Pervasive Blood Pressure Monitoring Using Photoplethysmogram (PPG) Sensor
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

"Peripheral Vascular Noninvasive Measurements"
234 PERIPHERAL VASCULAR NONINVASIVE MEASUREMENTS Peripheral vascular disease includes occlusive diseases of the arteries and the veins. An example is peripheral arter- ial occlusive disease (PAOD), which is the result of a buildup of plaque on the inside of the arterial walls, inhi- biting proper blood supply to the organs. Symptoms include pain and cramping in extremities, as well as fatigue; ultimately, PAOD threatens limb vitality. The PAOD is often indicative of atherosclerosis of the heart and brain, and is therefore associated with an increased risk of myo- cardial infarction or cerebrovascular accident (stroke). Venous occlusive disease is the forming of blood clots in the veins, usually in the legs. Clots pose a risk of breaking free and traveling toward the lungs, where they can cause pulmonary embolism. In the legs, thromboses interfere with the functioning of the venous valves, causing blood pooling in the leg (postthrombotic syndrome) that leads to swelling and pain. Other causes of disturbances in peripheral perfusion include pathologies of the autoregulation of the microvas- PARENTERAL NUTRITION. See NUTRITION, culature, such as in Reynaud’s disease or as a result of PARENTERAL. diabetes. To monitor vascular function, and to diagnose and PCR. See POLYMERASE CHAIN REACTION. monitor PVD, it is important to be able to measure PERCUTANEOUS TRANSLUMINAL CORONARY and evaluate basic vascular parameters, such as arterial ANGIOPLASTY. See CORONARY ANGIOPLASTY AND and venous blood flow, arterial blood pressure, and GUIDEWIRE DIAGNOSTICS. vascular compliance. Many peripheral vascular parameters can be assessed See FETAL MONITORING. PERINATAL MONITORING. with invasive or minimally invasive procedures. Examples are the use of arterial catheters for blood pressure monitoring and the use of contrast agents in vascular PERIPHERAL VASCULAR NONINVASIVE X ray imaging for the detection of blood clots. -

Sinus Or Not
Sinus or not Citation for published version (APA): Papini, G. B., Fonseca, P., Eerikäinen, L. M., Overeem, S., Bergmans, J. W. M., & Vullings, R. (2018). Sinus or not: a new beat detection algorithm based on a pulse morphology quality index to extract normal sinus rhythm beats from wrist-worn photoplethysmography recordings. Physiological Measurement, 39(11), [115007]. https://doi.org/10.1088/1361-6579/aae7f8 DOI: 10.1088/1361-6579/aae7f8 Document status and date: Published: 26/11/2018 Document Version: Accepted manuscript including changes made at the peer-review stage Please check the document version of this publication: • A submitted manuscript is the version of the article upon submission and before peer-review. There can be important differences between the submitted version and the official published version of record. People interested in the research are advised to contact the author for the final version of the publication, or visit the DOI to the publisher's website. • The final author version and the galley proof are versions of the publication after peer review. • The final published version features the final layout of the paper including the volume, issue and page numbers. Link to publication General rights Copyright and moral rights for the publications made accessible in the public portal are retained by the authors and/or other copyright owners and it is a condition of accessing publications that users recognise and abide by the legal requirements associated with these rights. • Users may download and print one copy of any publication from the public portal for the purpose of private study or research. -
Blood Pressure Estimation Using Photoplethysmogram Signal and Its Morphological Features
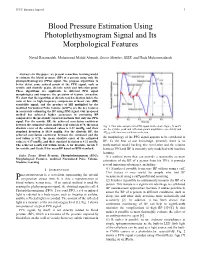
IEEE Sensors Journal 1 Blood Pressure Estimation Using Photoplethysmogram Signal and Its Morphological Features Navid Hasanzadeh, Mohammad Mahdi Ahmadi, Senior Member, IEEE, and Hoda Mohammadzade Abstract —In this paper, we present a machine learning model to estimate the blood pressure (BP) of a person using only his photoplethysmogram (PPG) signal. We propose algorithms to better detect some critical points of the PPG signal, such as systolic and diastolic peaks, dicrotic notch and inflection point. These algorithms are applicable to different PPG signal morphologies and improve the precision of feature extraction. We show that the logarithm of dicrotic notch reflection index, the ratio of low- to high-frequency components of heart rate (HR) variability signal, and the product of HR multiplied by the modified Normalized Pulse Volume (mNPV) are the key features in accurately estimating the BP using PPG signal. Our proposed method has achieved higher accuracies in estimating BP compared to the previously reported methods that only use PPG signal. For the systolic BP, the achieved correlation coefficient between the estimated values and the real values is 0.78, the mean Fig. 1. Two pulse samples of a PPG signal. In the above figure, X and Y absolute error of the estimated values is 8.22 mmHg, and their are the systolic peak and inflection points amplitudes respectively and standard deviation is 10.38 mmHg. For the diastolic BP, the ∆͎ is the time interval be tween the two . achieved correlation coefficient between the estimated and the real values is 0.72, the mean absolute error of the estimated the morphology of the PPG signal appears to be correlated to values is 4.17 mmHg, and their standard deviation is 4.22 mmHg. -

