FY 2016 ICD-10-CM Official Guidelines for Coding and Reporting
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Information for Referrers: Chronic Urticaria
Fact Sheet Information for Referrers: Chronic Urticaria Chronic urticaria (CU) is defined by the presence of urticaria (wheals, hives) on most days of the week, for longer than six weeks. Angioedema occurs in about 40 percent of patients with CU and usually affects the lips, cheeks, periorbital areas, extremities, and genitals (seldom the tongue, throat or airway). In many cases, the underlying cause is autoimmunity (autoantibodies to the mast cell IgE receptor). Food allergy is almost never the cause. Chronic urticaria can cause marked distress because it is physically uncomfortable, waxes and wanes unpredictably, and may interfere with work/school and sleep. When to refer CU patients: > Where CU is not controlled by antihistamines or has persisted for more than 6 months. > Where there is concern patients are undertaking inappropriate dietary restrictions. > Where angioedema has involved the oropharyngeal or laryngeal areas. > Any features that might suggest an autoimmune or inflammatory disorder. > Where there are features to suggest urticarial vasculitis (lesions lasting >24 hours, burning rather than itching, residual bruising). > Where prednisolone has been needed repeatedly to control symptoms. Reassurance Patients with CU are often frustrated, and reassurance is an important component of successful management. There are three important concepts to relay to patients: > CU is usually transient, and 50 percent of patients undergo remission within one year. > While acute urticaria may be a manifestation of allergy and may be associated with anaphylaxis, chronic urticaria is a different disorder that is usually not allergic in origin and is not dangerous. > The symptoms of CU can be successfully managed in the majority of patients. -

The Health and Welfare of Australia's Aboriginal and Torres Strait Islander People: an Overview (Full Publication; 5 May
The health and welfare of Australia’s Aboriginal and Torres Strait Islander people an overview 2011 The Australian Institute of Health and Welfare is Australia’s national health and welfare statistics and information agency. The Institute’s mission is better information and statistics for better health and wellbeing. © Australian Institute of Health and Welfare 2011 This work is copyright. Apart from any use as permitted under the Copyright Act 1968, no part may be reproduced without prior written permission from the Australian Institute of Health and Welfare. Requests and enquiries concerning reproduction and rights should be directed to the Head of the Communications, Media and Marketing Unit, Australian Institute of Health and Welfare, GPO Box 570, Canberra ACT 2601. A complete list of the Institute’s publications is available from the Institute’s website <www.aihw.gov.au>. ISBN 978 1 74249 148 6 Suggested citation Australian Institute of Health and Welfare 2011. The health and welfare of Australia’s Aboriginal and Torres Strait Islander people, an overview 2011. Cat. no. IHW 42. Canberra: AIHW. Australian Institute of Health and Welfare Board Chair Hon. Peter Collins, AM, QC Director David Kalisch Any enquiries about or comments on this publication should be directed to: Communication, Media and Marketing Unit Australian Institute of Health and Welfare GPO Box 570 Canberra ACT 2601 Phone: (02) 6244 1032 Email: [email protected] Published by the Australian Institute of Health and Welfare Printed by Paragon Printers Australasia Please note that there is the potential for minor revisions of data in this report. Please check the online version at <www.aihw.gov.au> for any amendments. -

Consensus Recommendations for National and State Poisoning Surveillance
