Download File
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

University of California, San Diego
UNIVERSITY OF CALIFORNIA, SAN DIEGO The post-terminal differentiation fate of RNAs revealed by next-generation sequencing A dissertation submitted in partial satisfaction of the requirements for the degree Doctor of Philosophy in Biomedical Sciences by Gloria Kuo Lefkowitz Committee in Charge: Professor Benjamin D. Yu, Chair Professor Richard Gallo Professor Bruce A. Hamilton Professor Miles F. Wilkinson Professor Eugene Yeo 2012 Copyright Gloria Kuo Lefkowitz, 2012 All rights reserved. The Dissertation of Gloria Kuo Lefkowitz is approved, and it is acceptable in quality and form for publication on microfilm and electronically: __________________________________________________________________ __________________________________________________________________ __________________________________________________________________ __________________________________________________________________ __________________________________________________________________ Chair University of California, San Diego 2012 iii DEDICATION Ma and Ba, for your early indulgence and support. Matt and James, for choosing more practical callings. Roy, my love, for patiently sharing the ups and downs of this journey. iv EPIGRAPH It is foolish to tear one's hair in grief, as though sorrow would be made less by baldness. ~Cicero v TABLE OF CONTENTS Signature Page .............................................................................................................. iii Dedication .................................................................................................................... -

Supplemental Table S1
Entrez Gene Symbol Gene Name Affymetrix EST Glomchip SAGE Stanford Literature HPA confirmed Gene ID Profiling profiling Profiling Profiling array profiling confirmed 1 2 A2M alpha-2-macroglobulin 0 0 0 1 0 2 10347 ABCA7 ATP-binding cassette, sub-family A (ABC1), member 7 1 0 0 0 0 3 10350 ABCA9 ATP-binding cassette, sub-family A (ABC1), member 9 1 0 0 0 0 4 10057 ABCC5 ATP-binding cassette, sub-family C (CFTR/MRP), member 5 1 0 0 0 0 5 10060 ABCC9 ATP-binding cassette, sub-family C (CFTR/MRP), member 9 1 0 0 0 0 6 79575 ABHD8 abhydrolase domain containing 8 1 0 0 0 0 7 51225 ABI3 ABI gene family, member 3 1 0 1 0 0 8 29 ABR active BCR-related gene 1 0 0 0 0 9 25841 ABTB2 ankyrin repeat and BTB (POZ) domain containing 2 1 0 1 0 0 10 30 ACAA1 acetyl-Coenzyme A acyltransferase 1 (peroxisomal 3-oxoacyl-Coenzyme A thiol 0 1 0 0 0 11 43 ACHE acetylcholinesterase (Yt blood group) 1 0 0 0 0 12 58 ACTA1 actin, alpha 1, skeletal muscle 0 1 0 0 0 13 60 ACTB actin, beta 01000 1 14 71 ACTG1 actin, gamma 1 0 1 0 0 0 15 81 ACTN4 actinin, alpha 4 0 0 1 1 1 10700177 16 10096 ACTR3 ARP3 actin-related protein 3 homolog (yeast) 0 1 0 0 0 17 94 ACVRL1 activin A receptor type II-like 1 1 0 1 0 0 18 8038 ADAM12 ADAM metallopeptidase domain 12 (meltrin alpha) 1 0 0 0 0 19 8751 ADAM15 ADAM metallopeptidase domain 15 (metargidin) 1 0 0 0 0 20 8728 ADAM19 ADAM metallopeptidase domain 19 (meltrin beta) 1 0 0 0 0 21 81792 ADAMTS12 ADAM metallopeptidase with thrombospondin type 1 motif, 12 1 0 0 0 0 22 9507 ADAMTS4 ADAM metallopeptidase with thrombospondin type 1 -

