Midwifery Services: an Evaluation of Current Service Provision and Service Requirements for Sure Start Rotherham Central
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

From Working-Class to Underclass
REVISTA DIVERGENCIA ISSN: 0719-2398 N°5 / AÑO 3 / ENERO - JULIO 2014 / PP 51-75 FROM WORKING-CLASS TO UNDERCLASS: THE RISE AND FALL OF INDUSTRIAL CAPITALISM IN SOUTH YORKSHIRE DE CLASE TRABAJADORA A CLASES BAJAS: EL AUGE Y CAÍDA DEL CAPITALISMO INDUSTRIAL EN YORKSHIRE DEL SUR Charles J. Lockett* ABSTRACT: South Yorkshire has been a cauldron of ‘working-class politics’ for more than 150 years, reflecting deep changes in the social and economic fortunes of the British proletariat. There is a distinct circularity of experience between early industrial workers in Sheffield and Rotherham and the modern generation of zero-hours workers: since the 1980s, a more naked form of capitalism has reasserted itself, revealing the ‘post-war consensus’ to be a fleeting and incomplete phenomenon. This article will seek to probe the reasons for and political alternatives to the ‘long arc’ of the South Yorkshire working-class, from precariously employed day labourers to settled working-class and back again. Key words: working-class - development - neoliberalism - social-democracy - trade unionism. RESUMEN: South Yorkshire ha sido caldo de cultivo para la “acción política de la clase trabajadora” por mas de 150 años, reflejando cambios profundos en la suerte tanto económica como social, que ha experimentado el proletariado británico. Existe una experiencia circular distintiva entre los trabajadores de la época industrial temprana de Sheffield y Rotherham, y los trabajadores de la generación moderna de las «cero-horas»: desde la década de 1980, una forma de capitalismo mas desnuda se ha reafirmado, revelando que el «consenso de la post-guerra» fue un fenómeno fugaz e incompleto. -

74 Bus Time Schedule & Line Route
74 bus time schedule & line map 74 Rotherham - She∆eld View In Website Mode The 74 bus line (Rotherham - She∆eld) has 2 routes. For regular weekdays, their operation hours are: (1) Rotherham Town Centre <-> Waverley: 8:32 AM - 6:55 PM (2) Waverley <-> Rotherham Town Centre: 7:47 AM - 5:52 PM Use the Moovit App to ƒnd the closest 74 bus station near you and ƒnd out when is the next 74 bus arriving. Direction: Rotherham Town Centre <-> Waverley 74 bus Time Schedule 29 stops Rotherham Town Centre <-> Waverley Route VIEW LINE SCHEDULE Timetable: Sunday Not Operational Rotherham Interchange/B10, Rotherham Town Monday 8:32 AM - 6:55 PM Centre Tuesday 8:32 AM - 6:55 PM Corporation Street/Market Street, Rotherham Town Centre Wednesday 8:32 AM - 6:55 PM Corporation Street, Rotherham Thursday 8:32 AM - 6:55 PM Westgate/Unity Place, Rotherham Town Centre Friday 8:32 AM - 6:55 PM 28-32 Westgate, Rotherham Saturday 8:32 AM - 6:55 PM Canklow Road/Alma Road, Rotherham Town Centre Alma Road, Rotherham Canklow Road/Mill Street, Canklow 74 bus Info Direction: Rotherham Town Centre <-> Waverley Canklow Road/Jubilee Street, Canklow Stops: 29 Trip Duration: 21 min Canklow Road/Warden Street, Canklow Line Summary: Rotherham Interchange/B10, Rotherham Town Centre, Corporation Street/Market Canklow Road/Canklow Hill Road, Canklow Street, Rotherham Town Centre, Westgate/Unity Place, Rotherham Town Centre, Canklow Road/Alma Centenary Way/West Bawtry Road, Canklow Road, Rotherham Town Centre, Canklow Road/Mill Street, Canklow, Canklow Road/Jubilee Street, Bawtry -

