Annual Progress Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

SR. NO. Village Name Taluka District Region
SR. NO. Village Name Taluka District Region 1 Sidhpur Gangapur Aurangabad Aurangabad DPAP 2 Manulapur Gangapur Aurangabad Aurangabad DPAP 3 Manjari Gangapur Aurangabad Aurangabad DPAP 4 Phajlapur Gangapur Aurangabad Aurangabad DPAP 5 Wahegaon Gangapur Aurangabad Aurangabad DPAP 6 Sudeshwadgaon Gangapur Aurangabad Aurangabad DPAP 7 Alamgirpur Gangapur Aurangabad Aurangabad DPAP 8 Hakigatpur Gangapur Aurangabad Aurangabad DPAP 9 Katepimpalgaon Gangapur Aurangabad Aurangabad DPAP 10 Ankoli Wadagaon Gangapur Aurangabad Aurangabad DPAP 11 Aminabad Gangapur Aurangabad Aurangabad DPAP 12 Arapur Gangapur Aurangabad Aurangabad DPAP 13 Gavalidhnora Gangapur Aurangabad Aurangabad DPAP 14 Pratappur Gangapur Aurangabad Aurangabad DPAP 15 Chandikapur Gangapur Aurangabad Aurangabad DPAP 16 Wadgaon Gangapur Aurangabad Aurangabad DPAP 17 Rampuri Gangapur Aurangabad Aurangabad DPAP 18 Gavalishiwra Gangapur Aurangabad Aurangabad DPAP 19 Lanzi Gangapur Aurangabad Aurangabad DPAP 20 Hirapur Gangapur Aurangabad Aurangabad DPAP 21 Mustaphabad Gangapur Aurangabad Aurangabad DPAP 22 Ambegaon Gangapur Aurangabad Aurangabad DPAP 23 Gangapur Gangapur Aurangabad Aurangabad DPAP 24 Jakhmatha Gangapur Aurangabad Aurangabad DPAP 25 Ambewadi Gangapur Aurangabad Aurangabad DPAP 26 Sanjarpur Gangapur Aurangabad Aurangabad DPAP 27 Jamgaon Gangapur Aurangabad Aurangabad DPAP 28 Nawabpur Gangapur Aurangabad Aurangabad DPAP 29 Sirasgaon Gangapur Aurangabad Aurangabad DPAP 30 Maluja Ku. Gangapur Aurangabad Aurangabad DPAP 31 Shariphur Gangapur Aurangabad Aurangabad DPAP 32 Hadiyabad -

District Taluka Center Name Contact Person Address Phone No Mobile No
District Taluka Center Name Contact Person Address Phone No Mobile No Mhosba Gate , Karjat Tal Karjat Dist AHMEDNAGAR KARJAT Vijay Computer Education Satish Sapkal 9421557122 9421557122 Ahmednagar 7285, URBAN BANK ROAD, AHMEDNAGAR NAGAR Anukul Computers Sunita Londhe 0241-2341070 9970415929 AHMEDNAGAR 414 001. Satyam Computer Behind Idea Offcie Miri AHMEDNAGAR SHEVGAON Satyam Computers Sandeep Jadhav 9881081075 9270967055 Road (College Road) Shevgaon Behind Khedkar Hospital, Pathardi AHMEDNAGAR PATHARDI Dot com computers Kishor Karad 02428-221101 9850351356 Pincode 414102 Gayatri computer OPP.SBI ,PARNER-SUPA ROAD,AT/POST- 02488-221177 AHMEDNAGAR PARNER Indrajit Deshmukh 9404042045 institute PARNER,TAL-PARNER, DIST-AHMEDNAGR /221277/9922007702 Shop no.8, Orange corner, college road AHMEDNAGAR SANGAMNER Dhananjay computer Swapnil Waghchaure Sangamner, Dist- 02425-220704 9850528920 Ahmednagar. Pin- 422605 Near S.T. Stand,4,First Floor Nagarpalika Shopping Center,New Nagar Road, 02425-226981/82 AHMEDNAGAR SANGAMNER Shubham Computers Yogesh Bhagwat 9822069547 Sangamner, Tal. Sangamner, Dist /7588025925 Ahmednagar Opposite OLD Nagarpalika AHMEDNAGAR KOPARGAON Cybernet Systems Shrikant Joshi 02423-222366 / 223566 9763715766 Building,Kopargaon – 423601 Near Bus Stand, Behind Hotel Prashant, AHMEDNAGAR AKOLE Media Infotech Sudhir Fargade 02424-222200 7387112323 Akole, Tal Akole Dist Ahmadnagar K V Road ,Near Anupam photo studio W 02422-226933 / AHMEDNAGAR SHRIRAMPUR Manik Computers Sachin SONI 9763715750 NO 6 ,Shrirampur 9850031828 HI-TECH Computer -
