Skin, Orbicularis, Tarsus, and Conjunctiva. the Lower 5 Mm Has 7
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

MR Imaging of the Orbital Apex
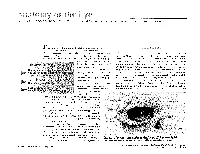
J Korean Radiol Soc 2000;4 :26 9-0 6 1 6 MR Imaging of the Orbital Apex: An a to m y and Pat h o l o g y 1 Ho Kyu Lee, M.D., Chang Jin Kim, M.D.2, Hyosook Ahn, M.D.3, Ji Hoon Shin, M.D., Choong Gon Choi, M.D., Dae Chul Suh, M.D. The apex of the orbit is basically formed by the optic canal, the superior orbital fis- su r e , and their contents. Space-occupying lesions in this area can result in clinical d- eficits caused by compression of the optic nerve or extraocular muscles. Even vas c u l a r changes in the cavernous sinus can produce a direct mass effect and affect the orbit ap e x. When pathologic changes in this region is suspected, contrast-enhanced MR imaging with fat saturation is very useful. According to the anatomic regions from which the lesions arise, they can be classi- fied as belonging to one of five groups; lesions of the optic nerve-sheath complex, of the conal and intraconal spaces, of the extraconal space and bony orbit, of the cav- ernous sinus or diffuse. The characteristic MR findings of various orbital lesions will be described in this paper. Index words : Orbit, diseases Orbit, MR The apex of the orbit is a complex region which con- tains many nerves, vessels, soft tissues, and bony struc- Anatomy of the orbital apex tures such as the superior orbital fissure and the optic canal (1-3), and is likely to be involved in various dis- The orbital apex region consists of the optic nerve- eases (3). -

Extraocular Muscles Orbital Muscles
EXTRAOCULAR MUSCLES ORBITAL MUSCLES INTRA- EXTRA- OCULAR OCULAR CILIARY MUSCLES INVOLUNTARY VOLUNTARY 1.Superior tarsal muscle. 1.Levator Palpebrae Superioris 2.Inferior tarsal muscle 2.Superior rectus 3.Inferior rectus 4.Medial rectus 5.Lateral rectus 6.Superior oblique 7.Inferior oblique LEVATOR PALPEBRAE SUPERIORIOS Origin- Inferior surface of lesser wing of sphenoid. Insertion- Upper lamina (Voluntary) - Anterior surface of superior tarsus & skin of upper eyelid. Middle lamina (Involuntary) - Superior margin of superior tarsus. (Superior Tarsus Muscle / Muller muscle) Lower lamina (Involuntary) - Superior conjunctival fornix Nerve Supply :- Voluntary part – Oculomotor Nerve Involuntary part – Sympathetic ACTION :- Elevation of upper eye lid C/S :- Drooping of upper eyelid. Congenital ptosis due to localized myogenic dysgenesis Complete ptosis - Injury to occulomotor nerve. Partial ptosis - disruption of postganglionic sympathetic fibres from superior cervical sympathetic ganglion. Extra ocular Muscles : Origin Levator palpebrae superioris Superior Oblique Superior Rectus Lateral Rectus Medial Rectus Inferior Oblique Inferior Rectus RECTUS MUSCLES : ORIGIN • Arises from a common tendinous ring knows as ANNULUS OF ZINN • Common ring of connective tissue • Anterior to optic foramen • Forms a muscle cone Clinical Significance Retrobulbar neuritis ○ Origin of SUPERIOR AND MEDIAL RECTUS are closely attached to the dural sheath of the optic nerve, which leads to pain during upward & inward movements of the globe. Thyroid orbitopathy ○ Medial & Inf.rectus thicken. especially near the orbital apex - compression of the optic nerve as it enters the optic canal adjacent to the body of the sphenoid bone. Ophthalmoplegia ○ Proptosis occur due to muscle laxity. Medial Rectus Superior Rectus Origin :- Superior limb of the tendonous ring, and optic nerve sheath. -