To Registers of General Admission South Yorkshire Lunatic Asylum (Later Middlewood Hospital), 1872 - 1910 : Surnames L-R
Index to Registers of General Admission South Yorkshire Lunatic Asylum (Later Middlewood Hospital), 1872 - 1910 : Surnames L-R To order a copy of an entry (which will include more information than is in this index) please complete an order form (www.sheffield.gov.uk/libraries/archives‐and‐local‐studies/copying‐ services) and send with a sterling cheque for £8.00. Please quote the name of the patient, their number and the reference number. Surname First names Date of admission Age Occupation Abode Cause of insanity Date of discharge, death, etc No. Ref No. Laceby John 01 July 1879 39 None Killingholme Weak intellect 08 February 1882 1257 NHS3/5/1/3 Lacey James 23 July 1901 26 Labourer Handsworth Epilepsy 07 November 1918 5840 NHS3/5/1/14 Lack Frances Emily 06 May 1910 24 Sheffield 30 September 1910 8714 NHS3/5/1/21 Ladlow James 14 February 1894 25 Pit Laborer Barnsley Not known 10 December 1913 4203 NHS3/5/1/10 Laidler Emily 31 December 1879 36 Housewife Sheffield Religion 30 June 1887 1489 NHS3/5/1/3 Laines Sarah 01 July 1879 42 Servant Willingham Not known 07 February 1880 1375 NHS3/5/1/3 Laister Ethel Beatrice 30 September 1910 21 Sheffield 05 July 1911 8827 NHS3/5/1/21 Laister William 18 September 1899 40 Horsekeeper Sheffield Influenza 21 December 1899 5375 NHS3/5/1/13 Laister William 28 March 1905 43 Horse keeper Sheffield Not known 14 June 1905 6732 NHS3/5/1/17 Laister William 28 April 1906 44 Carter Sheffield Not known 03 November 1906 6968 NHS3/5/1/18 Laitner Sarah 04 April 1898 29 Furniture travellers wife Worksop Death of two -

NHS Rotherham GP Commissioning Localities - January 2011
NHS Rotherham GP Commissioning Localities - January 2011 PA Rep STUART LAKIN Central North GP Lead Other GP's with in the practice Practice Name Practice Manager Address Telephone List Size Kirsty Gillgrass Dr Everett, Brynes, Jones, Bhattacharya, Woodstock Bower Group PracticeBernadette Conway Kimberworth Road, Rotherham, South 0844 8151956 11524 Adrian Cole, Rihal, Saeed Yorkshire, S61 1AH Naresh PATEL Dr Stott, Martin, Cullen, Sanders, Kacker, Broom Lane Medical PracticeMartyn Heeley 70 Broom Lane, Rotherham, S60 3EW 0844 477 39 79 12574 George, Thomas Shrinivas Ravula Dr M Husain Greasbrough Medical Centre Claire Astbury Greasbrough, Greenside, Rotherham, South 01709 559955 3269 Yorkshire, S61 4PT Charles Collinson Dr Myers, Barragry, Evans Greenside Surgery Carole Dalling Munsbrough Rise, Greasborough, 0845 1240887 5187 Rotherham, South Yorkshire, S61 4RB Total 32554 PA Rep GOVINDER BHOGAL RICHARD RUSSELL Central Two Practice Practice Name Practice Manager Address Telephone List Size Tariq Ahmed Dr Nazir, Jubb, Ghaebi and Chikthimmah Kilnhurst Surgery Steve Hindle Magna Lane, Dalton, Rotherham, South 0845 1244746 7011 (Deputy) Yorkshire, S65 4HH Nayyer Ishaque Dr Iqbal Dalton Health Centre Angela Madden Magna Lane, Dalton, Rotherham, South 0845 1266430 2040 Yorkshire, S65 4HH Hilal Jarjis Badsley Moor Lane Surgery Julie Gibson 292 Badsley Moor Lane, Rotherham, South 0845 1222276 2464 Yorkshire, S65 2QW Saheel BATT Dr A Goni and Dr M S Chauhdry Shakespeare Road Surgery Diane Batham 50 Shakespeare Road, Eastwood, 0845 1213122 4879 -
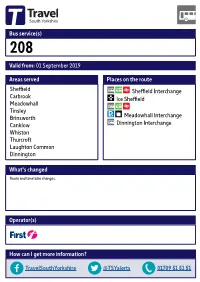
Valid From: 01 September 2019 Bus Service(S) What's Changed Areas
Bus service(s) 208 Valid from: 01 September 2019 Areas served Places on the route Sheffield Sheffield Interchange Carbrook Ice Sheffield Meadowhall Tinsley Brinsworth Meadowhall Interchange Canklow Dinnington Interchange Whiston Thurcroft Laughton Common Dinnington What’s changed Route and timetable changes. Operator(s) How can I get more information? TravelSouthYorkshire @TSYalerts 01709 51 51 51 Bus route map for service 208 01/02/2019 Scholes Parkgate Dalton Thrybergh Braithwell Ecclesfield Ravenfield Common Kimberworth East Dene Blackburn ! Holmes Meadowhall, Interchange Flanderwell Brinsworth, Hellaby Bonet Lane/ Bramley Wincobank Brinsworth Lane Maltby ! Longley ! Brinsworth, Meadowhall, Whiston, Worrygoose Lane/Reresby Drive ! Ñ Whitehill Lane/ Meadowhall Drive/ Hooton Levitt Bawtry Road Meadowhall Way 208 Norwood ! Thurcroft, Morthen Road/Green Lane Meadowhall, Whiston, ! Meadowhall Way/ Worrygoose Lane/ Atterclie, Vulcan Road Greystones Road Thurcroft, Katherine Road/Green Arbour Road ! Pitsmoor Atterclie Road/ Brinsworth, Staniforth Road Comprehensive School Bus Park ! Thurcroft, Katherine Road/Peter Street Laughton Common, ! ! Station Road/Hangsman Lane ! Atterclie, AtterclieDarnall Road/Shortridge Street ! ! ! Treeton Dinnington, ! ! ! Ulley ! Doe Quarry Lane/ ! ! ! Dinnington Comp School ! Sheeld, Interchange Laughton Common, Station Road/ ! 208! Rotherham Road 208 ! Aughton ! Handsworth ! 208 !! Manor !! Dinnington, Interchange Richmond ! ! ! Aston database right 2019 Swallownest and Heeley Todwick ! Woodhouse yright p o c Intake North Anston own r C Hurlfield ! data © y Frecheville e Beighton v Sur e South Anston c ! Wales dnan ! r O ! ! ! ! Kiveton Park ! ! ! ! ! ! Sothall ontains C 2019 ! = Terminus point = Public transport = Shopping area = Bus route & stops = Rail line & station = Tram route & stop 24 hour clock 24 hour clock Throughout South Yorkshire our timetables use the 24 hour clock to avoid confusion between am and pm times. -