Scanned by Camscanner Scanned with Camscanner
Scanned by CamScanner Scanned with CamScanner YEAR 2019-20 (Draft Report) DISTRICT SURVEY REPORT For Sand Mining or River Bed Mining Prepared as per Gazette Notification S.O. 3611 (E) Dated. 25.07.2018 AURANGABAD, MAHARASHTRA Prepared By District Mining Officer, Aurangabad 1. INTRODUCTION Hon'ble Supreme Court of India dated 27th February, 2012 in I.A. No.12-13 of 2011 in Special Leave Petition (C) No.19628-19629 of 2009, in the matter of Deepak Kumar etc. Vs. State of Haryana and Others etc., prior environmental clearance has made mandatory for mining of minor minerals irrespective of the area of mining lease. Accordingly, Ministry of Environment, Forest & Climate Change (MoEF & CC) had issued Office Memorandum No. LllOll/47/2011-IA.II(M) dated 18th May 2013. As per this O.M. all mining projects of minor minerals would henceforth require prior Environmental Clearance irrespective of the lease area. The stone quarry and sand quarrying projects need environmental clearance as per the MoEF guidelines and such pg. 47 projects are treated as Category ‘B' even if the lease area is less than 5 Ha. Subsequently, various amendments were made as regards to obtain environmental clearance of the minor minerals. The Hon'ble National Green Tribunal, vide its order dated the 13th January, 2015 in the matter regarding sand mining has directed for making a policy on environmental clearance for mining leases in cluster for minor minerals. As per the latest amendment S.O. 141 (E) & S.O.190(E) dated 15th January 2016 & 20th January in exercise of the powers conferred by sub-section (3) of Section 3 of the Environment (Protection) Act, 1986 (29 of 1986) and in pursuance of notification of Ministry of Environment and Forest number S.O. -
![District Survey Report [Compatibility Mode]](https://docslib.b-cdn.net/cover/1086/district-survey-report-compatibility-mode-431086.webp)
District Survey Report [Compatibility Mode]
Map of Aurangabad District Sand Belts 2016-17 details in Aurangabad District ° Total Tahsils – 06 (Kannad, Paithan, Phulambri, Sillod, Gangapur, Vaijapur) [No sand ghats are available from other Tahsils this time] ° Total Rivers – 08 (Shivna, Godavari, Girija, Purna, Kharinala, Khari, Anjana, Kelna) ° Sand Belts - 37 (On District Level Sand Ghat – 35, Joint Sand Ghats – 02) ° Average Rain fall in District – 675.46 mm • But actual Rainfall – 617.28 mm (91%) Sand Belt Allotment And Monitoring System Proposals (from Tahsildars) – 99 Joint Surveys (DMO, Tahsildars and GSDA officers) – 99 Total Approved Sandghats from GSDA - 58 Prefeasibility Report + G. P. NOC/SDO’s Positive Reports – 37 Hon. Divisional Commissioner Approval – 37 (On District Level Sand