A Computational Approach for Defining a Signature of Β-Cell Golgi Stress in Diabetes Mellitus
Page 1 of 781 Diabetes A Computational Approach for Defining a Signature of β-Cell Golgi Stress in Diabetes Mellitus Robert N. Bone1,6,7, Olufunmilola Oyebamiji2, Sayali Talware2, Sharmila Selvaraj2, Preethi Krishnan3,6, Farooq Syed1,6,7, Huanmei Wu2, Carmella Evans-Molina 1,3,4,5,6,7,8* Departments of 1Pediatrics, 3Medicine, 4Anatomy, Cell Biology & Physiology, 5Biochemistry & Molecular Biology, the 6Center for Diabetes & Metabolic Diseases, and the 7Herman B. Wells Center for Pediatric Research, Indiana University School of Medicine, Indianapolis, IN 46202; 2Department of BioHealth Informatics, Indiana University-Purdue University Indianapolis, Indianapolis, IN, 46202; 8Roudebush VA Medical Center, Indianapolis, IN 46202. *Corresponding Author(s): Carmella Evans-Molina, MD, PhD ([email protected]) Indiana University School of Medicine, 635 Barnhill Drive, MS 2031A, Indianapolis, IN 46202, Telephone: (317) 274-4145, Fax (317) 274-4107 Running Title: Golgi Stress Response in Diabetes Word Count: 4358 Number of Figures: 6 Keywords: Golgi apparatus stress, Islets, β cell, Type 1 diabetes, Type 2 diabetes 1 Diabetes Publish Ahead of Print, published online August 20, 2020 Diabetes Page 2 of 781 ABSTRACT The Golgi apparatus (GA) is an important site of insulin processing and granule maturation, but whether GA organelle dysfunction and GA stress are present in the diabetic β-cell has not been tested. We utilized an informatics-based approach to develop a transcriptional signature of β-cell GA stress using existing RNA sequencing and microarray datasets generated using human islets from donors with diabetes and islets where type 1(T1D) and type 2 diabetes (T2D) had been modeled ex vivo. To narrow our results to GA-specific genes, we applied a filter set of 1,030 genes accepted as GA associated. -

Arg206cys Substitution in DNASE1L3 Causes a Defect in DNASE1L3 Protein Secretion That Confers Risk of Systemic Lupus Erythematos
Ann Rheum Dis: first published as 10.1136/annrheumdis-2020-218810 on 17 January 2021. Downloaded from Systemic lupus erythematosus TRANSLATIONAL SCIENCE Arg206Cys substitution in DNASE1L3 causes a defect in DNASE1L3 protein secretion that confers risk of systemic lupus erythematosus Latanya N Coke ,1 Hongxiu Wen ,1 Mary Comeau ,2 Mustafa H Ghanem ,1,3 Andrew Shih ,1 Christine N Metz ,1,3 Wentian Li ,1 Carl D Langefeld ,2 Peter K Gregersen ,1,3 Kim R Simpfendorfer 1,3 Handling editor Josef S ABSTRACT Key messages Smolen Objectives To determine if the polymorphism encoding the Arg206Cys substitution in DNASE1L3 explains the ► Additional material is What is already known about this subject? published online only. To view, association of the DNASE1L3/PXK gene locus with systemic ► The coding polymorphism rs35677470 is the please visit the journal online lupus erythematosus (SLE) and to examine the effect of the causal variant for rheumatoid arthritis (RA) and (http:// dx. doi. org/ 10. 1136/ Arg206Cys sequence change on DNASE1L3 protein function. scleroderma/systemic sclerosis (SSc) association annrheumdis- 2020- 218810). Methods Conditional analysis for rs35677470 was in the DNASE1L3/PXK locus and is reported to 1 performed on cases and controls with European ancestry The Institute of Molecular eliminate DNASE1L3 enzyme function. Medicine, Northwell Health from the SLE Immunochip study, and genotype and haplotype Feinstein Institutes for Medical frequencies were compared. DNASE1L3 protein levels were What does this study add? Research, Manhasset, New measured in cells and supernatants of HEK293 cells and York, USA ► The coding polymorphism rs35677470 is 2 monocyte-derived dendritic cells expressing recombinant and Department of Biostatistics the causal variant for the systemic lupus endogenous 206Arg and 206Cys protein variants. -
![Downloaded from [266]](https://docslib.b-cdn.net/cover/7352/downloaded-from-266-347352.webp)
Downloaded from [266]
Patterns of DNA methylation on the human X chromosome and use in analyzing X-chromosome inactivation by Allison Marie Cotton B.Sc., The University of Guelph, 2005 A THESIS SUBMITTED IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE OF DOCTOR OF PHILOSOPHY in The Faculty of Graduate Studies (Medical Genetics) THE UNIVERSITY OF BRITISH COLUMBIA (Vancouver) January 2012 © Allison Marie Cotton, 2012 Abstract The process of X-chromosome inactivation achieves dosage compensation between mammalian males and females. In females one X chromosome is transcriptionally silenced through a variety of epigenetic modifications including DNA methylation. Most X-linked genes are subject to X-chromosome inactivation and only expressed from the active X chromosome. On the inactive X chromosome, the CpG island promoters of genes subject to X-chromosome inactivation are methylated in their promoter regions, while genes which escape from X- chromosome inactivation have unmethylated CpG island promoters on both the active and inactive X chromosomes. The first objective of this thesis was to determine if the DNA methylation of CpG island promoters could be used to accurately predict X chromosome inactivation status. The second objective was to use DNA methylation to predict X-chromosome inactivation status in a variety of tissues. A comparison of blood, muscle, kidney and neural tissues revealed tissue-specific X-chromosome inactivation, in which 12% of genes escaped from X-chromosome inactivation in some, but not all, tissues. X-linked DNA methylation analysis of placental tissues predicted four times higher escape from X-chromosome inactivation than in any other tissue. Despite the hypomethylation of repetitive elements on both the X chromosome and the autosomes, no changes were detected in the frequency or intensity of placental Cot-1 holes. -

