Embryology of the Nervous System
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Ultrasound Evaluation of the Central Nervous System
Ultrasound Evaluation of the Ultrasound Evaluation of the Central Nervous System Central Nervous System ••CNSCNS malformations are the second most Mani Montazemi, RDMS frequent category of congenital anomaly, Director of Ultrasound Education & Quality Assurancee after congenital heart disease Baylor College of Medicine Division of Maternal-Fetal Medicine ••PoorPoor timing of the examination, rather than Department of Obstetrics and Gynecology Texas Children’s Hospital, Pavilion for Women poor sensitivity, can be an important factor Houston Texas & in failing to detect a CNS abnormality Clinical Instructor Thomas Jefferson University Hospital Radiology Department Fetal Head Philadelphia, Pennsylvania Fetal Head Central Nervous System Brain Development 9 -13 weeks Rhombencephalon 5th Menstrual Week •Gives rise to hindbrain •4th ventricle Arises from the posterior surface of the embryonic ectoderm Mesencephalon •Gives rise to midbrain A small groove is found along •Aqueduct the midline of the embryo and the edges of this groove fold over to form a neuro tube that Prosencephalon gives rise to the fetal spinal •Gives rise to forebrain rd cord and brain •Lateral & 3 ventricles Fetal Head Fetal Head Ventricular view Neural Tube Defects ••LateralLateral ventricles ••ChoroidChoroid plexus Group of malformations: Thalamic view • Anencephaly ••MidlineMidline falx •Anencephaly ••CavumCavum septiseptipellucidi pellucidi ••CephalocelesCephaloceles ••ThalamiThalami ••SpinaSpina bifida Cerebellar view ••CerebellumCerebellum ••CisternaCisterna magna Fetal -
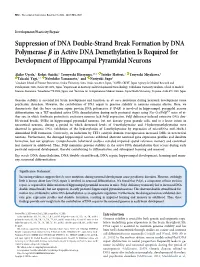
Suppression of DNA Double-Strand Break Formation by DNA Polymerase B in Active DNA Demethylation Is Required for Development of Hippocampal Pyramidal Neurons
9012 • The Journal of Neuroscience, November 18, 2020 • 40(47):9012–9027 Development/Plasticity/Repair Suppression of DNA Double-Strand Break Formation by DNA Polymerase b in Active DNA Demethylation Is Required for Development of Hippocampal Pyramidal Neurons Akiko Uyeda,1 Kohei Onishi,1 Teruyoshi Hirayama,1,2,3 Satoko Hattori,4 Tsuyoshi Miyakawa,4 Takeshi Yagi,1,2 Nobuhiko Yamamoto,1 and Noriyuki Sugo1 1Graduate School of Frontier Biosciences, Osaka University, Suita, Osaka 565-0871, Japan, 2AMED-CREST, Japan Agency for Medical Research and Development, Suita, Osaka 565-0871, Japan, 3Department of Anatomy and Developmental Neurobiology, Tokushima University Graduate School of Medical Sciences, Kuramoto, Tokushima 770-8503, Japan, and 4Institute for Comprehensive Medical Science, Fujita Health University, Toyoake, Aichi 470-1192, Japan Genome stability is essential for brain development and function, as de novo mutations during neuronal development cause psychiatric disorders. However, the contribution of DNA repair to genome stability in neurons remains elusive. Here, we demonstrate that the base excision repair protein DNA polymerase b (Polb) is involved in hippocampal pyramidal neuron fl/fl differentiation via a TET-mediated active DNA demethylation during early postnatal stages using Nex-Cre/Polb mice of ei- ther sex, in which forebrain postmitotic excitatory neurons lack Polb expression. Polb deficiency induced extensive DNA dou- ble-strand breaks (DSBs) in hippocampal pyramidal neurons, but not dentate gyrus granule cells, and to a lesser extent in neocortical neurons, during a period in which decreased levels of 5-methylcytosine and 5-hydroxymethylcytosine were observed in genomic DNA. Inhibition of the hydroxylation of 5-methylcytosine by expression of microRNAs miR-29a/b-1 diminished DSB formation. -