Ghat – 35, Joint Sand Ghats – 02) E – Tendering, E – Auction with due process. Map of Tahsils in Aurangabad District Tahsil - Kannad Tahsils Sand Belts (08) River Area 1. Kannad i. Borsar Kh Shivna 3.00 ii. Borsar Bk Shivna 3.00 iii. Shevta Shivna 0.90 iv. Kanadgaon Kharinala 0.06 v. Khaparkheda Khari 0.50 vi. Nadarpur Anjana 0.40 vii. Javkheda kh Anjana 0.13 viii. Amdabad Anjana 0.09 Total area in Hectare – 8.08 Total Quantity of available sand in Brass - 83946 Tahsil - Paithan Tahsils Sand Belts (07) River Area 2. Paithan i. Pategaon Godavari 2.00 ii. Naygaon-I Godavari 3.50 iii. Naygaon-II Godavari 3.50 iv. Vadvali Godavari 2.00 v. Vaghadi Godavari 0.13 vi. Maygaon Godavari 0.10 vii. Navgaon Godavari 0.09 Total area in Hectors – 11.13 Total Quantity of available sand in Brass – 22047 Tahsil - Phulambri Tahsils Sand Belts (07) River Area 3. -

Report on AQUIFER MAPS and GROUND WATER MANAGEMENT PLAN Soygaon and Sillod Taluka, Aurangabad District, Maharashtra (Part-I)
Draft Report क� द्र�यभू�म �ल बो जल संसाधन, नद� �वकास और गंगा संर�ण मंत्रा भारत सरकार Central Ground Water Board Ministry of Water Resources, River Development and Ganga Rejuvenation Government of India Report on AQUIFER MAPS AND GROUND WATER MANAGEMENT PLAN Soygaon and Sillod Taluka, Aurangabad District, Maharashtra (Part-I) म鵍ा �ेत, नागपुर Central Region, Nagpur Government of India Ministry of Water Resources, River Development & Ganga Rejuvenation CENTRAL GROUND WATER BOARD AQUIFER MAPS AND GROUND WATER MANAGEMENT PLAN OF SOYGAON AND SILLOD TALUKA, AURANGABAD DISTRICT, MAHARASHTRA CENTRAL REGION, NAGPUR November 2016 1 PART-I BRIEF REPORT ON AQUIFER MAPS AND GROUND WATER MANAGEMENT PLANS, SOYGAON AND SILLOD TALUKA, AURANGABAD DISTRICT CONTRIBUTORS’ Principal Authors Kartik P. Dongre : Scientist-C Sandeep D. Waghmare : Assistant Hydrogeologist Supervision & Guidance D. Subba Rao : Regional Director Dr. P.K. Jain : Supdtg. Hydrogeologist Hydrogeology, GIS maps and Management Plan Kartik P. Dongre : Scientist-C Sandeep D. Waghmare : Assistant Hydrogeologist J. R. Verma : Scientist-D Rahul R. Shende : Assistant Hydrogeologist Groundwater Exploration Kartik P. Dongre : Scientist-C Sandeep D. Waghmare : Assistant Hydrogeologist Chemical Analysis Dr. Devsharan Verma : Scientist B (Chemist) Dr. Rajni Kant Sharma : Scientist B (Chemist) T. Dinesh Kumar : Assistant Chemist 2 PART-I BRIEF REPORT ON AQUIFER MAPS AND GROUND WATER MANAGEMENT PLANS, SOYGAON AND SILLOD TALUKA, AURANGABAD DISTRICT CONTENTS 1 INTRODUCTION 1.1 Objective and Scope 1.2 -

1 Aurangabad Rural Kannad 33 Kv Aurala 10.00 2 Aurangabad Rural Kannad 33 KV Andhaner 10.00 3 Aurangabad Rural Kannad 33 KV Chap
