Aviation Short Investigation Bulletin
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Nhulunbuy Corporation ABN: 57 009 596 598
PO Box 345 Nhulunbuy NT 0881 Australia Telephone: (08) 8939 2200 Facsimile: (08) 8987 2451 Email: [email protected] nhulunbuy corporation ABN: 57 009 596 598 8 February 2018 Dr Jane Thompson Committee Secretary Senate Standing Committees on Rural and Regional Affairs and Transport PO Box 6100 Parliament House Canberra ACT 2600 Dear Dr Thomson, RE: The operation, regulation and funding of air routes service delivery to rural, regional and remote communities The Nhulunbuy Corporation Limited would like to thank the Senate Committee for the opportunity to provide a submission to the above-mentioned inquiry. The township of Nhulunbuy has a population of around 3,200 and is situated in East Arnhem Land on the north western tip of the Gulf of Carpentaria 600 kilometres due east of Darwin. It is considered a vital lifeline to the outer regions with respect to the provision of shopping, hospital and health care services. Each year during the monsoonal season road access between communities within the region are not accessible by road and residents of these communities become dependent on air travel to access their basic needs. Gove Airport is located 15 kilometres from Nhulunbuy and services the communities of Nhulunbuy, Yirrkala, Gunyangara and some 80 other communities within East Arnhem Land. It also provides residents and visitors of East Arnhem Land a link with interstate and international travel through the gateway airports of Cairns International and Darwin International. It is operated by the Nhulunbuy Corporation Limited under a Deed of Agreement with Rio Tinto Alcan. Because of its strategic position, Gove Airport is a nominated alternate aerodrome for certain domestic and international carriers when access to their planned destination airport is inaccessible due to inclement weather or technical issues. -

(Iii) Airport Runway Extension Feasibility Study Update
Board Meeting: May 2018 Agenda Number: 12 (iii) Record No: ED18/3501 LORD HOWE ISLAND BOARD Business Paper OPEN SESSION ITEM Airport Runway Extension Feasibility Study Update RECOMMENDATION It is recommended that the Board note this report and endorse further investigation of the ‘570m runway extension’ option to the NW. BACKGROUND Lord Howe Island’s restricted runway length of 888 metres limits the type of commercial aircrafts that can operate on the Island. While other options have been considered such as leasing or hiring other aircrafts to operate on Lord Howe Island or to get other airlines to operate; without extending the runway, airlines will be restricted in the types of aircrafts that can service the Island. A sustainable and viable long-term solution is therefore needed to secure the provision of air services to Lord Howe Island. In late November 2017, AECOM Australia Pty Ltd was contracted to undertake the Lord Howe Island Airport Runway Extension Feasibility. The scope of the study includes the future aircraft requirements for the island, plane characteristics, existing runway/site limitations, CASA requirements, conceptual design, geotechnical investigation, environmental assessment, community consultation and economic impacts/costs. The project is broken down into a number of milestones. Milestone Description Anticipated time Completion of detailed assessment of extended runway and 1. March 2018 suitable aircraft options 2. Completion of preliminary geotechnical investigation June 2018 3. Completion of conceptual engineering design August 2018 4. Completion of preliminary environmental assessment September 2018 5. Undertake economical assessment and preliminary business case October 2018 6. Final presentation and report December 2018 The funding for the project comes predominately from a Restart NSW grant through Infrastructure NSW with a small amount of Board staff wages for project management as shown below: 1. -

Annual Report 19