Bhagwan Moorjani, MD, FAAP, FAAN • Requires Knowledge of Normal CNS Developmental (I.E
1/16/2012 Neuroimaging in Childhood • Neuroimaging issues are distinct from Pediatric Neuroimaging in adults Neurometabolic-degenerative disorder • Sedation/anesthesia and Epilepsy • Motion artifacts Bhagwan Moorjani, MD, FAAP, FAAN • Requires knowledge of normal CNS developmental (i.e. myelin maturation) • Contrast media • Parental anxiety Diagnostic Approach Neuroimaging in Epilepsy • Age of onset • Peak incidence in childhood • Static vs Progressive • Occurs as a co-morbid condition in many – Look for treatable causes pediatric disorders (birth injury, – Do not overlook abuse, Manchausen if all is negative dysmorphism, chromosomal anomalies, • Phenotype presence (syndromic, HC, NCS, developmental delays/regression) systemic involvement) • Predominant symptom (epilepsy, DD, • Many neurologic disorders in children weakness/motor, psychomotor regression, have the same chief complaint cognitive/dementia) 1 1/16/2012 Congenital Malformation • Characterized by their anatomic features • Broad categories: based on embryogenesis – Stage 1: Dorsal Induction: Formation and closure of the neural tube. (Weeks 3-4) – Stage 2: Ventral Induction: Formation of the brain segments and face. (Weeks 5-10) – Stage 3: Migration and Histogenesis: (Months 2-5) – Stage 4: Myelination: (5-15 months; matures by 3 years) Dandy Walker Malformation Dandy walker • Criteria: – high position of tentorium – dysgenesis/agenesis of vermis – cystic dilatation of fourth ventricle • commonly associated features: – hypoplasia of cerebellum – scalloping of inner table of occipital bone • associated abnormalities: – hydrocephalus 75% – dysgenesis of corpus callosum 25% – heterotropia 10% 2 1/16/2012 Etiology of Epilepsy: Developmental and Genetic Classification of Gray Matter Heterotropia Cortical Dysplasia 1. Secondary to abnormal neuronal and • displaced masses of nerve cells • Subependymal glial proliferation/apoptosis (gray matter) heterotropia (most • most common: small nest common) 2. -

A Anencephaly
Glossary of Birth Anomaly Terms: A Anencephaly: A deadly birth anomaly where most of the brain and skull did not form. Anomaly: Any part of the body or chromosomes that has an unusual or irregular structure. Aortic valve stenosis: The aortic valve controls the flow of blood from the left ventricle of the heart to the aorta, which takes the blood to the rest of the body. If there is stenosis of this valve, the valve has space for blood to flow through, but it is too narrow. Atresia: Lack of an opening where there should be one. Atrial septal defect: An opening in the wall (septum) that separates the left and right top chambers (atria) of the heart. A hole can vary in size and may close on its own or may require surgery. Atrioventricular septal defect (endocardial cushion defect): A defect in both the lower portion of the atrial septum and the upper portion of the ventricular septum. Together, these defects make a large opening (canal) in the middle part of the heart. Aniridia (an-i-rid-e-a): An eye anomaly where the colored part of the eye (called the iris) is partly or totally missing. It usually affects both eyes. Other parts of the eye can also be formed incorrectly. The effects on children’s ability to see can range from mild problems to blindness. To learn more about aniridia, go to the U.S. National Library of Medicine website. Anophthalmia/microphthalmia (an-oph-thal-mia/mi-croph-thal-mia): Birth anomalies of the eyes. In anophthalmia, a baby is born without one or both eyes. -

The Genetic Basis of Mammalian Neurulation
REVIEWS THE GENETIC BASIS OF MAMMALIAN NEURULATION Andrew J. Copp*, Nicholas D. E. Greene* and Jennifer N. Murdoch‡ More than 80 mutant mouse genes disrupt neurulation and allow an in-depth analysis of the underlying developmental mechanisms. Although many of the genetic mutants have been studied in only rudimentary detail, several molecular pathways can already be identified as crucial for normal neurulation. These include the planar cell-polarity pathway, which is required for the initiation of neural tube closure, and the sonic hedgehog signalling pathway that regulates neural plate bending. Mutant mice also offer an opportunity to unravel the mechanisms by which folic acid prevents neural tube defects, and to develop new therapies for folate-resistant defects. 6 ECTODERM Neurulation is a fundamental event of embryogenesis distinct locations in the brain and spinal cord .By The outer of the three that culminates in the formation of the neural tube, contrast, the mechanisms that underlie the forma- embryonic (germ) layers that which is the precursor of the brain and spinal cord. A tion, elevation and fusion of the neural folds have gives rise to the entire central region of specialized dorsal ECTODERM, the neural plate, remained elusive. nervous system, plus other organs and embryonic develops bilateral neural folds at its junction with sur- An opportunity has now arisen for an incisive analy- structures. face (non-neural) ectoderm. These folds elevate, come sis of neurulation mechanisms using the growing battery into contact (appose) in the midline and fuse to create of genetically targeted and other mutant mouse strains NEURAL CREST the neural tube, which, thereafter, becomes covered by in which NTDs form part of the mutant phenotype7.At A migratory cell population that future epidermal ectoderm. -