ADDENDUM-1 T-24(Aurangabad) Tentative list of MSEDCL sub-stations for grid connectivity at 22 or 11KV Level of proposed 2 to 10 MW Solar generation projects to be developed under this tender Capacity Available Sr.No. Name of Circle Name of Taluka Name of S/s in MW for Solar Project 1 Aurangabad Rural Kannad 33 Kv Aurala 10.00 2 Aurangabad Rural Kannad 33 KV Andhaner 10.00 3 Aurangabad Rural Kannad 33 KV Chapaner 10.00 4 Aurangabad Rural Kannad 33 Kv Jehur 5.00 5 Aurangabad Rural Kannad 33 Kv Hatnur 10.00 6 Aurangabad Rural Kannad 33 Kv Kannad 10.00 7 Aurangabad Rural Kannad 33/11 kV Wasadi substation 10.00 8 Aurangabad Rural Kannad 33/11 kV Nagad substation 10.00 9 Aurangabad Rural Sillod Sillod 10.00 10 Aurangabad Rural Sillod Khodkai 10.00 11 Aurangabad Rural Sillod Bhavan 10.00 12 Aurangabad Rural Sillod Andhari 10.00 13 Aurangabad Rural Sillod Bharadi 15.00 14 Aurangabad Rural Sillod Golegaon 15.00 15 Aurangabad Rural Sillod Ambhai 10.00 16 Aurangabad Rural Sillod Ajantha 10.00 17 Aurangabad Rural Sillod Anwi 10.00 18 Aurangabad Rural Soygaon Faradapur 15.00 19 Aurangabad Rural Soygaon Soygaon 10.00 20 Aurangabad Rural VAIJAPUR VAIJAPUR URBAN 10.00 21 Aurangabad Rural VAIJAPUR LADGAON 10.00 22 Aurangabad Rural VAIJAPUR SHIVRAI 5.00 23 Aurangabad Rural VAIJAPUR NAGAMTHAN 10.00 24 Aurangabad Rural VAIJAPUR CHICHADGAON 10.00 25 Aurangabad Rural VAIJAPUR 33/11 KV KHANDALA 10.00 26 Aurangabad Rural VAIJAPUR 33/ 11 KV PARSODA 10.00 27 Aurangabad Rural VAIJAPUR 33/11 KV LONI 10.00 28 Aurangabad Rural VAIJAPUR 33/11 KV GARAJ 10.00 29 Aurangabad -

Quality of Ground Water in Aurangabad District (Maharashtra, India) Using Geostatistical Method
IJISET - International Journal of Innovative Science, Engineering & Technology, Vol. 2 Issue 2, February 2015. www.ijiset.com ISSN 2348 – 7968 Quality of Ground Water in Aurangabad District (Maharashtra, India) using Geostatistical Method. Rahul Sagar Department of Computer Science, Vinayakrao Patil College, Vaijapur Aurangabad, Maharashtra, 423701, India Abstract pollution and losing of water sources have changed Groundwater is one of the major sources of water in exploitation policy of water and soil sources [3]. arid and semi -arid regions. Groundwater quality data In this research our aim is to estimate ground water and its spatial distribution are important for the purpose chemical quality using spatial interpolation techniques of planning and management. Geo-statistical methods several studies shown that interpolation technique are one of the most advanced techniques for accuracy is analyzed for soil & water properties. Several interpolation of groundwater quality. In this study, research shown that using kriging method to estimate kriging methods were used for predicting spatial spatial prediction of Groundwater to estimate one variable distribution of some groundwater quality parameters depends on variables type and regional factors which such as: pH, Alkalinity, salinity, dissolved influence this and any selected method for given region oxygen(DO), Biological oxygen cannot be generalized to others use of geo-statistics demand(BOD),Chloride(Cl), Sulphate method for analyzing Groundwater quality to estimate EC, (So4),Nitrate(No3), Calcium Hardness( CaH), CL, SO4, NO3, TDS has suitable accuracy to estimate Magnesium Hardness( MgH), and Total Hardness Groundwater quality [4, 5]. (TH). Data were collected from fixed eight (08) dug The present study was therefore, carried out with wells and bore wells in Aurangabad district the aim of spatial interpolation techniques for mapping (Maharashtra, India). -
