Greater Severity of Clinical Features in Older Patients with Duane's Retraction Syndrome
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Official Scientific Journal of the Delhi Ophthalmologycal Society DJO Vol
DJO Vol.20, No. 2, October-December 09 DJO Vol.20, No. 2, October-December 09 October-December 2, No. Vol.20, DJO The Official Scientific Journal of the Delhi Ophthalmologycal Society DJO Vol. 20, No. 2, October-December, 2009 Delhi Journal of Ophthalmology Editor Editorial Board Rohit Saxena Rajvardhan Azad Ramanjit Sihota Managing Editor Vimla Menon Divender Sood Rajesh Sinha Atul Kumar Rishi Mohan Ashok K Grover Namrata Sharma Editorial Committee Mahipal S Sachdev Tanuj Dada Parijat Chandra M.Vanathi Lalit Verma Rajinder K hanna Tushar Agarwal Prakash Chand Agarwal Sharad Lakhotia Harbans Lal Chandrashekhar Kumar Swati Phuljhele P V Chaddha Amit Khosla Shibal Bhartiya Reena Sharma Dinesh Talwar B Ghosh Munish Dhawan Twinkle Parmar K.P.S Malik Kirti Singh Harinder Sethi Varun Gogia Pradeep Sharma B P Guliani Raghav Gupta Sashwat Ray V P Gupta S P Garg Ashish Kakkar Saptrishi Majumdar S. Bharti Arun Baweja General Information Delhi Journal of Ophthalmology (DJO), once called Visiscan, is a quarterly journal brought out by the Delhi Opthalmological Society. The journal aims at providing a platform to its readers for free exchange of ideas and information in accordance with the rules laid out for such publication. The DJO aims to become an easily readable referenced journal which will provide the specialists with up to date data and the residents with articles providing expert opinions supported with references. Contribution Methodology Delhi Journal of Opthalmology (DJO) is a quarterly journal. Author/Authors must have made significant contribution in carrying out the work and it should be original. It should be accompanied by a letter of transmittal. -

Duane Retraction Syndrome
Med. J. Cairo Univ., Vol. 78, No. 1, June: 331-336, 2010 www.medicaljournalofcairouniversity.com Duane Retraction Syndrome KARIMA L. SHALABY, M.D.* and MOSTAFA BAHGAT, M.D.** The Pediatric Ophthalmology Section*, Tripoli Eye Hospital and the Department of Ophthalmology**, Faculty of Medicine, Cairo University. Abstract Electromyography studies have shown paradox- ical innervations of Lateral rectus muscle and Purpose of Study: To evaluate and to manage if manage- anomalous synergistic innervations of medial rec- ment indicated for cases of Duane retraction syndrome. tus, inferior rectus, superior rectus and oblique Patients and Methods: 15 Duane retraction syndrome muscles [7,8] . (DRS) patients seen in Pediatric clinic in Tripoli Eye Hospital in period from January 2006-December 2006. Complete In most cases of DRS the entire 6 th nerve atro- ophthalmic examination including ortho-optic assessment for phy instead of post half of 6 th nerve (without all cases. specific teratogenic stimulus) 95% of DRS cases Results: Patients age ranged 1 year to 20 years in this this is the only initial abnormality. In about 5% of group of study, females were affected more than males with cases other abnormalities seen (e.g. nerve deafness). 2 to 1 ratio. Type 1 (esotropic) is the most common 80% of cases. Left eye was affected more than right eye. Bilateral in Most cases of DRS are sporadic [5,9] . 13.3% of cases. DRS clinical picture varies widely, surgical intervention will not eliminate the abnormality but will lessen Etiology: it. Two cases were operated upon to improve alignment in Etiology of DRS has been proposed by several primary position. -