Clonal Dispersion During Neural Tube Formation 4097 of Neuromeres
Development 126, 4095-4106 (1999) 4095 Printed in Great Britain © The Company of Biologists Limited 1999 DEV2458 Successive patterns of clonal cell dispersion in relation to neuromeric subdivision in the mouse neuroepithelium Luc Mathis1,*, Johan Sieur1, Octavian Voiculescu2, Patrick Charnay2 and Jean-François Nicolas1,‡ 1Unité de Biologie moléculaire du Développement, Institut Pasteur, 25, rue du Docteur Roux, 75724 Paris Cedex 15, France 2Unité INSERM 368, Ecole Normale Supérieure, 46 rue d’Ulm, 75230 Paris Cedex 05, France *Present address: Beckman Institute (139-74), California Institute of Technology, Pasadena, CA, 91125, USA ‡Author for correspondence (e-mail: [email protected]) Accepted 5 July; published on WWW 23 August 1999 SUMMARY We made use of the laacz procedure of single-cell labelling the AP and DV axis of the neural tube. A similar sequence to visualize clones labelled before neuromere formation, in of AP cell dispersion followed by an arrest of AP cell 12.5-day mouse embryos. This allowed us to deduce two dispersion, a preferential DV cell dispersion and then by a successive phases of cell dispersion in the formation of the coherent neuroepithelial growth, is also observed in the rhombencephalon: an initial anterior-posterior (AP) cell spinal cord and mesencephalon. This demonstrates that a dispersion, followed by an asymmetrical dorsoventral (DV) similar cascade of cell events occurs in these different cell distribution during which AP cell dispersion occurs in domains of the CNS. In the prosencephalon, differences in territories smaller than one rhombomere. We conclude that spatial constraints may explain the variability in the the general arrest of AP cell dispersion precedes the onset orientation of cell clusters. -

Optic Nerve Hypoplasia Plus: a New Way of Looking at Septo-Optic Dysplasia
Optic Nerve Hypoplasia Plus: A New Way of Looking at Septo-Optic Dysplasia Item Type text; Electronic Thesis Authors Mohan, Prithvi Mrinalini Publisher The University of Arizona. Rights Copyright © is held by the author. Digital access to this material is made possible by the University Libraries, University of Arizona. Further transmission, reproduction or presentation (such as public display or performance) of protected items is prohibited except with permission of the author. Download date 29/09/2021 22:50:06 Item License http://rightsstatements.org/vocab/InC/1.0/ Link to Item http://hdl.handle.net/10150/625105 OPTIC NERVE HYPOPLASIA PLUS: A NEW WAY OF LOOKING AT SEPTO-OPTIC DYSPLASIA By PRITHVI MRINALINI MOHAN ____________________ A Thesis Submitted to The Honors College In Partial Fulfillment of the Bachelors degree With Honors in Physiology THE UNIVERSITY OF ARIZONA M A Y 2 0 1 7 Approved by: ____________________________ Dr. Vinodh Narayanan Center for Rare Childhood Disorders Abstract Septo-optic dysplasia (SOD) is a rare congenital disorder that affects 1/10,000 live births. At its core, SOD is a disorder resulting from improper embryological development of mid-line brain structures. To date, there is no comprehensive understanding of the etiology of SOD. Currently, SOD is diagnosed based on the presence of at least two of the following three factors: (i) optic nerve hypoplasia (ii) improper pituitary gland development and endocrine dysfunction and (iii) mid-line brain defects, including agenesis of the septum pellucidum and/or corpus callosum. A literature review of existing research on the disorder was conducted. The medical history and genetic data of 6 patients diagnosed with SOD were reviewed to find damaging variants. -