Differential Epigenomic and Transcriptomic Responses in Subcutaneous Adipose Tissue Between Low and High Responders to Caloric Restriction1–3
Differential epigenomic and transcriptomic responses in subcutaneous adipose tissue between low and high responders to caloric restriction1–3 Luigi Bouchard, Re´mi Rabasa-Lhoret, May Faraj, Marie-E`ve Lavoie, Jonathan Mill, Louis Pe´russe, and Marie-Claude Vohl ABSTRACT weight loss responses to caloric restriction show considerable Background: Caloric restriction is recommended for the treatment interindividual variability (7). Studies of genetically identical of obesity, but it is generally characterized by large interindividual monozygotic twins have been particularly useful in disentangling variability in responses. The factors affecting the magnitude of the role of environmental and heritable factors in determining the weight loss remain poorly understood. Epigenetic factors (ie, heri- degree of weight loss. It has been shown that within-pair changes table but reversible changes to genomic function that regulate gene in body fat variability after a caloric deficit is significantly lower expression independently of DNA sequence) may explain some of than between-pair variability, which suggests that genetic factors the interindividual variability seen in weight-loss responses. have an important influence on an individual’s response to caloric Objective: The objective was to determine whether epigenetics and deficit (8, 9). However, the concordance between twin pairs was gene expression changes may play a role in weight-loss responsiveness. not complete, which suggests that environmental factors or other Design: Overweight/obese postmenopausal women were recruited DNA sequence–independent mechanisms may be involved. for a standard 6-mo caloric restriction intervention. Abdominal sub- It has been suggested that monozygotic twin discordance for cutaneous adipose tissue biopsy samples were collected before (n = complex traits such as body weight could be accounted for by 14) and after (n = 14) intervention, and the epigenomic and tran- epigenetic factors (10, 11). -

