Lyme Borreliosis in Finland, 1995–2014
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Preliminary Population Statistics 2017, March
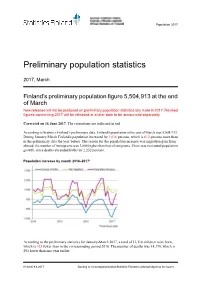
Population 2017 Preliminary population statistics 2017, March Finland’s preliminary population figure 5,504,913 at the end of March New releases will not be produced on preliminary population statistics any more in 2017. Revised figures concerning 2017 will be released at a later date to be announced separately. Corrected on 16 June 2017. The corrections are indicated in red. According to Statistics Finland's preliminary data, Finland's population at the end of March was 5,504,913. During January-March Finland's population increased by 1,616 persons, which is 612 persons more than in the preliminary data the year before. The reason for the population increase was migration gain from abroad: the number of immigrants was 3,868 higher than that of emigrants. There was no natural population growth, since deaths exceeded births by 2,252 persons. Population increase by month 2014–2017* According to the preliminary statistics for January-March 2017, a total of 12,118 children were born, which is 925 fewer than in the corresponding period 2016. The number of deaths was 14,370, which is 291 lower than one year earlier. Helsinki 9.6.2017 Quoting is encouraged provided Statistics Finland is acknowledged as the source. Altogether 7,062 persons immigrated to Finland from abroad and 3,194 persons emigrated from Finland during January-March period. The number of immigrants was 828 higher and the number of emigrants 418 lower than in the previous year. 1 520 of the immigrants and 2,127 of the emigrants were Finnish citizens. According to the preliminary data, the number of inter-municipal migrations totalled 56,798 by the end of March. -
Accommodation Statistics
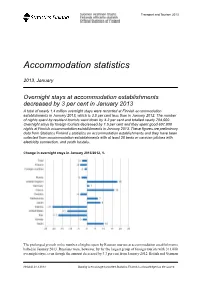
Transport and Tourism 2013 Accommodation statistics 2013, January Overnight stays at accommodation establishments decreased by 3 per cent in January 2013 A total of nearly 1.4 million overnight stays were recorded at Finnish accommodation establishments in January 2013, which is 3.0 per cent less than in January 2012. The number of nights spent by resident tourists went down by 4.2 per cent and totalled nearly 754,000. Overnight stays by foreign tourists decreased by 1.5 per cent and they spent good 607,000 nights at Finnish accommodation establishments in January 2013. These figures are preliminary data from Statistics Finland’s statistics on accommodation establishments and they have been collected from accommodation establishments with at least 20 beds or caravan pitches with electricity connection, and youth hostels. Change in overnight stays in January 2013/2012, % The prolonged growth in the number of nights spent by Russian tourists at accommodation establishments halted in January 2013. Russians were, however, by far the largest group of foreign tourists with 311,000 overnight stays, even though the amount decreased by 3.3 per cent from January 2012. British and German Helsinki 21.3.2013 Quoting is encouraged provided Statistics Finland is acknowledged as the source. visitors came next. For British tourists, 46,000 overnight stays were recorded and 32,000 for German tourists. Overnight stays by British tourists increased by 18.2 per cent and those by German tourists by 1.4 per cent. Overnight stays by French tourists also increased heavily by 16.3 per and they spent nearly 30,000 nights at Finnish accommodation establishments. -

