Uva-DARE (Digital Academic Repository)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

DJ – Titres Incontournables
DJ – Titres incontournables Ce listing de titres constamment réactualisé , il vous ait destiné afin de surligner avec un code couleur ce que vous préférez afin de vous garantir une personnalisation totale de votre soirée . Si vous le souhaitez , il vaut mieux nous appeler pour vous envoyer sur votre mail la version la plus récente . Vous pouvez aussi rajouter des choses qui n’apparaissent pas et nous nous chargeons de trouver cela pour vous . Des que cette inventaire est achevé par vos soins , nous renvoyer par mail ce fichier adapté à vos souhaits 2018 bruno mars – finesse dj-snake-magenta-riddim-audio ed-sheeran-perfect-official-music-video liam-payne-rita-ora-for-you-fifty-shades-freed luis-fonsi-demi-lovato-echame-la-culpa ofenbach-vs-nick-waterhouse-katchi-official-video vitaa-un-peu-de-reve-en-duo-avec-claudio-capeo-clip-officiel 2017 amir-on-dirait april-ivy-be-ok arigato-massai-dont-let-go-feat-tessa-b- basic-tape-so-good-feat-danny-shah bastille-good-grief bastille-things-we-lost-in-the-fire bigflo-oli-demain-nouveau-son-alors-alors bormin-feat-chelsea-perkins-night-and-day burak-yeter-tuesday-ft-danelle-sandoval calum-scott-dancing-on-my-own-1-mic-1-take celine-dion-encore-un-soir charlie-puth-attention charlie-puth-we-dont-talk-anymore-feat-selena-gomez clean-bandit-rockabye-ft-sean-paul-anne-marie dj-khaled-im-the-one-ft-justin-bieber-quavo-chance-the-rapper-lil-wayne dj-snake-let-me-love-you-ft-justin-bieber enrique-iglesias-subeme-la-radio-remix-remixlyric-video-ft-cnco feder-feat-alex-aiono-lordly give-you-up-feat-klp-crayon -

Дмитрий (Rodrigez) Тел Моб. – +7-918-77777-80 Тел Моб
1 СПИСОК МУЗЫКАЛЬНЫХ КОМПОЗИЦИЙ 1 ТАНЦЕВАЛЬНЫЕ ХИТЫ–50/50 2 РОССИЙСКАЯ ЭСТРАДА 3 РУССКИЕ НАРОДНЫЕ 4 СОВЕТСКАЯ ЭСТРАДА 5 РОССИЙСКИЕ МЕДЛЕННЫЕ 6 GOLDEN-DISCO 7 RЕMIX 8 ЗАРУБЕЖНАЯ ЭСТРАДА 9 КЛУБНАЯ МУЗЫКА 10 HEAVY METAL 11 HIP-HOP 12 LATIN HOUSE 13 LATINOS 14 ROMANTIC 15 TARANTINO 16 ВАЛЬСЫ 17 ВЕРКА СЕРДЮЧКА 18 ДЕТСКИЕ 19 ДЖАЗ 20 ИНСТРУМЕНТАЛ 21 КАНТРИ 22 МУЗЫКА ИЗ КИНО 23 КЛАССИКА 24 МАРШИ 25 МИНУСОВКИ 26 МОДНО 27 НОВЫЙ ГОД 28 НАЦИОНАЛЬНЫЕ 29 ПЕСНИ О ПРОФЕССИЯХ 30 ПЕСНИ О ВОЙНЕ 31 ПЕСНИ О СТАВРОПОЛЕ 32 РЕТРО 33 РЕГГИ 34 РЕТРО-80-Х-90-Х 35 РОК-Н-РОЛЛ 36 РОМАНСЫ 37 СПОРТ 38 ТАНГО 39 ТАНЦЫ-90-Х 40 ШАНСОН 41 ШКОЛЬНЫЕ ПЕСНИ Дмитрий (Rodrigez) Тел моб. – +7-918-77777-80 Тел моб. - 690-777 Музыкальное и световое E-mail: [email protected] оформление Вашего торжества 2 1. ТАНЦЕВАЛЬНЫЕ ХИТЫ – 50/50 2. 23-45 - & 5 IVESTA FAMILY - Я БУДУ 3. AKCENT - ON AND ON 4. ANTOINE MONTANA - PALQUE 5. ARASH - PURE LOVE FEAT HELENA 6. ARASH - PURE LOVE FEAT HELENA 7. АRMIN VAN BUUREN FEAT SHARON DEN ADEL - IN & OUT OF LOVE 8. AYSEL & ARASH - ALWAYS (RADIO MIX) 9. BASIC ELEMENT - TOUCH YOU RIGHT NOW 10. BOB SINCLAR - GIVE ME SOME MORE 11. BOB SINCLAR - LA LA SONG (TOCADISCO REMIX 12. BRITNEY SPEARS - CIRCUS 13. BRITNEY SPEARS - RADAR 14. BIG ALI FT DOLLARMAN - HIT THE FLOOR ---SNAP 15. C&C MUSIC FACTORY & KULCHA DON - WORK THAT BODY 16. CENTR - ГОРОД 17. CHRISTINA AGUILERA - KEEPS GETTIN BETTER 18. CRAIG DAVID - INSOMNIA 19. DA GROOVE DOCTORS - ALL WE NEED IS LOVE 20. -