Strabismus: a Decision Making Approach
Strabismus A Decision Making Approach Gunter K. von Noorden, M.D. Eugene M. Helveston, M.D. Strabismus: A Decision Making Approach Gunter K. von Noorden, M.D. Emeritus Professor of Ophthalmology and Pediatrics Baylor College of Medicine Houston, Texas Eugene M. Helveston, M.D. Emeritus Professor of Ophthalmology Indiana University School of Medicine Indianapolis, Indiana Published originally in English under the title: Strabismus: A Decision Making Approach. By Gunter K. von Noorden and Eugene M. Helveston Published in 1994 by Mosby-Year Book, Inc., St. Louis, MO Copyright held by Gunter K. von Noorden and Eugene M. Helveston All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, electronic, mechanical, photocopying, recording, or otherwise, without prior written permission from the authors. Copyright © 2010 Table of Contents Foreword Preface 1.01 Equipment for Examination of the Patient with Strabismus 1.02 History 1.03 Inspection of Patient 1.04 Sequence of Motility Examination 1.05 Does This Baby See? 1.06 Visual Acuity – Methods of Examination 1.07 Visual Acuity Testing in Infants 1.08 Primary versus Secondary Deviation 1.09 Evaluation of Monocular Movements – Ductions 1.10 Evaluation of Binocular Movements – Versions 1.11 Unilaterally Reduced Vision Associated with Orthotropia 1.12 Unilateral Decrease of Visual Acuity Associated with Heterotropia 1.13 Decentered Corneal Light Reflex 1.14 Strabismus – Generic Classification 1.15 Is Latent Strabismus -

Vertical Rectus Transposition in Duane&Rsquo
Eye (2015) 29, 839–842 & 2015 Macmillan Publishers Limited All rights reserved 0950-222X/15 www.nature.com/eye Sir, 5 Souza-Dias C. Congenital VI nerve palsy is Duane syndrome CORRESPONDENCE Vertical rectus transposition in Duane’s syndrome: does until disproven. Binocul Vis Strabismus Q 1992; 7:70. co-contraction worsen? 6 Sharma P, Tomar R, Menon V, Saxena R, Sharma A. Evaluation of periosteal fixation of lateral rectus and partial 1 We read with interest the article by Akar et al. We would VRT for cases of exotropic Duane’s retraction syndrome. like to make the following observations/queries. Indian J Ophthalmol 2014; 62: 204–208. In patients with Duane’s retraction syndrome there is some degree of subnormal and some degree of V Bhambhwani, PK Pandey, S Sood and K Rana anomalous innervation of the lateral rectus (LR) muscle. The extent and severity of the two may be variable. Guru Nanak Eye Centre and Maulana Azad Medical Presumably, subnormal innervation may lead to deficient College, New Delhi, India abduction and anomalous innervation may lead to E-mail: [email protected] co-contraction with globe retraction, palpebral aperture narrowing, or retraction equivalents like upshoots and Eye (2015) 29, 839; doi:10.1038/eye.2014.309; downshoots. published online 6 February 2015 In their article the authors describe patients of type 1 Duane syndrome to be with esotropia of 20 pd or more, an AHP larger than 201, limited abduction, and no significant upshoots or downshoots in the adducted Sir, position. There is no objective grading used for the Reply: Vertical rectus transposition in Duane’s measurement of shoots or palpebral aperture changes. -
Neurocranial Defects with Neuro-Ophthalmic Significance
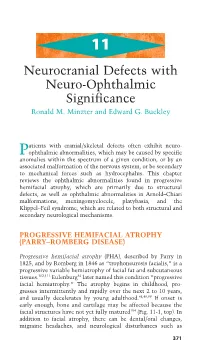
11 Neurocranial Defects with Neuro-Ophthalmic Significance Ronald M. Minzter and Edward G. Buckley atients with cranial/skeletal defects often exhibit neuro- Pophthalmic abnormalities, which may be caused by specific anomalies within the spectrum of a given condition, or by an associated malformation of the nervous system, or be secondary to mechanical forces such as hydrocephalus. This chapter reviews the ophthalmic abnormalities found in progressive hemifacial atrophy, which are primarily due to structural defects, as well as ophthalmic abnormalities in Arnold–Chiari malformations, meningomyelocele, platybasia, and the Klippel–Feil syndrome, which are related to both structural and secondary neurological mechanisms. PROGRESSIVE HEMIFACIAL ATROPHY (PARRY–ROMBERG DISEASE) Progressive hemifacial atrophy (PHA), described by Parry in 1825, and by Romberg in 1846 as “trophoneurosis facialis,” is a progressive variable hemiatrophy of facial fat and subcutaneous tissues.102,111 Eulenburg34 later named this condition “progressive facial hemiatrophy.” The atrophy begins in childhood, pro- gresses intermittently and rapidly over the next 2 to 10 years, and usually decelerates by young adulthood.48,49,99 If onset is early enough, bone and cartilage may be affected because the facial structures have not yet fully matured104 (Fig. 11-1, top). In addition to facial atrophy, there can be dental/oral changes, migraine headaches, and neurological disturbances such as 371 372 handbook of pediatric neuro-ophthalmology A B CD FIGURE 11-1A–D. Progressive nature of progressive hemifacial atrophy (PHA) in a patient at 8 years old (A) and again at 15 years (B), showing left-sided atrophy. Fundus photos of the normal contralateral side (C) and the ipsilateral affected side with hypopigmentary disturbances (D), par- ticularly along the inferior arcade. -