Turn-Over Orbital Septal Flap and Levator Recession for Upper-Eyelid
Eye (2013) 27, 1174–1179 & 2013 Macmillan Publishers Limited All rights reserved 0950-222X/13 www.nature.com/eye 1 2 3 1 CLINICAL STUDY Turn-over orbital A Watanabe , PN Shams , N Katori , S Kinoshita and D Selva2 septal flap and levator recession for upper-eyelid retraction secondary to thyroid eye disease Abstract Background A turn-over septal flap has been Keywords: upper-eyelid retraction; orbital reported as a spacer for levator lengthening septal flap; levator recession in a single case report. This study reports the preliminary outcomes of this technique in a series of patients with upper-lid retraction (ULR) associated with thyroid eye disease 1Department of Ophthalmology, Introduction Kyoto Prefectural University of (TED) causing symptomatic exposure Medicine, Kyoto, Japan keratopathy (EK). Achieving a predictable eyelid height and Methods Retrospective, multicenter study contour in the surgical correction of upper- 2 Department of Ophthalmology of 12 eyelids of 10 patients with TED eyelid retraction remains a challenge for and Visual Sciences, South Australian Institute of undergoing a transcutaneous levator- surgeons, as evidenced by the variety of Ophthalmology, Adelaide lengthening technique using the reflected procedures reported.1,2 These techniques are University, Adelaide, South orbital septum (OS) as a spacer. Change in based on weakening or lengthening the Australia, Australia palpebral aperture (PA) and contour, position upper-eyelid retractors and include anterior or 3Department of Oculoplastic of the skin crease (SC), symptoms of EK, and posterior approaches to graded recession and Orbital Surgery, Seirei complications were recorded. or resection of Mu¨ ller’s muscle,3–5 levator Hamamatsu Hospital, Results The average age was 47.5 years. -

Inferior Rectus Paresis After Secondary Blepharoplasty
Br J Ophthalmol: first published as 10.1136/bjo.68.8.535 on 1 August 1984. Downloaded from British Journal of Ophthalmology, 1984, 68, 535-537 Inferior rectus paresis after secondary blepharoplasty EDUARDO ALFONSO, ANDREW J. LEVADA, AND JOHN T. FLYNN From the Bascom Palmer Eye Institute, Department of Ophthalmology, University ofMiami School ofMedicine, Miami, Florida, USA SUMMARY A 52-year-old woman underwent a secondary cosmetic blepharoplasty for repair of residual dermatochalasis. Afterthis procedure vertical diplopia was noted. Ultrasound examination and the findings at operation were consistent with trauma to the inferior rectus muscle. We present this as an additional complication of cosmetic blepharoplasty. Numerous complications ofblepharoplasty have been The patient was examined by an ophthalmologist reported. They include blindness, orbital and eyelid and observation was recommended. One year later haematoma, epiphora, ectropion, lagophthalmos, she was examined by a second ophthalmologist in ptosis, incision' complications, scar thickening, Munich. A left hypertropia of 260 and exotropia of incomplete or excessive removal of orbital fat, 12° were found, and both inferior recti were thought lacrimal gland injury, exposure keratitis, and corneal to be involved. The patient could fuse only in gaze up ulcer. '-" Disturbances of ocular motility are and left. On 21 October 1981 she underwent a 5 mm uncommon, but superior oblique palsy,2 inferior recession ofthe right superior rectus muscle combined oblique injury,- superior rectus incarceration in the with release of conjunctival scar inferiorly, myotomy to ofthe inferior rectus muscle, and insertion of a Teflon wound,4 and restriction secondary retrobulbar http://bjo.bmj.com/ haemorrhage5 have been reported. -

The Complexity and Origins of the Human Eye: a Brief Study on the Anatomy, Physiology, and Origin of the Eye
Running Head: THE COMPLEX HUMAN EYE 1 The Complexity and Origins of the Human Eye: A Brief Study on the Anatomy, Physiology, and Origin of the Eye Evan Sebastian A Senior Thesis submitted in partial fulfillment of the requirements for graduation in the Honors Program Liberty University Spring 2010 THE COMPLEX HUMAN EYE 2 Acceptance of Senior Honors Thesis This Senior Honors Thesis is accepted in partial fulfillment of the requirements for graduation from the Honors Program of Liberty University. ______________________________ David A. Titcomb, PT, DPT Thesis Chair ______________________________ David DeWitt, Ph.D. Committee Member ______________________________ Garth McGibbon, M.S. Committee Member ______________________________ Marilyn Gadomski, Ph.D. Assistant Honors Director ______________________________ Date THE COMPLEX HUMAN EYE 3 Abstract The human eye has been the cause of much controversy in regards to its complexity and how the human eye came to be. Through following and discussing the anatomical and physiological functions of the eye, a better understanding of the argument of origins can be seen. The anatomy of the human eye and its many functions are clearly seen, through its complexity. When observing the intricacy of vision and all of the different aspects and connections, it does seem that the human eye is a miracle, no matter its origins. Major biological functions and processes occurring in the retina show the intensity of the eye’s intricacy. After viewing the eye and reviewing its anatomical and physiological domain, arguments regarding its origins are more clearly seen and understood. Evolutionary theory, in terms of Darwin’s thoughts, theorized fossilization of animals, computer simulations of eye evolution, and new research on supposed prior genes occurring in lower life forms leading to human life. -