Forced Back to Danger Asylum-Seekers Returned from Europe to Afghanistan
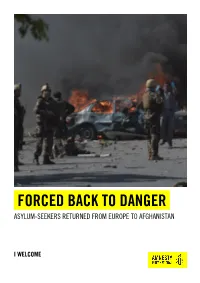
FORCED BACK TO DANGER ASYLUM-SEEKERS RETURNED FROM EUROPE TO AFGHANISTAN I WELCOME Amnesty International is a global movement of more than 7 million people who campaign for a world where human rights are enjoyed by all. Our vision is for every person to enjoy all the rights enshrined in the Universal Declaration of Human Rights and other international human rights standards. We are independent of any government, political ideology, economic interest or religion and are funded mainly by our membership and public donations. © Amnesty International 2017 Except where otherwise noted, content in this document is licensed under a Creative Commons Cover photo: Afghan security forces personnel are seen at the site of a truck bomb attack in Kabul on 31 (attribution, non-commercial, no derivatives, international 4.0) licence. May 2017. At least 150 people were killed and hundreds injured as a massive blast ripped through https://creativecommons.org/licenses/by-nc-nd/4.0/legalcode Kabul's diplomatic quarter, shattering the morning rush hour and bringing carnage to the streets of the For more information please visit the permissions page on our website: www.amnesty.org Afghan capital. © Shah Marai/AFP/Getty Images Where material is attributed to a copyright owner other than Amnesty International this material is not subject to the Creative Commons licence. First published in 2017 by Amnesty International Ltd Peter Benenson House, 1 Easton Street London WC1X 0DW, UK Index: ASA 11/6866/2017 Original language: English amnesty.org EMBARGOED UNTIL 5 OCTOBER 2017 CONTENTS GLOSSARY 4 EXECUTIVE SUMMARY 6 METHODOLOGY 11 1. FORCED BACK: STORIES FROM AFGHANISTAN 12 2. -

Classement Des 200 Premiers Singles Fusionnés Par Gfk Année 2012
Classement des 200 premiers Singles Fusionnés par GfK année 2012 Rang Artiste Titre Label Editeur Distributeur Physique Distributeur Numérique Genre 1 MICHEL TELO AI SE EU TE PEGO ULM MERCURY MUSIC GROUP UNIVERSAL MUSIC FRANCE UNIVERSAL MUSIC DIVISION MERCURY VARIETE INTERNATIONALE 2 GOTYE SOMEBODY THAT I USED TO KNOW CASABLANCA MERCURY MUSIC GROUP UNIVERSAL MUSIC FRANCE UNIVERSAL MUSIC DIVISION MERCURY POP ROCK 3 CARLY RAE JEPSEN CALL ME MAYBE INTERSCOPE RECORDS POLYDOR UNIVERSAL MUSIC FRANCE UNIVERSAL MUSIC DIVISION POLYDOR VARIETE INTERNATIONALE 4 PSY GANGNAM STYLE ULM MERCURY MUSIC GROUP UNIVERSAL MUSIC FRANCE UNIVERSAL MUSIC DIVISION MERCURY VARIETE INTERNATIONALE 5 ADELE SKYFALL Beggars Naïve NAIVE BEGGARD GROUP / XL RECORDING INDE 6 LYKKE LI I FOLLOW RIVERS WEA WEA WARNER MUSIC FRANCE WARNER MUSIC FRANCE VARIETE INTERNATIONALE 7 LANA DEL REY VIDEO GAMES POLYDOR POLYDOR UNIVERSAL MUSIC FRANCE UNIVERSAL MUSIC DIVISION POLYDOR VARIETE INTERNATIONALE 8 SHAKIRA JE LAIME A MOURIR Norte JIVE EPIC GROUP SONY MUSIC ENTERTAINMENT SONY MUSIC JIVE EPIC GROUP VARIETE INTERNATIONALE 9 SEXION D ASSAUT AVANT QU ELLE PARTE Jive Epic JIVE EPIC GROUP SONY MUSIC ENTERTAINMENT SONY MUSIC JIVE EPIC GROUP VARIETE FRANCAISE 10 RIHANNA DIAMONDS DEF JAM FRANCE Def Jam Recordings France UNIVERSAL MUSIC FRANCE UNIVERSAL MUSIC DIVISION DEF JAM VARIETE INTERNATIONALE 11 ASAF AVIDAN THE MOJOS ONE DAY RECKONING SONG Columbia Deutschland JIVE EPIC GROUP SONY MUSIC ENTERTAINMENT SONY MUSIC COLUMBIA GROUP VARIETE INTERNATIONALE 12 BIRDY SKINNY LOVE WEA WEA WARNER -