UCLA Previously Published Works
UCLA UCLA Previously Published Works Title The interplay of genetics and surgery in ophthalmic care. Permalink https://escholarship.org/uc/item/7nj489hp Journal Seminars in ophthalmology, 10(4) ISSN 0882-0538 Author Gorin, MB Publication Date 1995-12-01 DOI 10.3109/08820539509063801 Peer reviewed eScholarship.org Powered by the California Digital Library University of California Seminars in Ophthalmology ISSN: 0882-0538 (Print) 1744-5205 (Online) Journal homepage: http://www.tandfonline.com/loi/isio20 The Interplay of Genetics and Surgery in Ophthalmic Care Michael B. Gorin To cite this article: Michael B. Gorin (1995) The Interplay of Genetics and Surgery in Ophthalmic Care, Seminars in Ophthalmology, 10:4, 303-317, DOI: 10.3109/08820539509063801 To link to this article: http://dx.doi.org/10.3109/08820539509063801 Published online: 02 Jul 2009. Submit your article to this journal Article views: 9 View related articles Full Terms & Conditions of access and use can be found at http://www.tandfonline.com/action/journalInformation?journalCode=isio20 Download by: [UCLA Library] Date: 02 May 2017, At: 14:05 The Interplay of Genetics and Surgery in Ophthalmic Care Michael 6. Gorin LTHOUGH ONLY a minor component of dures. Genetic conditions that affect the eye A the surgical volume of ophthalmic care, directly may also affect the surgicaI outcomes of genetic disorders are among the most challeng- routine procedures. The coexistence of Fuch’s ing cases for the ophthalmic surgeon. Ophthal- endothelial dystrophy in patients undergoing mic surgery may be indicated to address specific routine cataract extraction can contribute to aspects of heritable disorders that involve the postoperative corneal edema. -

American Association for Pediatric Ophthalmology and Strabismus 45Th Annual Meeting, March 27-31, 2019, Preliminary Program, San Diego, CA
American Association for Pediatric Ophthalmology and Strabismus 45th Annual Meeting, March 27-31, 2019, Preliminary Program, San Diego, CA WEDNESDAY, MARCH 27, 2019 7:00 am – 2:30 pm Finance Committee, Board of Directors Meetings 12:00 pm – 8:00 pm Registration 1:00 pm – 4:00 pm Poster Set Up (1st Set) 4:00 pm – 6:00 pm Poster Viewing (1st Set) (Authors not present ) CME eligible 6:15 pm – 7:00 pm International Attendees Reception 7:00 pm – 9:00 pm Opening Reception THURSDAY, MARCH 28, 2019 6:30 am – 5:00 pm Registration 6:30 am – 8:00 am Breakfast 6:30 am – 7:30 am Poster Viewing (Authors not present) CME eligible 7:55 am – 8:00 am Introduction and Welcome Scott A. Larson, MD 8:00 am – 8:15 am AAPOS President’s Remarks, Honor Awards, Senior Honor Awards, Lifetime Achievement Awards R. Michael Siatkowski, MD 8:15 am – 8:20 am Introduction of Costenbader Lecturer Christie L. Morse, MD 8:20 am – 8:45 am Costenbader Lecture Supported by the Children’s Eye Foundation of AAPOS Making The Superior Oblique Great Again David A. Plager, MD 8:45 am – 8:48 am Presentation Ceremony M. Edward Wilson, Jr, MD CATARACT – GLAUCOMA – UVEITIS 8:50 am – 8:57 am Are Piggyback IOLs Recommendable for Children? M. Edward Wilson, Jr, MD 8:57 am – 9:04 am Outcomes of Bilateral Cataracts Removed in Infants 1 to 7 Months of Age Concurrent with the Infant Aphakia Treatment Study Erick D. Bothun, MD 9:04 am – 9:11 am Outcomes and Complications of Simultaneous Bilateral Cataract Surgery (SBCS) in Children – A 10 Year Review Vishaal Bhambhwani 9:11 am – 9:15 am DISCUSSION OF PREVIOUS PAPER David G. -