Rotherham Primary Care Estates Strategy V8
Rotherham Clinical Commissioning Group gy Amended November 2020 Intentionally Left Blank Rotherham Primary Care Estates Strategy 1 1. EXECUTIVE SUMMARY 1. EXECUTIVE SUMMARY 6.4.2. Key Issues from Appraisal and Mapping 6.4.3. Central North Locality Estates Prioritisation 2. INTRODUCTION 6.5. Health Village / Central Locality 6.5.1. Property Assessment 3. STRATEGIC CONTEXT 6.5.2. Key Issues from Appraisal and Mapping 3.1. National Policy Context 6.5.3. Health Village / Central Locality Estate Prioritisation 3.2. Five Year Forward View 6.6. Maltby & Wickersley Locality 3.3. Delivering the Five Year Forward View 6.6.1. Premises Assessment 3.4. General Practice Forward View 6.6.2. Key Issues from Appraisal and Mapping 3.5. Next Steps on Five Year Forward View 6.6.3. Maltby & Wickersley Locality Estates Prioritisation 6.7. Wentworth South Locality 4. ROTHERHAM COMMISSIONING PRIORITIES, ORGANISATIONS AND 6.7.1. Premises Assessment STRATEGIC PARTNERS 6.7.2. Key Issues from Appraisal and Mapping 4.1. Health and Social Pen Picture of Rotherham 6.7.3. Wentworth South Locality Estates Prioritisation 4.1.1. Socio-economic Profile 6.8. Wath / Swinton Locality 4.1.2. Housing 6.8.1. Premises Assessment 4.1.3. Demographic Profile 6.8.2. Key Issues from Appraisal and Mapping 4.1.4. Health Needs 6.8.3. Wath / Swinton Locality Estates Prioritisation 4.2. Clinical Commissioning Groups 4.3. Local Authorities 7. FINANCIAL SUMMARY 4.4. Providers / Third Sector 4.5. South Yorkshire & Bassetlaw Integrated Care System (STP) 8. 2020 UPDATE 5. REVIEW OF THE PRIMARY CARE ESTATE ACROSS ROTHERHAM 5.1. -