Consensus Recommendations for National and State Poisoning Surveillance REPORT FROM THE INJURY SURVEILLANCE WORKGROUP (ISW7) April 2012 Table of Contents FOREWORD 3 EXECUTIVE SUMMARY 4 Key products of the ISW7 include: 4 INTRODUCTION 6 Public Health Burden of Poisoning 7 CONCEPTUAL DEFINITIONS OF POISONING AND DRUG 9 Poisoning 9 Drug 10 OPERATIONAL DEFINITIONS OF POISONING AND DRUG POISONING 12 Description of the Poisoning Matrix for ICD-9-CM Coded Morbidity Data 12 Description of Poisoning Matrix for ICD-10 Coded Mortality Data 15 Operational Definitions for Other Major Data Sources 18 INVENTORY OF POISONING DATA SOURCES 20 GENERAL CONSIDERATIONS AND RECOMMENDATIONS FOR IMPROVING POISONING SURVEILLANCE 21 General considerations 21 Recommendations for proposed drug poisoning indicators for surveillance for state and local jurisdictions 21 Considerations for further sub-categorizations of indicators 24 RECOMMENDATIONS TO IMPROVE SURVEILLANCE AT THE STATE OR LOCAL LEVEL 25 Mortality surveillance 25 Morbidity surveillance 25 RECOMMENDATIONS TO IMPROVE SURVEILLANCE AT THE NATIONAL LEVEL 27 REFERENCES 29 APPENDICES 31 Appendix A: Detailed Description of Data Sources 32 Appendix B1: Poisoning Matrix for ICD-10 Coded Mortality Data 94 Appendix B2: SAS Programs for Poisoning Matrix for ICD-10 Coded Mortality Data 99 Appendix C1: Poisoning Matrix for ICD-9-CM Coded Morbidity Data 101 Appendix C2: SAS Programs for Poisoning Matrix for ICD-9-CM Coded Morbidity Data 106 Appendix D: List of ISW7 Workgroup Members 107 Consensus Recommendations for National and State Poisoning Surveillance 1 Methodology for this report: The Injury Surveillance Workgroup 7 worked from July 2009 through April 2012 using monthly conference calls, and more frequently through small subgroup calls, to develop this report. -

ICD-10 International Statistical Classification of Diseases and Related Health Problems
ICD-10 International Statistical Classification of Diseases and Related Health Problems 10th Revision Volume 2 Instruction manual 2010 Edition WHO Library Cataloguing-in-Publication Data International statistical classification of diseases and related health problems. - 10th revision, edition 2010. 3 v. Contents: v. 1. Tabular list – v. 2. Instruction manual – v. 3. Alphabetical index. 1.Diseases - classification. 2.Classification. 3.Manuals. I.World Health Organization. II.ICD-10. ISBN 978 92 4 154834 2 (NLM classification: WB 15) © World Health Organization 2011 All rights reserved. Publications of the World Health Organization are available on the WHO web site (www.who.int) or can be purchased from WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; e-mail: [email protected]). Requests for permission to reproduce or translate WHO publications – whether for sale or for noncommercial distribution – should be addressed to WHO Press through the WHO web site (http://www.who.int/about/licensing/copyright_form). The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. -

Urticaria and Angioedema
URTICARIA AND ANGIOEDEMA What are the aims of this leaflet? This leaflet has been written to help you understand more about urticaria and angioedema. It tells you what they are, what causes them, what you can do about them, and where you can find out more about them. What is urticaria and angioedema? Urticaria is common, and affects about 20% of people at some point in their lives. It is also known as hives or nettle rash. The short-lived swellings of urticaria are known as weals (see below) and typically any individual spot will clear within 24 hours although the overall rash may last for longer. Angioedema is a form of urticaria in which there is deeper swelling in the skin, and the swelling may take longer than 24 hours to clear. An affected individual may have urticaria alone, angioedema alone, or both together. Both are caused by the release of histamine from cells in the skin called mast cells. When angioedema occurs in association with urticaria, the two conditions can be considered part of the same process. When angioedema occurs on its own, different causes need to be considered. There are different types of urticaria of which the most common form is called ‘ordinary or idiopathic urticaria’. In this type no cause is usually identified and often patients have hives and angioedema occurring together. Ordinary urticaria with or without angioedema is usually divided into ‘acute’ and ‘chronic’ forms. In ‘acute’ urticaria/angioedema, the episode lasts from a few days up to six weeks. Chronic urticaria, by definition, lasts for more than six weeks. -

Drowning in Finland: “External Cause” and “Injury” Codes P Lunetta, a Penttilä, a Sajantila