Pushing the Limits of Prenatal Ultrasound: a Case of Dorsal Dermal Sinus Associated with an Overt Arnold–Chiari Malformation and a 3Q Duplication
reproductive medicine Case Report Pushing the Limits of Prenatal Ultrasound: A Case of Dorsal Dermal Sinus Associated with an Overt Arnold–Chiari Malformation and a 3q Duplication Olivier Leroij 1, Lennart Van der Veeken 2,*, Bettina Blaumeiser 3 and Katrien Janssens 3 1 Faculty of Medicine, University of Antwerp, 2610 Wilrijk, Belgium; [email protected] 2 Department of Obstetrics and Gynaecology, University Hospital Antwerp, 2650 Edegem, Belgium 3 Department of Medical Genetics, University Hospital and University of Antwerp, 2650 Edegem, Belgium; [email protected] (B.B.); [email protected] (K.J.) * Correspondence: [email protected] Abstract: We present a case of a fetus with cranial abnormalities typical of open spina bifida but with an intact spine shown on both ultrasound and fetal MRI. Expert ultrasound examination revealed a very small tract between the spine and the skin, and a postmortem examination confirmed the diagnosis of a dorsal dermal sinus. Genetic analysis found a mosaic 3q23q27 duplication in the form of a marker chromosome. This case emphasizes that meticulous prenatal ultrasound examination has the potential to diagnose even closed subtypes of neural tube defects. Furthermore, with cerebral anomalies suggesting a spina bifida, other imaging techniques together with genetic tests and measurement of alpha-fetoprotein in the amniotic fluid should be performed. Citation: Leroij, O.; Van der Veeken, Keywords: dorsal dermal sinus; Arnold–Chiari anomaly; 3q23q27 duplication; mosaic; marker chro- L.; Blaumeiser, B.; Janssens, K. mosome Pushing the Limits of Prenatal Ultrasound: A Case of Dorsal Dermal Sinus Associated with an Overt Arnold–Chiari Malformation and a 3q 1. -

Polymicrogyria (PMG) ‘Many–Small–Folds’
Polymicrogyria Dr Andrew Fry Clinical Senior Lecturer in Medical Genetics Institute of Medical Genetics, Cardiff [email protected] Polymicrogyria (PMG) ‘Many–small–folds’ • PMG is heterogeneous – in aetiology and phenotype • A disorder of post-migrational cortical organisation. PMG often appears thick on MRI with blurring of the grey-white matter boundary Normal PMG On MRI PMG looks thick but the cortex is actually thin – with folded, fused gyri Courtesy of Dr Jeff Golden, Pen State Unv, Philadelphia PMG is often confused with pachygyria (lissencephaly) Thick cortex (10 – 20mm) Axial MRI 4 cortical layers Lissencephaly Polymicrogyria Cerebrum Classical lissencephaly is due Many small gyri – often to under-migration. fused together. Axial MRI image at 7T showing morphological aspects of PMG. Guerrini & Dobyns Malformations of cortical development: clinical features and genetic causes. Lancet Neurol. 2014 Jul; 13(7): 710–726. PMG - aetiology Pregnancy history • Intrauterine hypoxic/ischemic brain injury (e.g. death of twin) • Intrauterine infection (e.g. CMV, Zika virus) TORCH, CMV PCR, [+deafness & cerebral calcification] CT scan • Metabolic (e.g. Zellweger syndrome, glycine encephalopathy) VLCFA, metabolic Ix • Genetic: Family history Familial recurrence (XL, AD, AR) Chromosomal abnormalities (e.g. 1p36 del, 22q11.2 del) Syndromic (e.g. Aicardi syndrome, Kabuki syndrome) Examin - Monogenic (e.g. TUBB2B, TUBA1A, GPR56) Array ation CGH Gene test/Panel/WES/WGS A cohort of 121 PMG patients Aim: To explore the natural history of PMG and identify new genes. Recruited: • 99 unrelated patients • 22 patients from 10 families 87% White British, 53% male ~92% sporadic cases (NB. ascertainment bias) Sporadic PMG • Array CGH, single gene and gene panel testing - then a subset (n=57) had trio-WES. -

Reportable BD Tables Apr2019.Pdf
April 2019 Georgia Department of Public Health | Division of Health Protection | Maternal and Child Health Epidemiology Unit Reportable Birth Defects with ICD-10-CM Codes Reportable Birth Defects in Georgia with ICD-10-CM Diagnosis Codes Table D.1 Brain Malformations and Neural Tube Defects ICD-10-CM Diagnosis Codes Birth Defect ICD-10-CM 1. Brain Malformations and Neural Tube Defects Q00-Q05, Q07 Anencephaly Q00.0 Craniorachischisis Q00.1 Iniencephaly Q00.2 Frontal encephalocele Q01.0 Nasofrontal encephalocele Q01.1 Occipital encephalocele Q01.2 Encephalocele of other sites Q01.8 Encephalocele, unspecified Q01.9 Microcephaly Q02 Malformations of aqueduct of Sylvius Q03.0 Atresia of foramina of Magendie and Luschka (including Dandy-Walker) Q03.1 Other congenital hydrocephalus (including obstructive hydrocephaly) Q03.8 Congenital hydrocephalus, unspecified Q03.9 Congenital malformations of corpus callosum Q04.0 Arhinencephaly Q04.1 Holoprosencephaly Q04.2 Other reduction deformities of brain Q04.3 Septo-optic dysplasia of brain Q04.4 Congenital cerebral cyst (porencephaly, schizencephaly) Q04.6 Other specified congenital malformations of brain (including ventriculomegaly) Q04.8 Congenital malformation of brain, unspecified Q04.9 Cervical spina bifida with hydrocephalus Q05.0 Thoracic spina bifida with hydrocephalus Q05.1 Lumbar spina bifida with hydrocephalus Q05.2 Sacral spina bifida with hydrocephalus Q05.3 Unspecified spina bifida with hydrocephalus Q05.4 Cervical spina bifida without hydrocephalus Q05.5 Thoracic spina bifida without -