False Arrhythmia Alarm Suppression Using ECG, ABP, and Photoplethysmogram Anagha Vishwas Deshmane
False Arrhythmia Alarm Suppression Using ECG, ABP, and Photoplethysmogram by Anagha Vishwas Deshmane S.B., Massacusetts Institute of Technology (2008) Submitted to the Department of Electrical Engineering and Computer Science in partial fulfillment of the requirements for the degree of Master of Engineering in Electrical Engineering and Computer Science at the MASSACHUSETTS INSTITUTE OF TECHNOLOGY September 2009 c Massachusetts Institute of Technology 2009. All rights reserved. Author.............................................................. Department of Electrical Engineering and Computer Science August 21, 2009 Certified by. Dr. Roger G. Mark Distinguished Professor in Health Science & Technology M.I.T. Thesis Supervisor Certified by. Lauren J. Kessler Charles Stark Draper Laboratory VI-A Company Thesis Supervisor Accepted by......................................................... Dr. Christopher J. Terman Chairman, Department Committee on Graduate Theses 2 False Arrhythmia Alarm Suppression Using ECG, ABP, and Photoplethysmogram by Anagha Vishwas Deshmane Submitted to the Department of Electrical Engineering and Computer Science on August 21, 2009, in partial fulfillment of the requirements for the degree of Master of Engineering in Electrical Engineering and Computer Science Abstract A signal quality assessment scheme for the photoplethysmogram waveform recorded by a pulse oximeter has been created. The signal quality algorithm uses statistical methods on time-series and spectral analysis to locate high-frequency segments of the photoplethysmogram waveform. A photoplethysmogram pulse onset detector has been implemented for heart rate estimation. Application of the signal quality met- ric and photoplethysmogram pulse onset detector are demonstrated in an algorithm which suppresses false electrocardiogram critical arrhythmia alarms issued by bedside monitors in hospital intensive care units. M.I.T. Thesis Supervisor: Dr. Roger G. -

Sources of Inaccuracy in Photoplethysmography for Continuous Cardiovascular Monitoring
biosensors Review Sources of Inaccuracy in Photoplethysmography for Continuous Cardiovascular Monitoring Jesse Fine 1, Kimberly L. Branan 1, Andres J. Rodriguez 2, Tananant Boonya-ananta 2, Ajmal 2, Jessica C. Ramella-Roman 2,3, Michael J. McShane 1,4,5,* and Gerard L. Coté 1,5,* 1 Department of Biomedical Engineering, Texas A&M University, College Station, TX 77843, USA; jfi[email protected] (J.F.); [email protected] (K.L.B.) 2 Department of Biomedical Engineering, Florida International University, Miami, FL 33174, USA; arodr829@fiu.edu (A.J.R.); tboon007@fiu.edu (T.B.-a.); aajma003@fiu.edu (A.); jramella@fiu.edu (J.C.R.-R.) 3 Herbert Wertheim College of Medicine, Florida International University, Miami, FL 33199, USA 4 Department of Materials Science and Engineering, Texas A&M University, College Station, TX 77843, USA 5 Center for Remote Health Technologies and Systems, Texas A&M Engineering Experimentation Station, Texas A&M University, College Station, TX 77843, USA * Correspondence: [email protected] (M.J.M.); [email protected] (G.L.C.); Tel.: +1-979-845-7941 (M.J.M.); +1-979-458-6082 (G.L.C.) Abstract: Photoplethysmography (PPG) is a low-cost, noninvasive optical technique that uses change in light transmission with changes in blood volume within tissue to provide information for cardiovascular health and fitness. As remote health and wearable medical devices become more prevalent, PPG devices are being developed as part of wearable systems to monitor parameters such as heart rate (HR) that do not require complex analysis of the PPG waveform. However, complex analyses of the PPG waveform yield valuable clinical information, such as: blood pressure, respiratory information, sympathetic nervous system activity, and heart rate variability. -