Former County of South Yorkshire
Archaeological Investigations Project 2002 Post-Determination & Non-Planning Related Projects Yorkshire & Humberside Region FORMER COUNTY OF SOUTH YORKSHIRE Doncaster 3/1690 (E.04.J004) SK 49409600 FIRSBY HALL FARM, CONISBROUGH. An Archaeological Watching Brief at Firsby Hall Farm, Conisbrough. South Yorkshire Davies, G. Sheffield : ARCUS, 2002, 26pp, figs, tabs, refs Work undertaken by: ARCUS A watching brief was carried out on the site. No undisturbed deposits and no in situ structures were identified. There were numerous fragments of burnt clay probably from kilns, suggesting there presence nearby. These remains were identified as likely to be related to the medieval pottery production site previously identified in Firsby. [Au(adp)] Archaeological periods represented: MD 3/1691 (E.04.J002) SE 62000410 MARKHAM MAIN RESTORATION PROJECTS, DONCASTER Markham Main Restration Project. Doncaster, South Yorkshire Archaeological Services WYAS Morley : Archaeological Services WYAS, 2002, 16pp, pls, figs, refs Work undertaken by: Archaeological Services WYAS An archaeological watching brief was maintained during part of the landscaping for the Markham Main Restoration Project. The Groundworks proved to be less intrusive than expected and no features or deposits of an archaeological origin were identified. [Au(abr)] 3/1692 (E.04.H001) SE 53691203 ST HELENS CHURCH, BURGHWALLIS St Helen's Church, Burghwallis, South Yorkshire Dennison, E Beverley : Ed Dennison Archaeological Services, 2002, 21pp, colour pls, figs, tabs Work undertaken by: Ed Dennison Archaeological Services An archaeological watching brief was carried out on groundworks at the site. A pit was recorded containing a childs stone coffin, covered by two undecorated stone slabs. The remains of a slightly curved wall just to the north of the coffin was also observed. -

Rotherham Unique Reference Number
INSPECTION REPORT CANKLOW WOOD PRIMARY SCHOOL Canklow, Rotherham, South Yorkshire LEA area: Rotherham Unique reference number: 131696 Headteacher: Mr A Clark Lead inspector: Mr J R Francis Dates of inspection: 8th March 2004 Inspection number: 255705 Inspection carried out under section 10 of the School Inspections Act 1996 © Crown copyright 2004 This report may be reproduced in whole or in part for non-commercial educational purposes, provided that all extracts quoted are reproduced verbatim without adaptation and on condition that the source and date thereof are stated. Further copies of this report are obtainable from the school. Under the School Inspections Act 1996, the school must provide a copy of this report and/or its summary free of charge to certain categories of people. A charge not exceeding the full cost of reproduction may be made for any other copies supplied. Canklow Wood Primary School - 2 INFORMATION ABOUT THE SCHOOL Type of school: Primary School category: Community Age range of pupils: 3 – 11 years Gender of pupils: Mixed Number on roll: 177 plus 17 part-time in the nursery School address: Wood Lane Canklow Rotherham South Yorkshire Postcode: S60 2XJ Telephone number: 01709 828405 Fax number: 01709 837873 Appropriate authority: Governing Body Name of chair of governors: Mrs M Sheard Date of previous inspection: 22nd March 1999 CHARACTERISTICS OF THE SCHOOL This average sized primary school has 177 pupils in six classes and 17 children who attend the nursery part-time. There are a similar number of boys and girls. The school also houses a Learning Centre funded through the Excellence in Cities project1. -

Nnfoi 200 Nd
NNFOI_ND Property Address Liable Party Contact Address Rateable Value C/O Capa Audit & Property Advisors, Audit ., Poplar Way, Catcliffe, Rotherham, South Yorkshire, Woolworths P L C - In Department, Po Box 29416, Glasgow, S60 5TR Administration G67 1XU £1,220,000.00 ., Greasbrough Street, Rotherham, South Yorkshire, Oakgate House, 25 Market Street, S60 1LQ Oakgate Rotherham Llp Wetherby, LS22 6LQ £377,500.00 Building 36, Meadows Road, Wath Upon Dearne, Rotherham, South Yorkshire, S63 5DJ Lazarus Properties Ltd 3 Lazarus Court, Doncaster, DN1 3NF £320,000.00 C/O C B Richard Ellis Portfolio Management , 2nd Floor , St Martin'S Town Mills, Canklow Road, Rotherham, South Court, 10 Paternoster Row, London, Yorkshire, S60 2JG Premier Foods Group Ltd EC4M 7HP £305,000.00 C/O Pendragon Plc - Property Dept, Loxley House, 2 Oakwood Court Little ., Great Eastern Way, Parkgate, Rotherham, South Andre Baldet Ltd T/A Evans Oak Drive, Annesley, Nottingham, NG15 Yorkshire, S62 6JD Halshaw 0DR £300,000.00 Unit 1 - Mansells, Adwick Park, Wath Upon Dearne, Cert Octavian House, St Martins Road, Rotherham, South Yorkshire, S63 5NB Cert Octavian Plc Hoddesdon, Herts, EN11 0BT £285,000.00 M F I Group Ltd (In C/O M C R, 43/45 Portman Square, Unit 9, Beale Way, Parkgate, Rotherham, S62 6EJ Administration) London, W1H 6LY £272,500.00 27 29, College Street, Rotherham, South Yorkshire, Nations House, 103 Wigmore Street, S65 1AG G E P (North) Ltd London, W1U 1QS £209,000.00 C/O Robert Smith Financial Management Warehouse, (Former Gloystarne Ltd), Don Street, The -