Study Guide Medical Terminology by Thea Liza Batan About the Author
Study Guide Medical Terminology By Thea Liza Batan About the Author Thea Liza Batan earned a Master of Science in Nursing Administration in 2007 from Xavier University in Cincinnati, Ohio. She has worked as a staff nurse, nurse instructor, and level department head. She currently works as a simulation coordinator and a free- lance writer specializing in nursing and healthcare. All terms mentioned in this text that are known to be trademarks or service marks have been appropriately capitalized. Use of a term in this text shouldn’t be regarded as affecting the validity of any trademark or service mark. Copyright © 2017 by Penn Foster, Inc. All rights reserved. No part of the material protected by this copyright may be reproduced or utilized in any form or by any means, electronic or mechanical, including photocopying, recording, or by any information storage and retrieval system, without permission in writing from the copyright owner. Requests for permission to make copies of any part of the work should be mailed to Copyright Permissions, Penn Foster, 925 Oak Street, Scranton, Pennsylvania 18515. Printed in the United States of America CONTENTS INSTRUCTIONS 1 READING ASSIGNMENTS 3 LESSON 1: THE FUNDAMENTALS OF MEDICAL TERMINOLOGY 5 LESSON 2: DIAGNOSIS, INTERVENTION, AND HUMAN BODY TERMS 28 LESSON 3: MUSCULOSKELETAL, CIRCULATORY, AND RESPIRATORY SYSTEM TERMS 44 LESSON 4: DIGESTIVE, URINARY, AND REPRODUCTIVE SYSTEM TERMS 69 LESSON 5: INTEGUMENTARY, NERVOUS, AND ENDOCRINE S YSTEM TERMS 96 SELF-CHECK ANSWERS 134 © PENN FOSTER, INC. 2017 MEDICAL TERMINOLOGY PAGE III Contents INSTRUCTIONS INTRODUCTION Welcome to your course on medical terminology. You’re taking this course because you’re most likely interested in pursuing a health and science career, which entails proficiencyincommunicatingwithhealthcareprofessionalssuchasphysicians,nurses, or dentists. -
The Orbit Is Composed Anteri
DAVID L. PARVER, MD The University of Texas Southwestern Medical Center, Dallas Theability to successfully assess and treat The Orbit physical ailments requires an understanding of the anatomy involved in the injury or The eye itself lies within a protective shell trauma. When dealing with injuries and called the bony orbits. These bony cavities are trauma associated with the eye, it is neces- located on each side of the root of the nose. sary to have a work- Each orbit is structured like a pear with the ing knowledge of optic nerve, the nerve that carries visual im- basic ocular anatomy pulses from the retina to the brain, represent- so that an accurate ing the stem of the orbtt (Duke-Elder, 1976). Understa eye also diagnosis can be Seven bones make up the bony orbit: frontal, achieved and treat- zygomatic, maxillary, ethmoidal, sphenoid, ment can be imple- lacrimal, and palatine (Figures 1 and 2). in a bony " mented. The roof of the orbit is composed anteri- . .. The upcoming ar- orly of the orbital plate of the frontal bone ticles in this special and posteriorly by the lesser wing of the sphe- Each portion of the 01 I noid bone. The lateral wall is separated from .r. theme section the nervc an eye will deal specifically 2 with recognizing ocular illness, disease, and injuries, and will also address the incidence of sports related eye injuries and trauma. This paper covers the ba- sics of eye anatomy, focusing on the eye globe and its surrounding struc- tures. Once one gains an understand- ing of the normal anatomy of the eye, it will be easier to recognize trauma, injury, or illness. -