Photoplethysmography-Based Continuous Systolic Blood Pressure Estimation Method for Low Processing Power Wearable Devices
applied sciences Article Photoplethysmography-Based Continuous Systolic Blood Pressure Estimation Method for Low Processing Power Wearable Devices Rolandas Gircys 1, Agnius Liutkevicius 1,* , Egidijus Kazanavicius 1, Vita Lesauskaite 2, Gyte Damuleviciene 2 and Audrone Janaviciute 1 1 Centre of Real Time Computer Systems, Kaunas University of Technology, Barsausko str. 59-A316, LT-51423 Kaunas, Lithuania; [email protected] (R.G.); [email protected] (E.K.); [email protected] (A.J.) 2 Clinical Department of Geriatrics, Lithuanian University of Health Sciences, Josvainiu str. 2, LT-47144 Kaunas, Lithuania; [email protected] (V.L.); [email protected] (G.D.) * Correspondence: [email protected] Received: 13 April 2019; Accepted: 28 May 2019; Published: 30 May 2019 Abstract: Regardless of age, it is always important to detect deviations in long-term blood pressure from normal levels. Continuous monitoring of blood pressure throughout the day is even more important for elderly people with cardiovascular diseases or a high risk of stroke. The traditional cuff-based method for blood pressure measurements is not suitable for continuous real-time applications and is very uncomfortable. To address this problem, continuous blood pressure measurement methods based on photoplethysmogram (PPG) have been developed. However, these methods use specialized high-performance hardware and sensors, which are not available for common users. This paper proposes the continuous systolic blood pressure (SBP) estimation method based on PPG pulse wave steepness for low processing power wearable devices and evaluates its suitability using the commercially available CMS50FW Pulse Oximeter. The SBP estimation is done based on the PPG pulse wave steepness (rising edge angle) because it is highly correlated with systolic blood pressure. -

The Comparison Between High Tension and Normal Tension Glaucoma
EPMA Journal (2018) 9:35–45 https://doi.org/10.1007/s13167-017-0124-4 RESEARCH Heart rate variability: the comparison between high tension and normal tension glaucoma Natalia Ivanovna Kurysheva1,2,3 & Tamara Yakovlevna Ryabova4 & Vitaliy Nikiforovich Shlapak4 Received: 4 October 2017 /Accepted: 21 December 2017 /Published online: 22 February 2018 # The Author(s) 2018. This article is an open access publication Abstract Relevance Vascular factors may be involved in the development of both high tension glaucoma (HTG) and normal tension (NTG) glaucoma; however, they may be not exactly the same. Autonomic dysfunction characterized by heart rate variability (HRV) is one of the possible reasons of decrease in mean ocular perfusion pressure (MOPP). Purpose To compare the shift of the HRV parameters in NTG and HTG patients after a cold provocation test (CPT). Methods MOPP, 24-hour blood pressure and HRV were studied in 30 NTG, 30 HTG patients, and 28 healthy subjects. The cardiovascular fitness assessment was made before and after the CPT. The direction and magnitude of the average group shifts of the HRV parameters after CPT were assessed using the method of comparing regression lines in order to reveal the difference between the groups. Results MOPP and minimum daily diastolic blood pressure were decreased in HTG and NTG patients compared to healthy subjects. There was no difference in MOPP between HTG and NTG before the CPT. However, all HRV parameters reflected the predominance of sympathetic innervation in glaucoma patients compared to healthy subjects (P <0.05). Before the CPT, the standard deviation of NN intervals (SDNN) of HRV was lower in HTG compared to NTG, 27.2 ± 4.1 ms and 35.33 ± 2.43 ms (P = 0.02), respectively. -