Non-Classical 1P36 Deletion in a Patient
Yokoyama et al. Mol Cytogenet (2020) 13:42 https://doi.org/10.1186/s13039-020-00510-5 CASE REPORT Open Access Non-classical 1p36 deletion in a patient with Duane retraction syndrome: case report and literature review Emiy Yokoyama1, Camilo E. Villarroel1, Sinhué Diaz2, Victoria Del Castillo1, Patricia Pérez‑Vera3, Consuelo Salas3, Samuel Gómez4, Reneé Barreda1, Bertha Molina5 and Sara Frias5,6* Abstract Background: Monosomy of 1p36 is considered the most common terminal microdeletion syndrome. It is character‑ ized by intellectual disability, growth retardation, seizures, congenital anomalies, and distinctive facial features that are absent when the deletion is proximal, beyond the 1p36.32 region. In patients with proximal deletions, little is known about the associated phenotype, since only a few cases have been reported in the literature. Ocular manifestations in patients with classical 1p36 monosomy are frequent and include strabismus, myopia, hypermetropia, and nystagmus. However, as of today only one patient with 1p36 deletion and Duane retraction syndrome (DRS) has been reported. Case presentation: We describe a patient with intellectual disability, facial dysmorphism, and bilateral Duane retrac‑ tion syndrome (DRS) type 1. Array CGH showed a 7.2 Mb de novo deletion from 1p36.31 to 1p36.21. Discussion: Our patient displayed DRS, which is not part of the classical phenotype and is not a common clinical feature in 1p36 deletion syndrome; we hypothesized that this could be associated with the overlapping deletion between the distal and proximal 1p36 regions. DRS is one of the Congenital Cranial Dysinnervation Disorders, and a genetic basis for the syndrome has been extensively reported. -

Duane Syndrome
Duane Syndrome Here are some strategies to help schools meet the needs of children with Duane Syndrome. The needs of children and young people with Duane Syndrome can be met through Quality First Teaching and simple strategies used in the classroom. In the majority of cases these children and young people do not require specialist interventions from a Qualified Teacher for Visual Impairment. The information in the universal section of the Mainstream Core Standards for VI will also be useful. What is Duane Syndrome? The movement of our eyes is controlled by three pairs of external muscles. In Duane syndrome some of them do not work as they should, as there appears to be a ‘mis-wiring’ of the nerves to the external eye muscles. Duane syndrome is present from birth. It does not get better nor does it get worse. It cannot be improved by surgery, although surgery does sometimes take place to deal with some aspects. Usually Duane syndrome affects just one eye, most often the left, although in some children it can affect both eyes. It is more commonly found in girls than in boys. Many children with Duane syndrome just have problems with their eye movements but it is important that they are checked to see if they have any other visual impairment as some can be associated with the syndrome. As with all children they may require glasses for long-sightedness, short-sightedness or astigmatism. They must also be checked for any hearing problems or developmental difficulties, as these too can sometimes be associated with Duane syndrome. -