Forced Back to Danger Asylum-Seekers Returned from Europe to Afghanistan
FORCED BACK TO DANGER ASYLUM-SEEKERS RETURNED FROM EUROPE TO AFGHANISTAN I WELCOME Amnesty International is a global movement of more than 7 million people who campaign for a world where human rights are enjoyed by all. Our vision is for every person to enjoy all the rights enshrined in the Universal Declaration of Human Rights and other international human rights standards. We are independent of any government, political ideology, economic interest or religion and are funded mainly by our membership and public donations. © Amnesty International 2017 Except where otherwise noted, content in this document is licensed under a Creative Commons Cover photo: Afghan security forces personnel are seen at the site of a truck bomb attack in Kabul on 31 (attribution, non-commercial, no derivatives, international 4.0) licence. May 2017. At least 150 people were killed and hundreds injured as a massive blast ripped through https://creativecommons.org/licenses/by-nc-nd/4.0/legalcode Kabul's diplomatic quarter, shattering the morning rush hour and bringing carnage to the streets of the For more information please visit the permissions page on our website: www.amnesty.org Afghan capital. © Shah Marai/AFP/Getty Images Where material is attributed to a copyright owner other than Amnesty International this material is not subject to the Creative Commons licence. First published in 2017 by Amnesty International Ltd Peter Benenson House, 1 Easton Street London WC1X 0DW, UK Index: ASA 11/6866/2017 Original language: English amnesty.org CONTENTS GLOSSARY 4 EXECUTIVE SUMMARY 6 METHODOLOGY 11 1. FORCED BACK: STORIES FROM AFGHANISTAN 12 2. -

Top 100 No. 608 – 15.08.2011
CHARTSSERVICE – WORLDCHARTS – TOP 100 NO. 608 – 15.08.2011 PL VW WO PK ARTIST SONG 1 1 18 1 PITBULL ft. NE-YO, NAYER & AFROJACK give me everything 2 3 11 2 KATY PERRY last friday night (t.g.i.f.) 3 2 20 2 LMFAO ft. LAUREN BENNETT & GOONROCK party rock anthem 4 4 14 4 LADY GAGA the edge of glory 5 7 7 5 MAROON 5 ft. CHRISTINA AGUILERA moves like jagger 6 13 22 6 ADELE set fire to the rain 7 5 10 5 COLDPLAY every teardrop is a waterfall 8 6 30 4 ALEXANDRA STAN mr. saxobeat 9 14 7 9 BRITNEY SPEARS i wanna go 10 8 28 1 JENNIFER LOPEZ ft. PITBULL on the floor 11 11 35 8 ADELE rolling in the deep 12 9 11 9 JASON DERULO don't wanna go home 13 10 23 2 BRUNO MARS the lazy song 14 12 17 6 RIHANNA california king bed LUCENZO ft. DON OMAR / 15 15 43 15 LUCENZO & BIG ALI danza kuduro / vem dancar kuduro 16 17 7 16 BEYONCÉ best things i never had 17 16 12 15 BLACK EYED PEAS don't stop the party 18 20 17 18 SHAKIRA ft. PITBULL rabiosa 19 18 15 14 DAVID GUETTA ft. FLO RIDA & NICKI MINAJ where them girls at 20 21 22 6 SNOOP DOGG ft. DAVID GUETTA sweat 21 23 8 21 BAD MEETS EVIL ft. BRUNO MARS lighters 22 19 16 12 JENNIFER LOPEZ ft. LIL' WAYNE i'm into you 23 28 4 23 PITBULL ft. -