Photoplethysmograph 1 Photoplethysmograph
Photoplethysmograph 1 Photoplethysmograph A photoplethysmograph (PPG) is an optically obtained plethysmograph, a volumetric measurement of an organ. A PPG is often obtained by using a pulse oximeter which illuminates the skin and measures changes in light absorption (Shelley and Shelley, 2001). A conventional pulse oximeter monitors the perfusion of blood to the dermis and subcutaneous tissue of the skin. Representative PPG taken from an ear pulse oximeter. Variation in amplitude are from Respiratory Induced Variation. With each cardiac cycle the heart pumps blood to the periphery. Even though this pressure pulse is somewhat damped by the time it reaches the skin, it is enough to distend the arteries and arterioles in the subcutaneous tissue. If the pulse oximeter is attached without compressing the skin, a pressure pulse can also be seen from the venous plexus, as a small secondary peak. The change in volume caused by the pressure pulse is detected by illuminating the skin with the light from a Light Emitting Diode (LED) and then measuring the amount of light either transmitted or reflected to a photodiode. Each cardiac cycle appears as a peak, as seen in the figure. Because blood flow to the skin can be modulated by multiple other physiological systems, the PPG can also be used to monitor breathing, hypovolemia, and other circulatory conditions (Reisner, Diagram of the layers of human skin et al., 2008) [1]. Additionally, the shape of the PPG waveform differs from subject to subject, and varies with the location and manner in which the pulse oximeter is attached. Sites for measuring PPG While pulse oximeters are a commonly used medical device the PPG derived from them is rarely displayed, and is nominally only processed to determine heart rate. -
Thesis Submitted to the University of Nottingham for the Degree of Doctor
/. NýVERsýýý ýN`? ,ý ý+`" ý ý+ ýTING off;..:ý,,.. ýý,ý "The Wavelength Dependence of the Photoplethysmogram and its Implication to Pulse Oximetry" by Damianos Damianou, MSc Thesis submitted to the University of Nottingham for the degree of Doctor of Philosophy, October, 1995 ABSTRACT Since the early 1980s the increase in use of pulse oximeters in many clinical situations has been quite remarkable, turning it into one of the most important methods of monitoring in use today. Pulse oximetry essentially uses photoplethysmography to calculate oxygen saturation. Consequently the wavelength dependence of the photoplethysmogram (PPG) is of direct relevance in the performance of pulse oximeters. The experimental results obtained on the wavelength dependence of the AC, DC AC/DC PPG and components for the 450 - 1000nm range are undoubtedly different to the ones predicted by the current simple pulse oximeter model based on the Lambert-Beer law. Moreover, they show unexpected phenomena regarding the magnitude of the above components over the whole range, with distinct differences between the reflection and transmission modes. This is of significance to the technique of pulse oximetry suggesting that perhaps other wavelengths should be considered for use, and that use of both "reflection" and "transmission" probes on the same oximeter may lead to inaccurate readings in one of the modes. A finger model was developed and results from Monte Carlo simulations of photon propagation obtained. The results did not correspond to the experimental results, this is most probably due to either wrong parameters or model. Recent advances in the use of reflection pulse oximeters on fetal monitoring during labour, have raised the question of possible artifacts which may arise due to inadequate probe application in the birth canal. -