342 Inj Prev: first published as 10.1136/ip.8.4.342 on 1 December 2002. Downloaded from METHODOLOGIC ISSUES Drowning in Finland: “external cause” and “injury” codes P Lunetta, A Penttilä, A Sajantila ............................................................................................................................. Injury Prevention 2002;8:342–344 Background: The International Classification of Diseases (ICD) external codes (E codes) for drowning assist in determining the primary event leading to drowning, but do not alone allow the precise deter- mination of the overall drowning rates. Aims: To analyze the sensitivity of the ICD E codes for drowning. To describe the pattern and trend of drowning deaths that are classified with E codes other than for drowning. Setting: Finland, 1969–2000. Methods: Mortality files of Statistics Finland were searched electronically using the injury codes (I codes) and E codes for drowning. Cross analysis of I and E coded drownings was performed to See end of article for determine the rate and pattern of drowning cases classified with E codes other than for drowning. Time authors’ affiliations trends were calculated using the Poisson regression model. ....................... Results: Of 13 705 drowning deaths, 644 (4.7%) were not identified with the E codes for drowning. Correspondence to: The great majority (n=547, 84.9%) of these cases were traffic accidents resulting in drowning. No sig- Dr Philippe Lunetta, nificant time trends were found even after the introduction, in 1996, of the ICD 10th revision. PL 40 Kytösuontie 11, 00300 Helsinki, Finland; Conclusions: In Finland, underestimation of overall drowning rates using the E code alone is less pro- [email protected] nounced than in countries where similar studies have been performed. -

Diagnostic Coding of Physical Abuse Among Patients Evaluated by a Multidisciplinary Child Protection Team in a Pediatric Level I Trauma Center
The Texas Medical Center Library DigitalCommons@TMC UT School of Public Health Dissertations (Open Access) School of Public Health Spring 5-2019 DIAGNOSTIC CODING OF PHYSICAL ABUSE AMONG PATIENTS EVALUATED BY A MULTIDISCIPLINARY CHILD PROTECTION TEAM IN A PEDIATRIC LEVEL I TRAUMA CENTER HOLLY HUGHES GARZA UTHealth School of Public Health Follow this and additional works at: https://digitalcommons.library.tmc.edu/uthsph_dissertsopen Part of the Community Psychology Commons, Health Psychology Commons, and the Public Health Commons Recommended Citation GARZA, HOLLY HUGHES, "DIAGNOSTIC CODING OF PHYSICAL ABUSE AMONG PATIENTS EVALUATED BY A MULTIDISCIPLINARY CHILD PROTECTION TEAM IN A PEDIATRIC LEVEL I TRAUMA CENTER" (2019). UT School of Public Health Dissertations (Open Access). 55. https://digitalcommons.library.tmc.edu/uthsph_dissertsopen/55 This is brought to you for free and open access by the School of Public Health at DigitalCommons@TMC. It has been accepted for inclusion in UT School of Public Health Dissertations (Open Access) by an authorized administrator of DigitalCommons@TMC. For more information, please contact [email protected]. DIAGNOSTIC CODING OF PHYSICAL ABUSE AMONG PATIENTS EVALUATED BY A MULTIDISCIPLINARY CHILD PROTECTION TEAM IN A PEDIATRIC LEVEL I TRAUMA CENTER by HOLLY HUGHES GARZA, BS, DVM APPROVED: ADRIANA PÉREZ, MS, PHD KARLA LAWSON, MPH, PHD Copyright by Holly Hughes Garza, BS, DVM, MPH 2019 DIAGNOSTIC CODING OF PHYSICAL ABUSE AMONG PATIENTS EVALUATED BY A MULTIDISCIPLINARY CHILD PROTECTION TEAM IN A PEDIATRIC LEVEL I TRAUMA CENTER by HOLLY HUGHES GARZA BS, University of Texas at Austin, 2000 DVM, North Carolina State University, 2004 Presented to the Faculty of The University of Texas School of Public Health in Partial Fulfillment of the Requirements for the Degree of MASTER OF PUBLIC HEALTH THE UNIVERSITY OF TEXAS SCHOOL OF PUBLIC HEALTH Houston, Texas May 2019 ACKNOWLEDGEMENTS Thanks to Dr. -
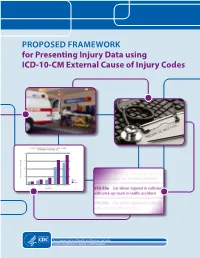
For Presenting Injury Data Using ICD-10-CM External Cause of Injury Codes