Crimes of the Community Honour-Based Violence in the UK
Crimes of the Community HONOUR-BASED VIOLENCE IN THE UK by James Brandon and Salam Hafez 2008 CENTRE FOR SO C I A L C O H E S ION Crimes of the Community: Honour-based violence in the UK by James Brandon and Salam Hafez Centre for Social Cohesion A Civitas Project Centre for Social Cohesion Clutha House 10 Storey’s Gate London SW1P 3AY Tel: +44 (0)20 7222 8909 Fax: +44 (0)5 601527476 Email: [email protected] www.socialcohesion.co.uk Director: Douglas Murray The Centre for Social Cohesion is a Civitas project CIVITAS is a registered charity: No. 1085494. Limited by guarantee. Registered in England and Wales: No. 04023541 © Centre for Social Cohesion, January 2008 All the Institute’s publications seek to further its objective of promoting the advancement of learning. The views expressed are those of the authors, not of the Institute. Crimes of the community: Honour-based violence in the UK All rights reserved ISBN 978-1-903386-64-4 Printed in Great Britain by The Cromwell Press Trowbridge, Wiltshire Contents Introduction 1 Ch A P T E R 1 Origins of honour 3 Introduction 3 Sexual honour 3 n Origins of an idea 3 n Honour today 4 Advantages of honour 5 Common ways in which honour can be damaged 6 Consequences of losing one’s honour 8 Ch A P T E R 2 Forced marriage 9 Introduction 9 Motives for forced marriage 12 Abuses related to forced marriage 15 n Physical violence 16 n Psychological and emotional violence 17 n Isolation, imprisonment and withdrawal from school 18 n Kidnapping and being forced to travel abroad 19 Abuses after a forced -

POSTAL ADDRESS Tbeats Studio 1204 Washington Avenue, Suite 400 Saint Louis, Missouri 63103
POSTAL ADDRESS TBeats Studio 1204 Washington Avenue, Suite 400 Saint Louis, Missouri 63103 CONTACT www.tbeatsstudio.com 314-754-5618 [email protected] Making Dreams Come True www.tbeatsstudio.com Press Kit About TBeats TBeats Studio is an affordable professional music production studio. The studio is located in St. Louis, Missouri at 1204 Washington Avenue on the 4th floor. TBeats Studios is owned by Tony Thompson and the signed artists, the marketing director, and the business development officer, giving the music industry a brand new model of an “Artist Owned Music Company.” TBeats provides a full range of services including high- quality music production and classes in audio recording, engineering, recording software and equipment. TBeats also offers artist support services including songwriting, publishing, artistic development, public relations, branding / marketing, and acting, fashion and career consulting. The TBeats Team developed the Live Your Dream program for high school seniors who have a passion for music and education. The goal of the organization is to seek out youth who might otherwise not have the opportunity to connect with those in the industry that can make their dreams come true by developing their music careers including production, business development, and overall growth development. Taking the possibilities of the students and showing them how to create a goal and aim for it, is one of the many tasks that TBeats cultivates. Our goal is to give a platform to students embarking on an artistic career so that their gifts can be exhibited in a substantial manner. Live Your Dream Project The Live Your Dream project was established to provide music scholarships to talented high school seniors who have a passion for music and education. -