De Novo Characterization of Cell-Free DNA Fragmentation Hotspots Boosts
bioRxiv preprint doi: https://doi.org/10.1101/2020.07.16.201350; this version posted July 16, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC 4.0 International license. 1 De novo characterization of cell-free DNA fragmentation hotspots 2 boosts the power for early detection and localization of multi- 3 cancer 4 Xionghui Zhou1, Yaping Liu1-4 * 5 1 Division of Human Genetics, Cincinnati Children’s Hospital Medical Center, Cincinnati, OH 6 45229 7 2 Division of Biomedical Informatics, Cincinnati Children’s Hospital Medical Center, 8 Cincinnati, OH 45229 9 3 Department of Pediatrics, University of Cincinnati College of Medicine, Cincinnati, OH 10 45229 11 4 Department of Electrical Engineering and Computing Sciences, University of Cincinnati 12 College of Engineering and Applied Science, Cincinnati, OH 45229 13 * Email: [email protected] 14 15 16 17 18 19 20 21 22 23 24 25 1 bioRxiv preprint doi: https://doi.org/10.1101/2020.07.16.201350; this version posted July 16, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC 4.0 International license. 26 Abstract 27 The global variation of cell-free DNA fragmentation patterns is a promising biomarker for 28 cancer diagnosis. However, the characterization of its hotspots and aberrations in early- 29 stage cancer at the fine-scale is still poorly understood. -
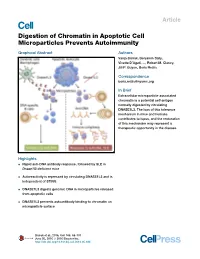
Digestion of Chromatin in Apoptotic Cell Microparticles Prevents Autoimmunity
Article Digestion of Chromatin in Apoptotic Cell Microparticles Prevents Autoimmunity Graphical Abstract Authors Vanja Sisirak, Benjamin Sally, Vivette D’Agati, ..., Robert M. Clancy, Jill P. Buyon, Boris Reizis Correspondence [email protected] In Brief Extracellular microparticle-associated chromatin is a potential self-antigen normally digested by circulating DNASE1L3. The loss of this tolerance mechanism in mice and humans contributes to lupus, and the restoration of this mechanism may represent a therapeutic opportunity in the disease. Highlights d Rapid anti-DNA antibody response, followed by SLE in Dnase1l3-deficient mice d Autoreactivity is repressed by circulating DNASE1L3 and is independent of STING d DNASE1L3 digests genomic DNA in microparticles released from apoptotic cells d DNASE1L3 prevents autoantibody binding to chromatin on microparticle surface Sisirak et al., 2016, Cell 166, 88–101 June 30, 2016 ª 2016 Elsevier Inc. http://dx.doi.org/10.1016/j.cell.2016.05.034 Article Digestion of Chromatin in Apoptotic Cell Microparticles Prevents Autoimmunity Vanja Sisirak,1,12 Benjamin Sally,1,2,12 Vivette D’Agati,3 Wilnelly Martinez-Ortiz,4 Z. Birsin O¨ zc¸ akar,5 Joseph David,1 Ali Rashidfarrokhi,1 Ada Yeste,6 Casandra Panea,2 Asiya Seema Chida,7 Milena Bogunovic,8 Ivaylo I. Ivanov,2 Francisco J. Quintana,6 Inaki Sanz,7 Keith B. Elkon,9 Mustafa Tekin,10 Fatosx Yalc¸ ınkaya,5 Timothy J. Cardozo,4 Robert M. Clancy,11 Jill P. Buyon,11 and Boris Reizis1,2,11,* 1Department of Pathology, New York University School of Medicine, New -
Identification of Novel Sleep Related Genes from Large Scale Phenotyping Experiments in Mice
University of Kentucky UKnowledge Theses and Dissertations--Biology Biology 2017 IDENTIFICATION OF NOVEL SLEEP RELATED GENES FROM LARGE SCALE PHENOTYPING EXPERIMENTS IN MICE Shreyas Joshi University of Kentucky, [email protected] Digital Object Identifier: https://doi.org/10.13023/ETD.2017.159 Right click to open a feedback form in a new tab to let us know how this document benefits ou.y Recommended Citation Joshi, Shreyas, "IDENTIFICATION OF NOVEL SLEEP RELATED GENES FROM LARGE SCALE PHENOTYPING EXPERIMENTS IN MICE" (2017). Theses and Dissertations--Biology. 42. https://uknowledge.uky.edu/biology_etds/42 This Doctoral Dissertation is brought to you for free and open access by the Biology at UKnowledge. It has been accepted for inclusion in Theses and Dissertations--Biology by an authorized administrator of UKnowledge. For more information, please contact [email protected]. STUDENT AGREEMENT: I represent that my thesis or dissertation and abstract are my original work. Proper attribution has been given to all outside sources. I understand that I am solely responsible for obtaining any needed copyright permissions. I have obtained needed written permission statement(s) from the owner(s) of each third-party copyrighted matter to be included in my work, allowing electronic distribution (if such use is not permitted by the fair use doctrine) which will be submitted to UKnowledge as Additional File. I hereby grant to The University of Kentucky and its agents the irrevocable, non-exclusive, and royalty-free license to archive and make accessible my work in whole or in part in all forms of media, now or hereafter known. -

Digestion of Chromatin in Apoptotic Cell
Digestion of Chromatin in Apoptotic Cell Microparticles Prevents Autoimmunity Vanja Sisirak, Benjamin Sally, Vivette d’Agati, Wilnelly Martinez-Ortiz, Z Birsin Özçakar, Joseph David, Ali Rashidfarrokhi, Ada Yeste, Casandra Panea, Asiya Chida, et al. To cite this version: Vanja Sisirak, Benjamin Sally, Vivette d’Agati, Wilnelly Martinez-Ortiz, Z Birsin Özçakar, et al.. Digestion of Chromatin in Apoptotic Cell Microparticles Prevents Autoimmunity. Cell, Elsevier, 2016, 166 (1), pp.88 - 101. 10.1016/j.cell.2016.05.034. hal-03045372 HAL Id: hal-03045372 https://hal.archives-ouvertes.fr/hal-03045372 Submitted on 27 Jan 2021 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. Digestion of Chromatin in Apoptotic Cell Microparticles Prevents Autoimmunity Vanja Sisirak1*, Benjamin Sally1,2*, Vivette D’Agati3, Wilnelly Martinez-Ortiz4, Z. Birsin Özçakar5, Joseph David1, Ali Rashidfarrokhi1, Ada Yeste6, Casandra Panea2, Asiya Seema Chida8, Milena Bogunovic7, Ivaylo I. Ivanov2, Francisco J. Quintana6, Inaki Sanz8, Keith B. Elkon9, Mustafa Tekin10, Fatoş Yalçınkaya5, Timothy J. Cardozo4, Robert M. Clancy11, Jill P. Buyon11 and Boris Reizis1,2,11 1Dept. of Pathology, New York University School of Medicine, New York, NY; 2Dept. of Microbiology and Immunology, Columbia University Medical Center, New York, NY; 3Dept. -