Darwin Alice Springs Tennant Creek A Airport Development Group International Airport Airport Airport Annual Report 19 . Highlights 2018–19 We reached a milestone The National Critical Care In October 2018, Alice Springs of 21 years since the three and Trauma Response Centre received the first of four airports were privatised was completed at Darwin charter flights from Tokyo, under the NT Airports International Airport in Nagoya and Osaka, Japan, in banner, celebrating with April 2019, creating a world- more than 10 years. a special airside premiere class, on-airport Emergency screening of the aviation Medical Retrieval Precinct. history film ‘The Sweet Little Note of the Engine.’ Virgin Australia launched a new three-times-weekly We refurbished an seasonal service to Denpasar, underused part of the Bali, in April 2019. Sustainability reporting Darwin terminal into the introduced. Emissions target ‘Green Room’, a pop-up developed and on track to community arts space, have zero net emissions by launching it in August 2018. SilkAir announced an 2030 (scope 1 and 2). increase in weekly services between Darwin and Singapore from July 2019, Ian Kew, CEO, continued marking its seventh year of Runway overlay works as Chairman of the Darwin operations to Darwin with a commenced in Alice Springs Major Business Group and seventh weekly service. at a value of circa Chairman of the Darwin $20 million. Festival. ADG staff and the company contributed $18,000 to two ‘Happy or Not’ instant community causes from our $1.4 million infrastructure customer feedback Workplace Giving initiative. boost at Tennant Creek platforms installed in Alice for improved fencing and Springs and Darwin. -

COVID-19 UPDATE – 21St January 2021
COVID-19 UPDATE – 21st January 2021 MANDATORY FACE MASKS REQUIRED AT GOVE AIRPORT On Friday 8th January 2021, the Prime Minister announced (National Cabinet agreed) mandatory use of masks in domestic airports and on all domestic commercial flights. Furthermore, the NT Chief Health Officer Directions make it mandatory from the 20th January 2021 for face masks to be worn at all major NT airports and while on board an aircraft. Masks must be worn when inside the airport terminal building and when on the airfield. Children under the age of 12 and people with a specified medical condition are not required to wear a mask. Mask wearing is mandatory at the following Northern Territory airports: • Darwin International Airport • Alice Springs Airport • Connellan Airport - Ayers Rock (Yulara) • Gove Airport • Groote Eylandt A person is not required to wear a mask during an emergency or while doing any of the following: • Consuming food or beverage • Communicating with a person who is hearing impaired. • Wearing an oxygen mask AIRPORT & TRAVELLING • PLEASE NOTE: To reduce the challenges with social distancing and to minimise risks, only Airline passengers will be able to enter the Airport terminal, • please drop-off and pick-up passengers outside of the terminal building It is the responsibility of individuals to make sure they have a mask to wear when at major NT airports and while on board an aircraft. Additional Information: • Please be aware of the NT Government Border Controls, which may be in place https://coronavirus.nt.gov.au/travel/interstate-arrivals • https://www.interstatequarantine.org.au/state-and-territory-border-closures/ • AirNorth schedule - https://www.airnorth.com.au/flying-with-us/before-you-fly/arrivals- and-departures • https://www.cairnsairport.com.au/travelling/airport-guide/covid19/ . -
Document Title
COVID-19 Management Plan COVID-19 Management Plan Table of Contents 1 Distribution List ........................................................................................................................................ 4 1.1 Copies ............................................................................................................................................. 4 2 Amendment Record ................................................................................................................................. 4 3 Purpose .................................................................................................................................................... 