Top 100 No. 609 – 22.08.2011
CHARTSSERVICE – WORLDCHARTS – TOP 100 NO. 609 – 22.08.2011 PL VW WO PK ARTIST SONG 1 1 19 1 PITBULL ft. NE-YO, NAYER & AFROJACK give me everything 2 2 12 2 KATY PERRY last friday night (t.g.i.f.) 3 5 8 3 MAROON 5 ft. CHRISTINA AGUILERA moves like jagger 4 3 21 2 LMFAO ft. LAUREN BENNETT & GOONROCK party rock anthem 5 4 15 4 LADY GAGA the edge of glory 6 7 11 5 COLDPLAY every teardrop is a waterfall 7 8 31 4 ALEXANDRA STAN mr. saxobeat 8 6 23 6 ADELE set fire to the rain 9 9 8 9 BRITNEY SPEARS i wanna go 10 11 36 8 ADELE rolling in the deep 11 10 29 1 JENNIFER LOPEZ ft. PITBULL on the floor LUCENZO ft. DON OMAR / 12 15 44 12 LUCENZO & BIG ALI danza kuduro / vem dancar kuduro 13 16 8 13 BEYONCÉ best things i never had 14 12 12 9 JASON DERULO don't wanna go home 15 14 18 6 RIHANNA california king bed 16 23 5 16 PITBULL ft. MARC ANTHONY rain over me 17 13 24 2 BRUNO MARS the lazy song 18 21 9 18 BAD MEETS EVIL ft. BRUNO MARS lighters 19 19 16 14 DAVID GUETTA ft. FLO RIDA & NICKI MINAJ where them girls at 20 17 13 15 BLACK EYED PEAS don't stop the party 21 24 27 17 ADELE someone like you 22 22 17 12 JENNIFER LOPEZ ft. LIL' WAYNE i'm into you 23 18 18 18 SHAKIRA ft. -

Journalism at the Borders
Journalism at the Borders Avh_Johan Östman_290809.indd 1 2009-07-30 10.01 Avh_Johan Östman_290809.indd 2 2009-07-30 10.01 Örebro Studies in Media and Communication 8 Örebro Studies in Conditions of Democracy 3 Johan Östman Journalism at the Borders The Constitution of Nationalist Closure in News Decoding Avh_Johan Östman_290809.indd 3 2009-07-30 10.01 © Johan Östman, 2009 Title: Journalism at the Borders. The Constitution of Nationalist Closure in News Decoding Publisher: Örebro University 2009 www.publications.oru.se Editor: Heinz Merten [email protected] Printer: intellecta infolog, Göteborg 08/2009 issn 1651-4785 isbn 978-91-7668-679-9 Avh_Johan Östman_290809.indd 4 2009-07-30 10.01 Abstract Östman, J. (2009) Journalism at the Borders. The Constitution of Nationalist Closure in News Decoding. Örebro studies in Media and Communication 8, Örebro Studies in Conditions of Democracy 3. This dissertation is a contribution to the social analysis of nationalism. Its disci- plinary context comprises the field of empirical studies that explore how forms of mediated quasi interaction can function in processes of reproduction and trans- formation of nationality. The study poses the question of how news journalism can establish national frames of reference within which social reality is made meaningful by citizens. The research design facilitates a novel contribution to a field of research that is largely dominated by studies of media output. Two distinct but intertwined do- mains are empirically studied: news as a form of discourse and the moment of news decoding as a form of social interaction between readers and texts. -
European Parliament