Literature Mining Sustains and Enhances Knowledge Discovery from Omic Studies
LITERATURE MINING SUSTAINS AND ENHANCES KNOWLEDGE DISCOVERY FROM OMIC STUDIES by Rick Matthew Jordan B.S. Biology, University of Pittsburgh, 1996 M.S. Molecular Biology/Biotechnology, East Carolina University, 2001 M.S. Biomedical Informatics, University of Pittsburgh, 2005 Submitted to the Graduate Faculty of School of Medicine in partial fulfillment of the requirements for the degree of Doctor of Philosophy University of Pittsburgh 2016 UNIVERSITY OF PITTSBURGH SCHOOL OF MEDICINE This dissertation was presented by Rick Matthew Jordan It was defended on December 2, 2015 and approved by Shyam Visweswaran, M.D., Ph.D., Associate Professor Rebecca Jacobson, M.D., M.S., Professor Songjian Lu, Ph.D., Assistant Professor Dissertation Advisor: Vanathi Gopalakrishnan, Ph.D., Associate Professor ii Copyright © by Rick Matthew Jordan 2016 iii LITERATURE MINING SUSTAINS AND ENHANCES KNOWLEDGE DISCOVERY FROM OMIC STUDIES Rick Matthew Jordan, M.S. University of Pittsburgh, 2016 Genomic, proteomic and other experimentally generated data from studies of biological systems aiming to discover disease biomarkers are currently analyzed without sufficient supporting evidence from the literature due to complexities associated with automated processing. Extracting prior knowledge about markers associated with biological sample types and disease states from the literature is tedious, and little research has been performed to understand how to use this knowledge to inform the generation of classification models from ‘omic’ data. Using pathway analysis methods to better understand the underlying biology of complex diseases such as breast and lung cancers is state-of-the-art. However, the problem of how to combine literature- mining evidence with pathway analysis evidence is an open problem in biomedical informatics research. -

Mckenna, Sim Et Al., Science, 2020
RESEARCH ◥ zation, we combined biochemical and structural RESEARCH ARTICLE SUMMARY approaches to define the function and mecha- nism of the P5A-ATPase. STRUCTURAL BIOLOGY RESULTS: P-type ATPases form a large class of The endoplasmic reticulum P5A-ATPase is a active transporters that are present in all kingdoms of life and predominantly trans- transmembrane helix dislocase port ions or lipids across cellular membranes. The P5A-ATPase belongs to a eukaryotic- Michael J. McKenna*, Sue Im Sim*, Alban Ordureau, Lianjie Wei, J. Wade Harper, specific subfamily of P-type ATPases with un- Sichen Shao†, Eunyong Park† known substrate specificity. We reconstituted membrane protein insertion into organelles in a cell-free system and used site-specific cross- INTRODUCTION: Eukaryotic cells contain geted transmembrane proteins from the ER linking to reveal that the P5A-ATPase interacts membrane-bound organelles with distinct membrane are incompletely understood. directly with the TM of a mitochondrial tail– identities and functionalities that depend anchored protein. Human cells lacking ATP13A1 on protein composition. Correct localization RATIONALE: As a model to study membrane pro- showed mislocalization of mitochondrial tail– of proteins is thus critical for organelle func- tein localization, we focused on tail–anchored anchored proteins to the ER and secretory tion and cellular homeostasis. The endoplas- proteins, which contain a single C-terminal TM pathway. In in vitro assays, newly synthesized mic reticulum (ER) and mitochondrial outer that is necessary and largely sufficient for or- mitochondrial tail–anchored proteins aber- Downloaded from membrane are the primary destinations for ganelle localization. We reasoned that factors rantly accumulated in ER vesicles lacking newly synthesized proteins with hydrophobic that mediate mitochondrial tail–anchored pro- P5A-ATPase activity.