Central Ostrobothnia Polytechnic, Kokkola, Finland
Language LHU Cost of Study Type of Approximate Eligibility VISA of partner Housing & Period Housing semester dates Instruction since Meals LHU and Housing external Fall Yes Fall: Sept. – Dec. €185-€280* students; and/or English Apartments 1996 Spring: Jan. - April Groceries Minimum Spring €300 GPA 2.5 F I N L A N D Centria University of Applied Sciences, Kokkola http://web.centria.fi/Default.aspx The Location Finland is the northernmost country in the world after Iceland. Don’t be deterred, however, by the weather. Partly because of the warming influence of the Gulf Stream, the climate is not as cold as one might think. The city of Kokkola, population 50,000, is a charming harbor town on the Gulf of Bothnia, 550 miles northwest of Helsinki. Today, Kokkola is not only the regional center of Central Ostrobothnia but also the most northerly point of coastal Swedish speaking Ostrobothnia (about 20% of the town’s inhabitants consider Swedish their native language). Take a walk into the old town with its museums and hundreds of wooden houses from the 17th and 18th centuries. The scenic “Seven Bridges Archipelago Road,” a 25-mile coastal drive connecting Kokkola with Pietarsaari to the south, is breathtaking. The University Kokkola is the main campus of Centria University of Applied Sciences (CU), a network of three institutions that include two other campuses located in Pietarsaari and Ylivieskai. Since Centria’s creation in 1992, international cooperation has been a focus of its outreach program. Currently, there are approximately 500 international students attending Centria, all of whom receive support from Centria’s International Office staff. -

Maakuntien Nimet Neljällä Kielellä (Fi-Sv-En-Ru) Ja Kuntien Nimet Suomen-, Ruotsin- Ja Englanninkielisiä Tekstejä Varten
16.1.2019 Suomen hallintorakenteeseen ja maakuntauudistukseen liittyviä termejä sekä maakuntien ja kuntien nimet fi-sv-en-(ru) Tiedosto sisältää ensin Suomen hallintorakenteeseen ja hallinnon tasoihin liittyviä termejä suomeksi, ruotsiksi ja englanniksi. Myöhemmin tiedostossa on termejä (fi-sv-en), jotka koskevat suunniteltua maakuntauudistusta. Lopuksi luetellaan maakuntien nimet neljällä kielellä (fi-sv-en-ru) ja kuntien nimet suomen-, ruotsin- ja englanninkielisiä tekstejä varten. Vastineet on pohdittu valtioneuvoston kanslian käännös- ja kielitoimialan ruotsin ja englannin kielityöryhmissä ja niitä suositetaan käytettäväksi kaikissa valtionhallinnon teksteissä. Termisuosituksiin voidaan tarvittaessa tehdä muutoksia tai täydennyksiä. Termivalintoja koskeva palaute on tervetullutta osoitteeseen termineuvonta(a)vnk.fi. Termer med anknytning till förvaltningsstrukturen i Finland och till landskapsreformen samt landskaps- och kommunnamn fi-sv-en-(ru) Först i filen finns finska, svenska och engelska termer med anknytning till förvaltningsstrukturen och förvaltningsnivåerna i Finland. Sedan följer finska, svenska och engelska termer som gäller den planerade landskapsreformen. I slutet av filen finns en fyrspråkig förteckning över landskapsnamnen (fi-sv-en-ru) och en förteckning över kommunnamnen för finska, svenska och engelska texter. Motsvarigheterna har tagits fram i svenska och engelska arbetsgrupper i översättnings- och språksektorn vid statsrådets kansli och det rekommenderas att motsvarigheterna används i statsförvaltningens texter. -