EUROPEAN PARLIAMENT Directorate General for Research WORKING PAPER HUMAN RIGHTS = WOMEN'S RIGHTS ? WOMEN'S RIGHTS SERIES w-7 DA DE EL ES FR IT NL PT Fl SV This publication is available in the following languages : DE EN ES FR NL This publication does not necessarily reflect the opinions of the European Parliament. Reproduction and translation for non-commercial purposes are authorized provided the source is acknowledged and the publisher is given prior notice and sent a copy. PUBLISHER: EUROPEAN PARLIAMENT DIRECTORATE-GENERAL FOR RESEARCH DIVISION FOR BUDGETARY AND CULTURAL AFFAIRS,WOMEN'S RIGHTS, CIVIL LIBERTIES AND INTERNAL AFFAIRS, RULES OF PROCEDURE, PETITIONS AND COMPARATIVE LAW L-2929 LUXEMBOURG B-1047 BRUSSELS TeL (32) 2/284 36 84 (Brussels) Fax (32) 2/284 49 55 (Brussels) EDITOR: Andrea SUBHAN assisted by Evelyne V ANNOOTE Manuscript completed in August 1995. EUROPEAN PARLIAMENT --•----- Directorate Gelleral fo.r Research WORKING PAPER HUMAN RIGHTS = WOMEN'S RIGHTS ? SUMMARY OF THE PUBLIC HEARING ORGANIZED BY THE COMMITTEE ON WOMEN'S RIGHTS 26-27 JUNE 1995 WOMEN'S RIGHTS SERIES w-7 6-1996 HUMAN RIGHTS= WOMEN'S RIGHTS? CONTENTS Page 1. Official opening by Mrs Anita GRADIN, Member of the Commission of the European Union 5 2. Mrs Nel VAN DIJK, Chairwoman of the Committee on Women's Rights 7 I. WOMEN'S RIGHTS AS AN INTEGRAL PART OF INDIVIDUAL RIGHTS 7 3. Mrs Marike RADSTAACKE, Representative of Amnesty International, Netherlands Section 7 4. Mrs Olof OLAFSDOTTIR, Head of the Equal Rights Section, Secretariat of the C.D.E.G., Directorate for Human Rights, Council of Europe . -
Les Indicateurs Radio
BILAN RADIO-TV-CLUB Programmation Musicale BILAN ANNEE 2013 [Bilan 2013] Tops 5 ● Radio ● TV ● Clubs 1 1 1 Daft Punk Stromae Bingo Players Get lucky Papaoutai Get up (Rattle) Columbia / Sony Mercury Group / Universal Happy Music Bruno Mars Saule feat. Major Lazer Charlie Winston Treasure Watch out for this Dusty men WEA / Warner Because / Warner Pias / Pïas Saule feat. Youssoupha Kid Cudi Charlie Winston feat. Ayna Pursuit of happiness Dusty men On se connait Def Jam / Universal Pias / Pias Believe Recordings Big Ali Robin Thicke Robin Thicke feat. Wati B Blurred lines Blurred lines WatiBigali Polydor / Universal Polydor / Universal Smart / Sony Génération Goldman Keen V Passenger (Leslie & Ivyrise) Elle t'a maté Let her go Je te donne (Fatoumata) Columbia / Sony My Major Company / Warner YP¨/ USM Bilan Radio Ce panel représente 95% de l’audience totale des radios musicales [Bilan 2013] Chiffres clés Radio (Panel constant 35 stations) Nombre % Diffusions % Diffusions Rotation Moyenne Francophones Francophones Hebdomadaire Diffusions (24h-24h) - (6h30-22h30) - 4,2 diffusions Internationales Diffusions 30,8% 3 673 289 - 0,9 pts 35,4% -0,2 vs 2012 5,8 diffusions Francophones Audiences 40,4% - 1% vs 2012 -1,7pts vs 2012 - 0,4 pts idem vs 2012 Nombre Nouveautés <1an Entrées en playlist Artistes # Titres # 39 142 titres 2 711 titres 32 739 Artistes +11,9% vs 2012 + 2,7% vs 2012 104 979 + 13,8% vs 2012 Francophones 4 912 804 Francophones 4 620 Francophones + 7,7% vs 2012 + 3,4% vs 2012 +7,2% vs 2012 + 3,4% vs 2012 [Bilan 2012] Focus Francophones (Panel 35 stations) Stat.