Eyelash Inversion in Epiblepharon: Is It Caused by Redundant Skin?
ORIGINAL RESEARCH Eyelash inversion in epiblepharon: Is it caused by redundant skin? Hirohiko Kakizaki1 Purpose: To evaluate the effect of redundant lower eyelid skin on the eyelash direction in Igal Leibovitch2 epiblepharon. Yasuhiro Takahashi3 Materials and methods: Asian patients with epiblepharon participated in this study. The Dinesh Selva4 lower eyelid skin was pulled downward in the upright position with the extent just to detach from eyelash roots, and the direction of the eyelashes was examined. These evaluations were 1Department of Ophthalmology, Aichi Medical University, Nagakute, repeated before surgery while the patients were lying supine under general anesthesia. Aichi 480-1195, Japan; 2Division of Results: The study included 41 lower eyelids of 25 patients (17 females, 8 males, average age; Oculoplastic and Orbital Surgery, 5.6 years, 16 cases bilateral, 9 unilateral). In the upright position, without downward traction Department of Ophthalmology, Tel-Aviv Medical Center, of the skin, the eyelashes were vertically positioned and touching the cornea. The redundant Tel-Aviv University, Tel-Aviv, Israel; skin touched only the eyelash roots and had minimal contribution to eyelash inversion. With 3 Department of Ophthalmology downward skin traction, there was no signifi cant change in the eyelash direction. In the spine and Visual Sciences, Osaka City University Graduate School position, the eyelashes were touching the cornea, and there was marked redundant skin that was of Medicine, Osaka 545-8585, Japan; pushing the eyelashes inward. With downward skin traction, there was no signifi cant change. 4 South Australian Institute Conclusions: The direction of lower eyelashes in patients with epiblepharon was less infl uenced of Ophthalmology and Discipline For personal use only. -

Evisceration, Enucleation and Exenteration
CHAPTER 10 EVISCERATION, ENUCLEATION AND EXENTERATION This chapter describes three operations that either remove the contents of the eye (evisceration), the eye itself (enucleation) or the whole orbital contents (exenteration). Each operation has specific indications which are important to understand. In many cultures the removal of an eye, even if blind, is resisted. If an eye is very painful or grossly disfigured an operation will be accepted more readily. However, if the eye looks normal the patient or their family may be very reluctant to accept its removal. Therefore tact, compassion and patience are needed when recommending these operations. ENUCLEATION AND EVISCERATION There are several reasons why either of these destructive operations may be necessary: 1. Malignant tumours in the eye. In the case of a malignant tumour or suspected malignant tumour the eye should be removed by enucleation and not evisceration.There are two important intraocular tumours, retinoblastoma and melanoma and for both of them the basic treatment is enucleation. Retinoblastoma is a relatively common tumour in early childhood. At first the growth is confined to the eye. Enucleation must be carried out at this stage and will probably save the child’s life. It is vital not to delay or postpone surgery. If a child under 6 has a blind eye and the possibility of a tumour cannot be ruled out, it is best to remove the eye. Always examine the other eye very carefully under anaesthetic as well. It may contain an early retinoblastoma which could be treatable and still save the eye. Retinoblastoma spreads along the optic nerve to the brain. -

Surgical Excision of Eyelid Lesions Reference Number: CP.VP.75 Coding Implications Last Review Date: 12/2020 Revision Log
Clinical Policy: Surgical Excision of Eyelid Lesions Reference Number: CP.VP.75 Coding Implications Last Review Date: 12/2020 Revision Log See Important Reminder at the end of this policy for important regulatory and legal information. Description: The majority of eyelid lesions are benign, ranging from innocuous cysts and chalazion/hordeolum to nevi and papillomas. Key features that should prompt further investigation include gradual enlargement, central ulceration or induration, irregular borders, eyelid margin destruction or loss of lashes, and telangiectasia. This policy describes the medical necessity requirements for surgical excision of eyelid lesions. Policy/Criteria I. It is the policy of health plans affiliated with Centene Corporation® (Centene) that surgical excision and repair of eyelid or conjunctiva due to lesion or cyst or eyelid foreign body removal is medically necessary for any of the following indications: A. Lesion with one or more of the following characteristics: 1. Bleeding; 2. Persistent or intense itching; 3. Pain; 4. Inflammation; 5. Restricts vision or eyelid function; 6. Misdirects eyelashes or eyelid; 7. Displaces lacrimal puncta or interferes with tear flow; 8. Touches globe; 9. Unknown etiology with potential for malignancy; B. Lesions classified as one of the following: 1. Malignant; 2. Benign; 3. Cutaneous papilloma; 4. Cysts; 5. Embedded foreign bodies; C. Periocular warts associated with chronic conjunctivitis. Background The majority of eyelid lesions are benign, ranging from innocuous cysts and chalazion/hordeolum to nevi and papillomas. Key features that should prompt further investigation include gradual enlargement, central ulceration or induration, irregular borders, eyelid margin destruction or loss of lashes, and telangiectasia. Benign tumors, even though benign, often require removal and therefore must be examined carefully and the differential diagnosis of a malignant eyelid tumor considered and the method of removal planned. -