PROPOSED FRAMEWORK for Presenting Injury Data using ICD-10-CM External Cause of Injury Codes NONFATAL UNINTENTIONAL MOTOR VEHICLE-TRAFFIC OCCUPANT INJURY RATES, UNITED STATES, 2012 2000 1500 1000 500 RATE PER 100,000 POPULATION RATE MALE FEMALE 0 00–04 yrs 05–09 yrs 10–14 yrs 15–19 yrs 20–24 yrs AGE GROUP U.S. Department of Health and Human Services Centers for Disease Control and Prevention Proposed Framework for Presenting Injury Data using ICD-10-CM External Cause of Injury Codes Joseph L Annest, PhD, MS,1 Holly Hedegaard, MD, MSPH,2 Li-Hui Chen, PhD,2 Margaret Warner, PhD,2 Equater (Ann) Smalls1 March 2014 A Collaboration of CDC’s National Center for Injury Prevention and Control,1 Atlanta, GA and National Center for Health Statistics,2 Hyattsville, MD Proposed Framework for Presenting Injury Data using ICD-10-CM External Cause of Injury Codes is a publication of The National Center for Injury Prevention and Control and the National Center for Health Statistics within the Centers for Disease Control and Prevention. Centers for Disease Control and Prevention Thomas R. Frieden, MD, MPH, Director National Center for Injury Prevention and Control Daniel M. Sosin, MD, MPH, FACP, Acting Director National Center for Health Statistics Charles J. Rothwell, MBA, MS, Director Suggested citation: Annest, J., Hedegaard, H., Chen, L., Warner, M., and Small, E. (2014). Proposed Framework for Presenting Injury Data using ICD-10-CM External Cause of Injury Codes. Atlanta, GA: National Center for Injury Prevention and Control, National Center for Health Statistics, Centers for Disease Control and Prevention. -
International Statistical Classification of Diseases and Related Health Problems (ICD-10) in Occupational Health Protection of T
World Health Organization WHO/SDE/OEH/99.11 English only Sustainable Development and Distr.: Limited Healthy Environments International Statistical Classification of Diseases and Related Health Problems (ICD-10) in Occupational Health Protection of the Human Environment Occupational and Environmental Health Series Geneva, 1999 INTERNATIONAL STATISTICAL CLASSIFICATION OF DISEASES AND RELATED HEALTH PROBLEMS (ICD-10) IN OCCUPATIONAL HEALTH Antti Karjalainen Finnish Institute of Occupational Health World Health Organization Geneva 1999 WORLD HEALTH ORGANIZATION ¾ WHO/SDE/OEH/99.11 ¾ page i INTERNATIONAL STATISTICAL CLASSIFICATION OF DISEASES AND RELATED HEALTH PROBLEMS (ICD-10) Preface Classifications of occupational diseases have been developed mainly for two purposes: (1) notification for labour safety and health surveillance and (2) compensation. The absence of unified diagnostic criteria, coding systems and classifications reduce the compatibility and comparability of national statistics on occupational diseases. The main purpose of this document is to serve as a guideline for the use of ICD-10 in notification of occupational diseases in countries which do not have a well-established notification system. The document contains general guidelines for the use of ICD-10 codes and a comprehensive list of ICD-10 codes which are relevant for notification of occupational diseases. The list enables one to select, for each country, a selection of occupational disease entities that are the most relevant when building a notification system for that country. The document also provides typical examples of the causative agents/risk factors and risk industries/occupations for each occupational disease. It is to be underlined that these lists are meant to be only examples and should not be taken as exhaustive. -

Implementing the External Cause Matrix for Injury Morbidity – North Carolina Emergency Department Data – January 2015 – May 2015/January 2016 – May 2016
IMPLEMENTING THE EXTERNAL CAUSE MATRIX FOR INJURY MORBIDITY – NORTH CAROLINA EMERGENCY DEPARTMENT DATA – JANUARY 2015 – MAY 2015/JANUARY 2016 – MAY 2016 A Report on the Transition to ICD-10-CM Prepared by Katherine Harmon1,2, MPH Clifton Barnett Barnett1, MSIS Stephen Marshall1Marshall2, PhD Anna Waller1,2, ScD Submitted July 27, 2016 1Carolina Center for Health Informatics, University of North Carolina at Chapel Hill 2Injury Prevention Research Center, University of North Carolina at Chapel Hill © 2016 University of North Carolina at Chapel Hill and NC Division of Public Health Data Attribution and Disclaimer: NC DHHS/DPH NC DETECT ED visit data were made available for this document by the NC DETECT Data Oversight Committee. The NC DETECT Data Oversight Committee and NC DETECT do not take responsibility for scientific validity or accuracy of the methodology, statistical analysis, results, or conclusions presented. Page 1 of 19 TABLE OF CONTENTS INTRODUCTION ............................................................................................................................................... 