4 3.1 Scope .............................................................................................................................................. 4 3.2 Documentation ................................................................................................................................ 4 4 Approvals ................................................................................................................................................. 5 5 Introduction .............................................................................................................................................. 5 5.1 Spread ............................................................................................................................................. 5 5.2 Symptoms ...................................................................................................................................... -

Northern Territory June 2012 Monthly Weather Review Northern Territory June 2012
Monthly Weather Review Northern Territory June 2012 Monthly Weather Review Northern Territory June 2012 The Monthly Weather Review - Northern Territory is produced twelve times each year by the Australian Bureau of Meteorology's Northern Territory Climate Services Centre. It is intended to provide a concise but informative overview of the temperatures, rainfall and significant weather events in Northern Territory for the month. To keep the Monthly Weather Review as timely as possible, much of the information is based on electronic reports. Although every effort is made to ensure the accuracy of these reports, the results can be considered only preliminary until complete quality control procedures have been carried out. Major discrepancies will be noted in later issues. We are keen to ensure that the Monthly Weather Review is appropriate to the needs of its readers. If you have any comments or suggestions, please do not hesitate to contact us: By mail Northern Territory Climate Services Centre Bureau of Meteorology PO Box 40050 Casuarina NT 0811 AUSTRALIA By telephone (08) 8920 3813 By email [email protected] You may also wish to visit the Bureau's home page, http://www.bom.gov.au. Units of measurement Except where noted, temperature is given in degrees Celsius (°C), rainfall in millimetres (mm), and wind speed in kilometres per hour (km/h). Observation times and periods Each station in Northern Territory makes its main observation for the day at 9 am local time. At this time, the precipitation over the past 24 hours is determined, and maximum and minimum thermometers are also read and reset. -

Company Profile
Commercial & Industrial Electrical & Mechanical Contracting, Fibre Optics, Communications, Data, Security, MATV, CCTV, Fire, Control Systems, Lightning Protection Systems High Voltage reticulation, Transformers Accredited PowerWater Contractor ABN 20 062 315 137 Company Profile Kellyco Electrical Services Pty Ltd was established in 1993 in Alice Springs. The company has enjoyed successful growth and expansion over the last 25 years, which has enabled us to establish an enviable reputation for professionalism and reliability. Our Darwin operation was opened in September 2008 and in 2012 we became an accredited member of Master Electricians. Kellyco initially specialised in remote area commercial and industrial projects. In 2001 we diversified and expanded completing more complex commercial projects in Alice Springs and Darwin. Over the last 25 years we have developed a sound infrastructure including over 20 registered vehicles and plant equipment, we hold Electrical Contracting Licences for Northern Territory and South Australia. Please find our NT Contractors Accreditation to give you an idea our Certificate Levels. Kellyco can offer a complete installation package for Commercial , High Rise, Large Residential Projects and Industrial Electrical Installations, Data (20 year Madison certified), Fibre Optic Cabling, Data and Communications, MATV, CCTV, Security, Fire, PA Systems, Lightning Protection, Control Systems, High Voltage Reticulation, Transformers, Low Voltage reticulation. We also manage our own Design and Construct packages all to AS/NZ standards. Federal Safety System Kellyco are accredited members of the Master Electricians Association which includes the Federally recognised Safety Connect Electrical Safety Management System. Our SafetyConnect program is a comprehensive, personalised safety management programme designed to dovetail into pre‐existing Federally Accredited Principle run programmes. -