List of Ginning & Pressing Units Rated Under Scheme on “Assessment
List of Ginning & Pressing Units Rated under scheme on “Assessment & Rating of G&P factories” SR. REGN NO NAME & ADDRESS DIST/ CONTACT RATING RATING NO OF THE FACTORY TALUKA PERSON & AWARDED CERTIFICATE PHONE NO VALID UPTO 1. G&P/0009 AMIT COTTONS PVT. LTD MAHABOOBN Hemant 5 Star SY.NO.745, NH – 7, AGAR Gujarathi 17.08.2014 CHINTAGUDEM (V), 9000300371 EHADNAGAR, DIST:MAHABUBNAGAR (AP) PIN – 509 202 2. G&P/0010 JALARAM COTTON & RAJKOT Anand Popat 5 Star PROTEINS LTD 9426914910 24.11.2013 JASDAN- AHMEDABAD 02821222201 HIGHWAY, JASDAN, DIST: RAJKOT, GUJARAT, PIN: 360 050 3. G&P/0034 SHRI BALAJI FIBERS YAVATMAL Madhusudan 5 Star GAT NO:61/2 07153244430 27.6.2015 VILLAGE LALGUDA, TAL:WANI, 9881715174 DIST:YAVATMAL-445304 MAHARASHTRA 4. G&P/0041 GIRIRAJ COTEX P.LTD RAJKOT Bharatbhai 5 Star GADHADIYA ROAD, 02827270453 17.08.2014 GADHADIYA 9825077522 TAL: JASDAN, DIST;RAJKOT - 360050 GUJARAT 5. G&P/0056 LOKNAYAK JAYPRAKASH NANDURBAR R.D.Patil 5 Star NARAYAN SHETKARI 02565229996 24.11.2013 SAHAKARI SOOT GIRNI LTD, 9881925174 KAMALNAGAR UNTAWAD HOL TAL. SHAHADA DIST: NANDURBAR MAHARASHTRA 6. G&P/0096 ADITYA COTTON & OIL KARIMNAGAR Mukka 5 Star AGROTECH INDUSTRIES Narayana 24.11.2013 POST: JAMMIKUNTA 08727 253754 DIST: KARIMNAGAR – 505122 9866171754 A.P. 7. G&P/027 6 RIMTEX ENGINEERING SURENDRAN Manubhai 5 Star PVT.LTD., AGAR Parmar 24.11.2013 (UNIT COTTON GINNING & 02752-243322 PRESSING) 9825223519 VIRAMGAM, SURENDRANAGAR ROAD, AT.DEDUDRA, TAL.WADHWAN, DIST SURENDRANAGAR GUJARAT 8. G&P/0290 TUNGABHADRA GINNING & BELLARY K G Thimma 5 Star PRESSING Reddy 24.11.2013 FACTORY,NO.87/B,3/4, 08392250383 T.S.NO.970, WARD 10 B, 9448470112 ANDRAL ROAD, BELLARY, KARNATAKA 9. -
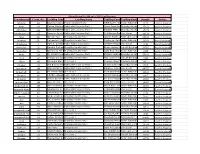
Exit Polls 2014 State Wise
Status Known For 288 out of 288 Constituencies Constituency Const. No. Leading Candidate Leading Party Trailing CandidateTrailing Party Margin Status Achalpur 42 Bachchu BabaraoPrahar Kadu Janshakti Party ANIRUDDHA ALIASIndian BABLUBHAU National SUBHANRAOCongress7616 i DESHMUKHResult in Progress Aheri 69 Aatram DharamraobabaNationalist Bhagwantrao Congress Party i Atram AmbrishraoBharatiya Raje Satyavanrao Janata Party15458 i Result in Progress Ahmadpur 236 BABASAHEB MOHANRAONationalist PATIL Congress Party i JADHAV PATIL VINAYAKRAOBharatiya Janata KISHANRAO Party27871 i Result in Progress Ahmednagar City 225 Sangram ArunkakaNationalist Jagtap Congress Party i Anil Bhaiyya RamkisanShiv Sena Rathod i 11139 Result in Progress Airoli 150 Ganesh Naik Bharatiya Janata Party i Ganesh Raghu ShindeNationalist Congress Party68832 i Result in Progress Akkalkot 250 Kalyanshetti SachinBharatiya Panchappa Janata Party i Siddharam SatlingappaIndian MhetreNational Congress36769 i Result Declared