98796-Anatomy of the Orbit
Anatomy of the orbit Prof. Pia C Sundgren MD, PhD Department of Diagnostic Radiology, Clinical Sciences, Lund University, Sweden Lund University / Faculty of Medicine / Inst. Clinical Sciences / Radiology / ECNR Dubrovnik / Oct 2018 Lund University / Faculty of Medicine / Inst. Clinical Sciences / Radiology / ECNR Dubrovnik / Oct 2018 Lay-out • brief overview of the basic anatomy of the orbit and its structures • the orbit is a complicated structure due to its embryological composition • high number of entities, and diseases due to its composition of ectoderm, surface ectoderm and mesoderm Recommend you to read for more details Lund University / Faculty of Medicine / Inst. Clinical Sciences / Radiology / ECNR Dubrovnik / Oct 2018 Lund University / Faculty of Medicine / Inst. Clinical Sciences / Radiology / ECNR Dubrovnik / Oct 2018 3 x 3 Imaging technique 3 layers: - neuroectoderm (retina, iris, optic nerve) - surface ectoderm (lens) • CT and / or MR - mesoderm (vascular structures, sclera, choroid) •IOM plane 3 spaces: - pre-septal •thin slices extraconal - post-septal • axial and coronal projections intraconal • CT: soft tissue and bone windows 3 motor nerves: - occulomotor (III) • MR: T1 pre and post, T2, STIR, fat suppression, DWI (?) - trochlear (IV) - abducens (VI) Lund University / Faculty of Medicine / Inst. Clinical Sciences / Radiology / ECNR Dubrovnik / Oct 2018 Lund University / Faculty of Medicine / Inst. Clinical Sciences / Radiology / ECNR Dubrovnik / Oct 2018 Superior orbital fissure • cranial nerves (CN) III, IV, and VI • lacrimal nerve • frontal nerve • nasociliary nerve • orbital branch of middle meningeal artery • recurrent branch of lacrimal artery • superior orbital vein • superior ophthalmic vein Lund University / Faculty of Medicine / Inst. Clinical Sciences / Radiology / ECNR Dubrovnik / Oct 2018 Lund University / Faculty of Medicine / Inst. -

Required List of Bones and Markings
REQUIRED LIST OF BONES AND MARKINGS Axial Skeleton Skull Cranial Bones (8) Frontal Bone (1) Supraorbital foramina Supraorbital ridges or margins Parietal Bones (2) Temporal Bones (2) External auditory meatus Mastoid process Styloid process Zygomatic process Mandibular fossa Foramen lacerum Carotid foramen Jugular foramen Stylomastoid foramen Internal auditory meatus Occipital Bone (1) Foramen magnum Occipital condyles Ethmoid Bone (1) Cribriform plate Olfactory foramina in cribriform plate Crista galli Perpendicular plate (forms superior part of nasal septum) Middle nasal concha Superior nasal concha Sphenoid Bone (1) Foramen ovale Foramen rotundum Sella turcica Greater wing Lesser wing Optic foramen Inferior orbital fissure Superior orbital fissure Pterygoid processes Skull (cont’d) Facial Bones (14) Lacrimal Bones (2) Lacrimal fossa Nasal Bones (2) Inferior Nasal Conchae (2) Vomer (1) (forms inferior portion of nasal septum) Zygomatic Bones (2) Temporal process (forms zygomatic arch with zygomatic process of temporal bone) Maxillae (2) Alveoli Palatine process (forms anterior part of hard palate) Palatine Bones (2) (form posterior part of hard palate) Mandible (1) Alveoli Body Mental foramen Ramus Condylar process (mandibular condyle) Coronoid process Miscellaneous (Skull) Paranasal sinuses are located in the ethmoid bone, sphenoid bone, frontal bone, and maxillae Zygomatic arch (“cheekbone”) is composed of the zygomatic process of the temporal bone and the temporal process of the zygomatic bone 2 pairs of nasal conchae (superior and middle) are part of the ethmoid bone. 1 pair (inferior) are separate facial bones. All the scroll-like conchae project into the lateral walls of the nasal cavity. Hard palate (“roof of mouth”) is composed of 2 palatine processes of the maxillae and the 2 palatine bones (total of 4 fused bones).