Dhupuma College Yearbook 1973.Pdf
YEAR BOOK 1973 Some of the walkers gathering at Gave Airport a little after dawn. DHUPUMA WALKATHON The Dhupuma Walkathon - 14 miles from Gove Airport to Wallaby Beach camp - was Dhupuma's first fund raising effort. Eighty-one walkers left the airport a little before 6.30 a.m. under very overcast conditions. The walkers were drenched by rain several times during their long hike, but this helped to keep all relatively cool and fresh. The aim was to cover as many sponsored miles as possible, rather than make a race of it. However, those keen to take line honours ran most of the way and the fourteen miles was covered in the time of 2 hours 18 minutes by Peter Darlison of Nhulunbuy Area School, closely followed by the first Dhupuma student, Rick Bayung, and several others. The slowest walkers took 4 hours and 20 minutes to cover the course, but these were three seven-year-olds, who did well to complete the walk. Only five walkers retired before the finish, and each of these covered more than eight miles. The main fund-raiser was Mr. Des O'Dowd, Gove Li cns Club representative @ $10 per mile plus several other sponsors. The leading fund-raiser from the Dhupuma students was Linda Galaway. The walkathon raised approximately $700 for the Dhupuma Social and Sporting Club Inc. and will be used to purchase recreation materials for the students' recreation rooms and dormitories. The only real damper on the day was the washout of the barbecue at Drimmie Head for walkers and their friends after the event. -
Airport Categorisation List
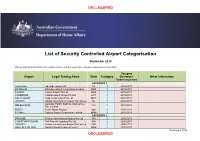
UNCLASSIFIED List of Security Controlled Airport Categorisation September 2018 *Please note that this table will continue to be updated upon new category approvals and gazettal Category Airport Legal Trading Name State Category Operations Other Information Commencement CATEGORY 1 ADELAIDE Adelaide Airport Ltd SA 1 22/12/2011 BRISBANE Brisbane Airport Corporation Limited QLD 1 22/12/2011 CAIRNS Cairns Airport Pty Ltd QLD 1 22/12/2011 CANBERRA Capital Airport Group Pty Ltd ACT 1 22/12/2011 GOLD COAST Gold Coast Airport Pty Ltd QLD 1 22/12/2011 DARWIN Darwin International Airport Pty Limited NT 1 22/12/2011 Australia Pacific Airports (Melbourne) MELBOURNE VIC 1 22/12/2011 Pty. Limited PERTH Perth Airport Pty Ltd WA 1 22/12/2011 SYDNEY Sydney Airport Corporation Limited NSW 1 22/12/2011 CATEGORY 2 BROOME Broome International Airport Pty Ltd WA 2 22/12/2011 CHRISTMAS ISLAND Toll Remote Logistics Pty Ltd WA 2 22/12/2011 HOBART Hobart International Airport Pty Limited TAS 2 29/02/2012 NORFOLK ISLAND Norfolk Island Regional Council NSW 2 22/12/2011 September 2018 UNCLASSIFIED UNCLASSIFIED PORT HEDLAND PHIA Operating Company Pty Ltd WA 2 22/12/2011 SUNSHINE COAST Sunshine Coast Airport Pty Ltd QLD 2 29/06/2012 TOWNSVILLE AIRPORT Townsville Airport Pty Ltd QLD 2 19/12/2014 CATEGORY 3 ALBURY Albury City Council NSW 3 22/12/2011 ALICE SPRINGS Alice Springs Airport Pty Limited NT 3 11/01/2012 AVALON Avalon Airport Australia Pty Ltd VIC 3 22/12/2011 Voyages Indigenous Tourism Australia NT 3 22/12/2011 AYERS ROCK Pty Ltd BALLINA Ballina Shire Council NSW 3 22/12/2011 BRISBANE WEST Brisbane West Wellcamp Airport Pty QLD 3 17/11/2014 WELLCAMP Ltd BUNDABERG Bundaberg Regional Council QLD 3 18/01/2012 CLONCURRY Cloncurry Shire Council QLD 3 29/02/2012 COCOS ISLAND Toll Remote Logistics Pty Ltd WA 3 22/12/2011 COFFS HARBOUR Coffs Harbour City Council NSW 3 22/12/2011 DEVONPORT Tasmanian Ports Corporation Pty. -

MINUTES AAA Northern Territory Division Annual General Meeting