Akkalkuwa 1 ADV. K. C. PADAVIIndian National Congress i AAMSHYA FULJI PADAVIShiv Sena i 2096 Result Declared Akola East 31 Randhir PralhadraoBharatiya Sawarkar Janata Party i Bhade Haridas PandhariVanchit Bahujan Aaghadi24723 i Result Declared Akola West 30 Govardhan MangilalBharatiya Sharma Janata @ Lalaji Party i Sajid Khan MannanIndian Khan National Congress2662 i Result in Progress Akole 216 Dr. KIRAN YAMAJINationalist LAHAMATE Congress Party i PICHAD VAIBHAVBharatiya MADHUKARRAO Janata Party57689 i Result Declared Akot 28 Prakash GunwantraoBharatiya Bharsakale Janata Party i Adv. Santosh VasantVanchit Rahate Bahujan Aaghadi8828 i Result in Progress Alibag 192 Mahendra Hari DalviShiv Sena i Subhash Alias PanditshetPeasants Patil And Workers28130 Party of IndiaResult i in Progress Amalner 15 Anil Bhaidas PatilNationalist Congress Party i Shirish Dada HiralalBharatiya Chaudhari Janata Party7805 i Result in Progress Ambegaon 196 Dilip Dattatray WalseNationalist Patil Congress Party i Bankhele RajaramShiv Bhivsen Sena i 66775 Result Declared Ambernath 140 Dr. -

District Census Handbook, Aurangabad, Part XII-A & B, Series-14
CENSUS OF INDIA 1991 DISTRICT dENSUS HANDBOOK AURANGABAD Compiled by THE MAHARASHTRA CENSUS DIRECTORATE PRINTED IN INDIA BY THE MANAGER, GOVERNMENT CENTRAL PRESS, MUMBAI 400 004 AND PUBLISHED BY THE DIRECTOR, GOVERNMENT PRINTING AND STATIONERY, MAHARASHTRA STATE MUMBAI· 400 004. 1995 [Price : Rs. 100.00] '"a 3 0 MAHARASHTRA .E G g A 0 N DISTRICT AURANGABAD A L Km I, 0 I, B 11 16 Km ........... I '\ - Part of District Jalno V - Part of TahSil Vailopur 5 - Port of T ohsil 50egoon. M5H - Major Stote Highway. z « .. .., Vl u a o Vl c H M o Oistrict H,adquarttrs 15 AtsoTh. Tahsil Htadquart,rs. o DISTRICT AURANOAIAD G CHANGE IN JURISDICTION 1981- 91 ""~'Km ;C,_ rr ...."'r)' -1 BOUNDARY, DISTRICT .. .' TAHSIL .. ( 0 •.[" HEADQUARTERS. DISTRICT, TAHSIL ... @;@ --/ SH16 r'i..'> STATE HIGHWAY .. ') DIS! RIC! IMPORTANT ME'TALLED ROAD ~ AURANG4BAD RAILWAY LINE WITH STATION, BROAD GAUGE -t RS r , ,~ r' METRE GAUGE -'-~ RIVER AND STREAM ~~.--..... _.... VILLAGE HAVING 5000 AND ABOVE Gonor, '~ POPULATION WITH NAME '" • "t ... URBAN AREA WITH POPULATION SIZE Boundary, District _._,_._ CLASS 1 , 1II , Jl[ AND J[ ... ~ ArliO lost to Newly Crfated POST AND TELEGRAPH OF'FICE .. , ••••PTa ~ Jolna Olstrict. DEGREE COLLEGE AND TECHNICAL INSTITUTION •• riiI rn _ Area lost to Ahmadnagor District Based Upon of Indio mop WIth the permISSion of the Sur'.leyor General of India Sur'le~ © Government of india COP1rlqllt, 199". MOTIF •• • ••c· • • Paithani sarees are among the costliest sarees in the world. Paithani at one time a must for every Maharashtrian bride. It derives its name from Paithan in Aurangabad district. -

Notice for Appointment of Regular / Rural Retail Outlet Dealership HPC Proposes to Appoint Retail Outlet Dealers in Maharashtra, As Per Following Details