Noninvasive Hemoglobin Level Prediction in a Mobile Phone Environment: State of the Art Review and Recommendations
JMIR MHEALTH AND UHEALTH Hasan et al Original Paper Noninvasive Hemoglobin Level Prediction in a Mobile Phone Environment: State of the Art Review and Recommendations Md Kamrul Hasan1, PhD; Md Hasanul Aziz2, BSc; Md Ishrak Islam Zarif2, BSc; Mahmudul Hasan3, BSc; MMA Hashem4, PhD; Shion Guha2, PhD; Richard R Love2, MD; Sheikh Ahamed2, PhD 1Department of Electrical Engineering and Computer Science, Vanderbilt University, Nashville, TN, United States 2Department of Computer Science, Marquette University, Milwaukee, WI, United States 3Department of Computer Science, Stony Brook University, Stony Brook, NY, United States 4Department of Computer Science & Engineering, Khulna University of Engineering & Technology, Khulna, Bangladesh Corresponding Author: Md Kamrul Hasan, PhD Department of Electrical Engineering and Computer Science Vanderbilt University 334 Featheringill Hall Nashville, TN United States Phone: 1 6153435032 Email: [email protected] Abstract Background: There is worldwide demand for an affordable hemoglobin measurement solution, which is a particularly urgent need in developing countries. The smartphone, which is the most penetrated device in both rich and resource-constrained areas, would be a suitable choice to build this solution. Consideration of a smartphone-based hemoglobin measurement tool is compelling because of the possibilities for an affordable, portable, and reliable point-of-care tool by leveraging the camera capacity, computing power, and lighting sources of the smartphone. However, several smartphone-based hemoglobin measurement techniques have encountered significant challenges with respect to data collection methods, sensor selection, signal analysis processes, and machine-learning algorithms. Therefore, a comprehensive analysis of invasive, minimally invasive, and noninvasive methods is required to recommend a hemoglobin measurement process using a smartphone device. -
Fuzzy Logic Hemoglobin Sensors
Fuzzy Logic Hemoglobin Sensors Zur Erlangung des akademischen Grades eines DOKTOR-INGENIEURS von M. Sc. Eng. Kawther Abo Alam Fuzzy Logic Hemoglobin Sensors Zur Erlangung des akademischen Grades eines DOKTOR-INGENIEURS von der Fakultät für Elektrotechnik und Informationstechnik des Karlsruher Instituts für Technologie (KIT) vorgelegte DISSERTATION von M. Sc. Eng. Kawther Abo Alam Geb. in: El-Minoufia, Ägypten. Tag der mündlichen Prüfung: 10.05.2011 Hauptreferent: Prof. Dr. rer. nat. Armin Bolz Korreferent: Prof. Dr. rer. nat. Josef Guttmann INSTITUT FÜR BIOMEDIZINISCHE TECHNIK KARLSRUHER INSTITUT FÜR TECHNOLOGIE (KIT) n 1 List of Contents: Introduction ............................................................................................................... 14 1.1 Motivation ..................................................................................................................... 14 1.2 Research objectives ........................................................................................................ 16 1.2.1 Non-invasive measuring ................................................................................... 16 1.2.2 Invasive measuring .......................................................................................... 16 1.3 Thesis outline ................................................................................................................. 17 Part I: Background and Current State of the Art .................................................... 18 Physiological Foundations ........................................................................................ -

Photoplethysmography in Normal and Pathological Sleep
sensors Perspective Photoplethysmography in Normal and Pathological Sleep Ramona S. Vulcan 1, Stephanie André 1 and Marie Bruyneel 1,2,* 1 Department of Pulmonary Medicine, CHU Brugmann, Université Libre de Bruxelles (ULB), 1020 Brussels, Belgium; [email protected] (R.S.V.); [email protected] (S.A.) 2 Department of Pulmonary Medicine, CHU Saint-Pierre, Université Libre de Bruxelles (ULB), 1000 Brussels, Belgium * Correspondence: [email protected]; Tel.: +322-5354219; Fax: +322-5353362 Abstract: This article presents an overview of the advancements that have been made in the use of photoplethysmography (PPG) for unobtrusive sleep studies. PPG is included in the quickly evolving and very popular landscape of wearables but has specific interesting properties, particularly the ability to capture the modulation of the autonomic nervous system during sleep. Recent advances have been made in PPG signal acquisition and processing, including coupling it with accelerometry in order to construct hypnograms in normal and pathologic sleep and also to detect sleep-disordered breathing (SDB). The limitations of PPG (e.g., oxymetry signal failure, motion artefacts, signal processing) are reviewed as well as technical solutions to overcome these issues. The potential medical applications of PPG are numerous, including home-based detection of SDB (for triage purposes), and long-term monitoring of insomnia, circadian rhythm sleep disorders (to assess treatment effects), and treated SDB (to ensure disease control). New contact sensor combinations to improve future wearables seem promising, particularly tools that allow for the assessment of brain activity. In this way, in-ear EEG combined with PPG and actigraphy could be an interesting focus for future research.