South Yorkshire
INDUSTRIAL HISTORY of SOUTH RKSHI E Association for Industrial Archaeology CONTENTS 1 INTRODUCTION 6 STEEL 26 10 TEXTILE 2 FARMING, FOOD AND The cementation process 26 Wool 53 DRINK, WOODLANDS Crucible steel 27 Cotton 54 Land drainage 4 Wire 29 Linen weaving 54 Farm Engine houses 4 The 19thC steel revolution 31 Artificial fibres 55 Corn milling 5 Alloy steels 32 Clothing 55 Water Corn Mills 5 Forging and rolling 33 11 OTHER MANUFACTUR- Windmills 6 Magnets 34 ING INDUSTRIES Steam corn mills 6 Don Valley & Sheffield maps 35 Chemicals 56 Other foods 6 South Yorkshire map 36-7 Upholstery 57 Maltings 7 7 ENGINEERING AND Tanning 57 Breweries 7 VEHICLES 38 Paper 57 Snuff 8 Engineering 38 Printing 58 Woodlands and timber 8 Ships and boats 40 12 GAS, ELECTRICITY, 3 COAL 9 Railway vehicles 40 SEWERAGE Coal settlements 14 Road vehicles 41 Gas 59 4 OTHER MINERALS AND 8 CUTLERY AND Electricity 59 MINERAL PRODUCTS 15 SILVERWARE 42 Water 60 Lime 15 Cutlery 42 Sewerage 61 Ruddle 16 Hand forges 42 13 TRANSPORT Bricks 16 Water power 43 Roads 62 Fireclay 16 Workshops 44 Canals 64 Pottery 17 Silverware 45 Tramroads 65 Glass 17 Other products 48 Railways 66 5 IRON 19 Handles and scales 48 Town Trams 68 Iron mining 19 9 EDGE TOOLS Other road transport 68 Foundries 22 Agricultural tools 49 14 MUSEUMS 69 Wrought iron and water power 23 Other Edge Tools and Files 50 Index 70 Further reading 71 USING THIS BOOK South Yorkshire has a long history of industry including water power, iron, steel, engineering, coal, textiles, and glass. -

Rotherham Circular Walk ‘A Meeting of Two Rivers’
Rotherham Circular Walk ‘A Meeting of Two Rivers’ Walk summary: A flat walk through the town centre and Page | 1 up a steady incline to the highest point of Rotherham with substantial views of Rotherham and Sheffield. Find out what the Boston Tea Party has to do with the town and the connection to New York. Distance: 2.7 miles / 4.3 kilometres Duration: approximately 1.5 hours not including stops Terrain: Flat, pavement walking involving some road crossings. Some steady inclines. Nearest Car Park: Pay and Display, George Street, S60 1EY 1. Rotherham Train Station With your back to the train station entrance, turn left and then immediately right to cross the bridge over the canal and River Don. On the left hand side of the second bridge, past the Bridge Inn is the Chapel of our Lady on the Bridge. Carefully cross over to the chapel and take a look. 2. Chapel of our Lady on the Bridge The chapel is one of only three surviving medieval bridge chapels still standing in the whole of England. The chapel was used by travellers to give thanks for a safe arrival or pray for a safe journey. Rotherham Bridge was built on the site of an old ford, possibly on the site of an older narrow packhorse bridge. The bridge is believed to have been a toll bridge: the priests levying a charge to cross in return for the upkeep. In 1483 The Chapel of Our Lady was built as part of the rebuilding of the bridge. The chapel was richly decorated but in 1547 the chapel was suppressed by Henry VIII and anything of value removed but the chapel survived because it was an integral part of the bridge. -

Strategic Green Belt Review April 2012
Rotherham local plan Rotherham Strategic Green Belt Review April 2012 www.rotherham.gov.uk Rotherham Strategic Green Belt Review Contents 1. Introduction & Need for the Study ....................................................................................................2 2. Aim of the Study..................................................................................................................................2 3. Scope....................................................................................................................................................3 4. Planning Policy Context .....................................................................................................................4 5. Methodology ........................................................................................................................................7 6. Strategic Green Belt Review : Informing Local Plan Preparation .............................................12 7. Results................................................................................................................................................13 8. Conclusion..........................................................................................................................................13 Appendix 1 – Methodology Consultation...............................................................................................15 Appendix 2 – Stage 2: Criteria to assess parcels against Green Belt purposes 1-4 .....................22 Appendix 3