Notice for appointment of Regular / Rural Retail Outlet Dealership HPC proposes to appoint Retail Outlet Dealers in Maharashtra, as per following details: Estimate Fixed Security Finance to be d Category Type of Minimum Dimensions (in M) / Mode of Fee / Deposit ( Sl No Name Of Location Revenue District Type of RO arranged by the monthly Site * Area of the site (in Sq. M.).* selection Minimu Rs in Applicant Sales m Bid Lakhs) 1 2 3 4 5 6 7 8 9(a) 9(b) 10 11 12 SC Estimat SC CC 1 Estimate ed SC PH d fund working ST required capital ST CC 1 for require ST PH develop Draw of (Regular/Rural MS+HSD CC / DC Fronta ment OBC Depth Area ment of Lots/Biddi ) in Kls /CFS ge for OBC CC 1 infrastru ng operati OBC PH cture at on of OPEN RO (Rs RO (Rs OPEN CC 1 in Lakhs in OPEN CC 2 ) Lakhs) OPEN PH FROM JAFRABAD PHATA IN CHIKHLI CITY TOWARDS JAFRABAD UP TO 5 DRAW OF 1 BULDHANA Regular 150 SC CFS 40 50 2000 0 0 0 3 KM ON SH-228 LOTS WITHIN 3 KM FROM SHELU BAZAR JUNCTION, LHS ON SHELUBAZAR DRAW OF 2 WASHIM Regular 152 SC CFS 40 50 2000 0 0 0 3 KARANJA ROAD TOWARDS KARANJA LOTS WITHIN 4 KM OF KHEMANAND ENGLISH SCHOOL TOWARDS BHOOM DRAW OF 3 AHMEDNAGAR Regular 150 ST CFS 40 50 2000 0 0 0 3 ON AHMEDNAGAR BHOOM ROAD SH-157 LOTS UPTO 4 KM FROM KRISHI UTPANNA BAZAR SAMITI GATE, LONI KHURD DRAW OF 4 AHMEDNAGAR Regular 150 ST CFS 40 50 2000 0 0 0 3 TOWARDS SINNAR ON SH 31 LOTS 5 VILLAGE KADRABAD, ON KADRABAD-KACHNER ROAD AURANGABAD Regular 150 SC CFS 40 50 2000 0 0 DRAW OF 0 3 DRAW OF 6 VILLAGE BHATKUDGAON ON SH- 44 ON NEWASA–SHEVGAON ROAD AHMEDNAGAR Regular -

Brief Industrial Profile of Aurangabad District
Government of India Ministry of MSME Brief Industrial Profile of Aurangabad District Carried out by Br.MSME-Development Institute, Aurangabad (Ministry of MSME, Govt. of India) Phone: 0240-2485430 E-mail: [email protected] 1 Contents Sl. Topic Page No. No. 1.0 General Characteristics of the District 03 1.1 Location & Geographical Area 03 1.2 Topography 03 1.3 Availability of Minerals 03 1.4 Forest 03 1.5 Administrative set up 04 2.0 District at a glance 05-08 2.1 Existing status of Industrial Area in the District Aurangabad 09 3.0 Industrial Scenario of Aurangabad 09 3.1 Industry at Glance 09 3.2 Year wise trend of units registered 10 3.3 Details of existing Micro & Small Enterprises & Artisan Units in 11-12 the District 3.4 Medium/Large Scale Industries/Public Sector Undertakings 13-30 3.5 Major Exportable Items 31 3.6 Growth Trend 31-32 3.7 Vendorisation / Ancillarisation of the Industry/Potential areas 33 3.8 Medium Scale Enterprises 33 3.8.1 List of the units in Aurangabad & nearby areas 33 3.9 Service Enterprises 33 3.9.2 Potential areas for service industry 34-35 3.10 Potential for new MSMEs 35-41 4.0 Existing clusters of Micro & Small Enterprise 42 4.1 Details of Major Clusters 42 4.1.1 Manufacturing Sector 42-45 4.1.2 Service Sector 46 4.2 Details of identified cluster 46 4.2.1 Name of the Cluster 46 5.0 General issues raised by Industries Association during the course 46 of meeting 6.0 Steps to set up MSMEs 47 7.0 Additional information if any 48-49 2 Brief Industrial Profile of Aurangabad District 1.