Sarah Kopper presented on June 1, 2010 APPROVED: Rebecca Warner, representing Sociology Bryan Tilt, representing Anthropology Janet Lee, representing Women’s Studies Sarah Kopper, Author ABSTRACT The World Health Organization (WHO) defines female genital cutting (FGC) as “all procedures that involve partial or total removal of the external female genitalia, or other injury to the female genital organs for non-medical reasons” (WHO, 2010). This practice has existed in Africa for thousands of years, but over the past few decades it has captured the attention of Western audiences and development organizations. One organization that has received a considerable amount of attention is Tostan, a NGO that implements a human-rights based, non-formal educational program in West and East Africa. Tostan vaulted onto the international scene in 1997 when it began facilitating the first public declaration abandoning FGC. To date, close to 5,000 communities in 5 countries have publically announced their abandonment of FGC in front of political leaders, religious leaders, and other communities in their area. This essay is a case study that explores why Tostan’s program and approach have led to FGC abandonment in The Gambian context. Using curriculum review, classroom observation, and interviews with staff and participants, I found that Tostan’s success stems from its use of a holistic, respectful approach that incorporates community values.