MINUTES AAA Northern Territory Division Annual General Meeting 21 November 2016 Held as part of the 2016 AAA National Conference, Canberra Convention Centre Chair: Tom Ganley Members: Tom Ganley, Darwin International Airport (AAA NT CHAIR); Les Mitchell, Nhulunbuy Corporation – Gove Airport (AAA NT DEPUTY CHAIR); Dave Batic and Davy Maddick‐Semal, Alice Springs and Tennant Creek Airports. The meeting opened at 1500 AEDT on 21 May 2016. PROCEDURAL MATTERS 1.1 Quorum Members NOTED that a Quorum was present at the meeting. 1.2 Adoption of Agenda Members unanimously RESOLVED to adopt the agenda provided. APOLOGIES 2.1 Members NOTED the apology of Ian Kew (Darwin Airport). MEMBER DISCLOSURES 3.1 Declaration of Interest / Conflicts of Interest Members NOTED that there were no additional conflicts declared. PREVIOUS MINUTES 4.1 12 May 2016 Meeting Members NOTED minutes of previous meeting conducted 12 May 2016. MATTERS FOR DISCUSSION 5.1 Airport Reporting Officer Resource Members discussed the concept of utilizing existing Airport Reporting Officers (ARO’s) from Alice Springs Airport to cover periods of leave and works at Gove, Ayers Rock and other Territory Airports. Members AGREED to explore this concept further as ARO retention is an issue and this may be a way of providing broader experience and encouraging retention and rotation at remote airports. 1 5.2 Regional Airport Masterplan Members NOTED that the AAA has a regional airport masterplan template. Members suggested this may be a suitable template for which many remote airports across the Territory could benefit. GENERAL BUSINESS 6.1 There were no items of General Business. -

AO-2016-062 Final – 14 October 2016
Separation issue due to runway incursion involving Cessna 172, VH-EKV, and Beech 58, VH-MLB Alice Springs Airport, Northern Territory, 16 June 2016 ATSB Transport Safety Report Aviation Occurrence Investigation AO-2016-062 Final – 14 October 2016 Released in accordance with section 25 of the Transport Safety Investigation Act 2003 Publishing information Published by: Australian Transport Safety Bureau Postal address: PO Box 967, Civic Square ACT 2608 Office: 62 Northbourne Avenue Canberra, Australian Capital Territory 2601 Telephone: 1800 020 616, from overseas +61 2 6257 4150 (24 hours) Accident and incident notification: 1800 011 034 (24 hours) Facsimile: 02 6247 3117, from overseas +61 2 6247 3117 Email: [email protected] Internet: www.atsb.gov.au © Commonwealth of Australia 2016 Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form license agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. -
Safetaxi Australia Coverage List - Cycle 21S5
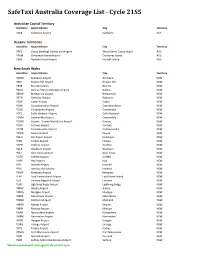
SafeTaxi Australia Coverage List - Cycle 21S5 Australian Capital Territory Identifier Airport Name City Territory YSCB Canberra Airport Canberra ACT Oceanic Territories Identifier Airport Name City Territory YPCC Cocos (Keeling) Islands Intl Airport West Island, Cocos Island AUS YPXM Christmas Island Airport Christmas Island AUS YSNF Norfolk Island Airport Norfolk Island AUS New South Wales Identifier Airport Name City Territory YARM Armidale Airport Armidale NSW YBHI Broken Hill Airport Broken Hill NSW YBKE Bourke Airport Bourke NSW YBNA Ballina / Byron Gateway Airport Ballina NSW YBRW Brewarrina Airport Brewarrina NSW YBTH Bathurst Airport Bathurst NSW YCBA Cobar Airport Cobar NSW YCBB Coonabarabran Airport Coonabarabran NSW YCDO Condobolin Airport Condobolin NSW YCFS Coffs Harbour Airport Coffs Harbour NSW YCNM Coonamble Airport Coonamble NSW YCOM Cooma - Snowy Mountains Airport Cooma NSW YCOR Corowa Airport Corowa NSW YCTM Cootamundra Airport Cootamundra NSW YCWR Cowra Airport Cowra NSW YDLQ Deniliquin Airport Deniliquin NSW YFBS Forbes Airport Forbes NSW YGFN Grafton Airport Grafton NSW YGLB Goulburn Airport Goulburn NSW YGLI Glen Innes Airport Glen Innes NSW YGTH Griffith Airport Griffith NSW YHAY Hay Airport Hay NSW YIVL Inverell Airport Inverell NSW YIVO Ivanhoe Aerodrome Ivanhoe NSW YKMP Kempsey Airport Kempsey NSW YLHI Lord Howe Island Airport Lord Howe Island NSW YLIS Lismore Regional Airport Lismore NSW YLRD Lightning Ridge Airport Lightning Ridge NSW YMAY Albury Airport Albury NSW YMDG Mudgee Airport Mudgee NSW YMER Merimbula