3 METHODS AND RESULTS ............................................................................................................................... 4 DISCUSSION .................................................................................................................................................. 17 CONCLUSIONS ............................................................................................................................................. -
Hospitalised Interpersonal Violence and Perpetrator Coding, Australia 2002–05
Hospitalised interpersonal violence and perpetrator coding, Australia 2002–05 Sophie Pointer and Renate Kreisfeld INJURY RESEARCH AND StatiSTICS SERIES NO. 77 INJURY RESEARCH AND STATISTICS SERIES Number 77 Hospitalised interpersonal violence and perpetrator coding, Australia 2002–05 Sophie Pointer and Renate Kreisfeld Australian Institute of Health and Welfare Canberra Cat. no. INJCAT 153 The Australian Institute of Health and Welfare is a major national agency which provides reliable, regular and relevant information and statistics on Australia’s health and welfare. The Institute’s mission is authoritative information and statistics to promote better health and wellbeing. © Australian Institute of Health and Welfare 2012 This product, excluding the AIHW logo, Commonwealth Coat of Arms and any material owned by a third party or protected by a trademark, has been released under a Creative Commons BY 3.0 (CC-BY 3.0) licence. Excluded material owned by third parties may include, for example, design and layout, images obtained under licence from third parties and signatures. We have made all reasonable efforts to identify and label material owned by third parties. You may distribute, remix and build upon this work. However, you must attribute the AIHW as the copyright holder of the work in compliance with our attribution policy available at <www.aihw.gov.au/copyright/>. The full terms and conditions of this licence are available at <http://creativecommons.org/licenses/by/3.0/au/>. Enquiries relating to copyright should be addressed to the Head of the Communications, Media and Marketing Unit, Australian Institute of Health and Welfare, GPO Box 570, Canberra ACT 2601. -

Underlying and Multiple Cause of Death Codes
Underlying and Multiple Cause of Death Codes This report contains information about the underlying cause of death variables included in the 2015 Restricted- Use Linked Mortality File (LMF). There are six underlying cause of death variables. Three variables are derived from the ICD-9 coding scheme (UCOD 282, UCOD 72, and UCOD 34); two are from the ICD-10 (UCOD 358 and UCOD 39); and one variable codes deaths from both the ICD-9 and ICD-10 into a single variable (UCOD 113). Please refer to the Public Use Data File Documentation website (https://www.cdc.gov/nchs/nvss/ mortality_public_use_data.htm) of the National Vital Statistics System (NVSS) for more detailed information on the ICD-9 and ICD-10 coding schemes. Contents 1 ICD-10 Underlying Cause of Death for Death Years 1979-2015 2 2 ICD-9: Underlying Cause of Death for Death Years 1979-1998 3 3 ICD-10: Underlying Cause of Death for Death Years 1999-2015 4 4 Multiple Cause of Death Codes 5 4.1 NCHS Procedures Used to Code Multiple Cause Data ..................... 5 4.2 Entity Axis Multiple Cause of Death Codes: COND 1-COND 20 ................ 6 4.3 Record Axis Multiple Cause of Death Codes: RCOND 1-RCOND 20 ............... 7 5 Underlying Cause of Death Tables 8 5.1 113 Causes of Death, 10th Revision: Underlying Cause of Death Recode Adapted for Use by DVS, Deaths 1979-2015 ..................................... 9 5.2 282 Causes of Death, 9th Revision: Underlying Cause of Death Recode Adapted for Use by DVS, Deaths 1979-1998 ........................................ 13 5.3 72 Causes of Death, 9th Revision: Underlying Cause of Death Recode Adapted for Use by DVS, Deaths 1979-1998 .......................................