Visual Disorders Associatedwith Cerebral Palsy
Br J Ophthalmol: first published as 10.1136/bjo.66.1.46 on 1 January 1982. Downloaded from British Journal ofOphthalmology, 1982, 66, 46-52 Visual disorders associated with cerebral palsy PETER BLACK From the Royal Air Force Hospital, Ely, Cambridgeshire SUMMARY School children severely afflicted with cerebral palsy, but unselected in regard to their visual status, have been studied. Of 120 children examined only 24 (20%) had normal eyes or ocular adnexae. Squint was found in 52*5% of the children and significant refractive errors in 50%. There was also a high incidence of strabismic and anisometropic amblyopia (15%) and visual field defects (11%). A number of other ocular abnormalities were found, the majority of which were not amenable to any form of treatment. Early identification of treatable ocular defects and their treatment along conventional lines is emphasised. It is also important to identify untreatable defects that may have a bearing on the child's education. These children need all the help available, and visual function should be at its best. A diagnosis of cerebral palsy has usually been made by the time such a child reaches 18 months of age. In view of the high incidence of ocular defects a full ophthalmological assessment should be part of the routine assessment of the child. Cerebral palsy consists of a group of conditions of and yet the latter still does not seem to merit the different aetiologies but with distinctive clinical attention that it deserves. These multiple manifes- features. The motor abnormalities dominate the tations have led to the terms 'brain damage clinical picture and form the basis for the definition of syndrome'2 or 'perinatal encephalopathy'3 being cerebral palsy that is most widely quoted in the British used, which perhaps are apter descriptions. -

Fuchs' Heterochromic Uveitis: a Reappraisal of the Clinical Spectrum
Eye (1991) S, 64 9-661 Fuchs' Heterochromic Uveitis: A Reappraisal of the Clinical Spectrum NICHOLAS P. JONES Manchester Summary The varying clinical appearance within a group of 103 patients with Fuchs' Hetero chromic Uveitis (FHU) is discussed. Bilateral cases accounted for 7.8% of patients. Cataract was found in 80.2% of cases after 8.8 years mean follow-up, and glaucoma affected 26.2% of patients. The most important diagnostic criteria are the typical pattern of iris atrophy and depigmentation, the characteristic intraocular inflam mation, and complicated cataract. These are described in detail. The correct diag nosis of FHU is important because it affects future management and prognosis. The presence or absence of macroscopic heterochromia is not a helpful component of the ocular examination and should play little part in diagnosis. FHU does not necessarily present in its classical form, and may first resemble acute anterior uveitis or pars planitis. The syndrome may be the end stage of a number of different conditions. Although the combination of heterochromia tis (FHU) has placed into perspective some of and cataract was noted in 1843 by Lawrence, I the accepted criteria for diagnosis, has and later by others2,3 it was not until 1906 that allowed further comment on some aspects of Ernst Fuchs comprehensively described a previous reports, and has brought to light group of 38 patients with signs of a form of some features not previously discussed in heterochromia with inflammation and catar detaiL The clinical spectrum of FHU is wider act, dubbed 'complicated heterochromia',4 than has been previously defined, and the The syndrome which now bears his name has clinical course is more variable, Studies on a interested many authors in the succeeding 85 cohort of 103 patients with FHU are reported. -

Ocular Manifestations of Inherited Diseases Maya Eibschitz-Tsimhoni
10 Ocular Manifestations of Inherited Diseases Maya Eibschitz-Tsimhoni ecognizing an ocular abnormality may be the first step in Ridentifying an inherited condition or syndrome. Identifying an inherited condition may corroborate a presumptive diagno- sis, guide subsequent management, provide valuable prognostic information for the patient, and determine if genetic counseling is needed. Syndromes with prominent ocular findings are listed in Table 10-1, along with their alternative names. By no means is this a complete listing. Two-hundred and thirty-five of approxi- mately 1900 syndromes associated with ocular or periocular manifestations (both inherited and noninherited) identified in the medical literature were chosen for this chapter. These syn- dromes were selected on the basis of their frequency, the char- acteristic or unique systemic or ocular findings present, as well as their recognition within the medical literature. The boldfaced terms are discussed further in Table 10-2. Table 10-2 provides a brief overview of the common ocular and systemic findings for these syndromes. The table is organ- ized alphabetically; the boldface name of a syndrome is followed by a common alternative name when appropriate. Next, the Online Mendelian Inheritance in Man (OMIM™) index num- ber is listed. By accessing the OMIM™ website maintained by the National Center for Biotechnology Information at http://www.ncbi.nlm.nih.gov, the reader can supplement the material in the chapter with the latest research available on that syndrome. A MIM number without a prefix means that the mode of inheritance has not been proven. The prefix (*) in front of a MIM number means that the phenotype determined by the gene at a given locus is separate from those represented by other 526 chapter 10: ocular manifestations of inherited diseases 527 asterisked entries and that the mode of inheritance of the phe- notype has been proven.