CONGENITAL ABNORMALITIES of the CENTRAL NERVOUS SYSTEM Christopher Verity, Helen Firth, Charles Ffrench-Constant *I3
J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.74.suppl_1.i3 on 1 March 2003. Downloaded from CONGENITAL ABNORMALITIES OF THE CENTRAL NERVOUS SYSTEM Christopher Verity, Helen Firth, Charles ffrench-Constant *i3 J Neurol Neurosurg Psychiatry 2003;74(Suppl I):i3–i8 dvances in genetics and molecular biology have led to a better understanding of the control of central nervous system (CNS) development. It is possible to classify CNS abnormalities Aaccording to the developmental stages at which they occur, as is shown below. The careful assessment of patients with these abnormalities is important in order to provide an accurate prog- nosis and genetic counselling. c NORMAL DEVELOPMENT OF THE CNS Before we review the various abnormalities that can affect the CNS, a brief overview of the normal development of the CNS is appropriate. c Induction—After development of the three cell layers of the early embryo (ectoderm, mesoderm, and endoderm), the underlying mesoderm (the “inducer”) sends signals to a region of the ecto- derm (the “induced tissue”), instructing it to develop into neural tissue. c Neural tube formation—The neural ectoderm folds to form a tube, which runs for most of the length of the embryo. c Regionalisation and specification—Specification of different regions and individual cells within the neural tube occurs in both the rostral/caudal and dorsal/ventral axis. The three basic regions of copyright. the CNS (forebrain, midbrain, and hindbrain) develop at the rostral end of the tube, with the spinal cord more caudally. Within the developing spinal cord specification of the different popu- lations of neural precursors (neural crest, sensory neurones, interneurones, glial cells, and motor neurones) is observed in progressively more ventral locations. -
NERVOUS SYSTEM هذا الملف لالستزادة واثراء المعلومات Neuropsychiatry Block
NERVOUS SYSTEM هذا الملف لﻻستزادة واثراء المعلومات Neuropsychiatry block. قال تعالى: ) َو َل َق د َخ َل قنَا ا ِْلن َسا َن ِمن ُس ََل َل ة ِ من ِطي ن }12{ ثُ م َجعَ لنَاه ُ نُ ط َفة فِي َق َرا ر م ِكي ن }13{ ثُ م َخ َل قنَا ال ُّن ط َفة َ َع َل َقة َف َخ َل قنَا ا لعَ َل َقة َ ُم ضغَة َف َخ َل قنَا ا ل ُم ضغَة َ ِع َظا ما َف َك َس ونَا ا ل ِع َظا َم َل ح ما ثُ م أَن َشأنَاه ُ َخ ل قا آ َخ َر َفتَبَا َر َك ّللا ُ أَ ح َس ُن ا ل َخا ِل ِقي َن }14{( Resources BRS Embryology Book. Pathoma Book ( IN DEVELOPMENTAL ANOMALIES PART ). [email protected] 1 OVERVIEW A- Central nervous system (CNS) is formed in week 3 of development, during which time the neural plate develops. The neural plate, consisting of neuroectoderm, becomes the neural tube, which gives rise to the brain and spinal cord. B- Peripheral nervous system (PNS) is derived from three sources: 1. Neural crest cells 2. Neural tube, which gives rise to all preganglionic autonomic nerves (sympathetic and parasympathetic) and all nerves (-motoneurons and -motoneurons) that innervate skeletal muscles 3. Mesoderm, which gives rise to the dura mater and to connective tissue investments of peripheral nerve fibers (endoneurium, perineurium, and epineurium) DEVELOPMENT OF THE NEURAL TUBE Neurulation refers to the formation and closure of the neural tube. BMP-4 (bone morphogenetic protein), noggin (an inductor protein), chordin (an inductor protein), FGF-8 (fibroblast growth factor), and N-CAM (neural cell adhesion molecule) appear to play a role in neurulation.