111223 Pohjois-Suomi 11 4 2012 Updatekv
Version: Final Date: 18 April 2012 Regional Innovation Monitor Regional Innovation Report (Pohjois-Suomi) To the European Commission Enterprise and Industry Directorate-General Directorate D – Industrial Innovation and Mobility Industries Kimmo Viljamaa Henri Lahtinen Ramboll Management Consulting www.technopolis-group.com PREFACE The Regional Innovation Monitor (RIM)1 is an initiative of the European Commission's Directorate General for Enterprise and Industry, which has the objective to describe and analyse innovation policy trends across EU regions. RIM analysis is based on methodologies developed in the context of the INNO-Policy Trendchart which covers innovation policies at national level as part of the PRO INNO Europe initiative. The overarching objective of this project is to enhance the competitiveness of European regions through increasing the effectiveness of their innovation policies and strategies. The specific objective of the RIM is to enhance the scope and quality of policy assessment by providing policy-makers, other innovation stakeholders with the analytical framework and tools for evaluating the strengths and weaknesses of regional policies and regional innovation systems. RIM covers EU-20 Member States: Austria, Belgium, Bulgaria, the Czech Republic, Denmark, Finland, France, Germany, Greece, Hungary, Ireland, Italy, the Netherlands, Poland, Portugal, Romania, Slovakia, Spain, Sweden and the United Kingdom. This means that RIM will not concentrate on Member States where the Nomenclature of territorial units for statistics NUTS 1 and 2 levels are identical with the entire country (Estonia, Latvia, and Lithuania), Malta which only has NUTS 3 regions, Slovenia which has a national innovation policy or Cyprus and Luxembourg which are countries without NUTS regions. -
Redistributive Regionalism Narratives on Regionalisation in the Nordic Periphery
Redistributive regionalism Narratives on regionalisation in the Nordic periphery Lisa Hörnström Department of Political Science SE-901 87 Umeå, Sweden Umeå 2010 Copyright©Lisa Hörnström ISBN: 978-91-7459-001-2 ISSN: 0349-0831. Research Report 2010:2 Cover: Micaela Adolfsson Printed by: Print & Media, Umeå University, 2007900 Umeå, Sweden 2010 To my grand-father Table of Contents Table of Contents................................................................................................i Abstract............................................................................................................... v Preface............................................................................................................... vii 1. Setting the scene ..............................................................................................................1 1.1 THE NORDIC PERIPHERY..................................................................................... 3 1.2 OUTLINE OF THE STUDY...................................................................................... 6 1.3 DISPOSITION OF THE THESIS............................................................................. 7 2. From centralist redistributive policy to new regionalism ...........................9 2.1 KEY CONCEPTS ....................................................................................................... 10 What is a region?........................................................................................................... 10 Regionalism -

Northern Sparsely Populated Areas Network Calls for a Strong Cohesion Policy Post-2020 (10.6.2016)
Northern Sparsely Populated Areas network calls for a strong cohesion policy post-2020 (10.6.2016) The Northern Sparsely Populated Areas network, NSPA, represents the interests of the four northernmost counties and regions of Sweden (Norrbotten, Västerbotten, Jämtland Härjedalen and Västernorrland), seven northernmost and eastern regions of Finland (Central Ostrobothnia, Kainuu, Lapland, North Karelia, Northern Ostrobothnia, Pohjois-Savo and Etelä-Savo) and North Norway (Finnmark, Troms and Nordland). The NSPA – a significant partner for tackling challenges within the European Union In order to strengthen European competitiveness, it is important that regional viability is based on regional strength and smart specialisation. All the European Union initiatives depend heavily on the regional level for successful implementation. Regions also offer political identification and legitimize the European Union to the citizens. The EU regional policy, the cohesion policy with its structural and investment funds, is therefore also a tool for creating legitimacy for the European project down to the regional and local level; additionally, it assures the engagement of all regions and their will to contribute to the EU, building capacity and interest in active partnership, and finding cooperation not otherwise fostered, within the regions, between the regions and throughout Europe as a whole. The Northern Sparsely Populated Areas network, NSPA, is a strong, specific and promising region. The NSPA region is also an important part of the EU, most notably due to the abundance of natural resources and nature values, advanced research institutions and high-performance industries in the area. It is, furthermore, an integral part of the Arctic, which is gaining importance at both European and global levels. -

The NSPA Views on EU's Long-Term Vision for Rural Areas
Position on EU’s long-term vision for rural areas NSPA Steering Committee December 2, 2020 The NSPA views on EU’s long-term vision for rural areas The Northern Sparsely Populated Areas network, NSPA, represents the interests of the four northernmost regions of Sweden (Norrbotten, Västerbotten, Jämtland Härjedalen and Västernorrland), the seven eastern and northernmost of Finland (Central Ostrobothnia, Kainuu, Lapland, North Karelia, Northern Ostrobothnia, Pohjois-Savo and South Savo), as well as the two northernmost regions of Norway (Nordland, Troms & Finnmark). In regard to the European Commission’s consultation on a long-term vision for Europe’s rural areas, the Northern Sparsely Populated Areas would like to make the following comments: • Promote a place-based approach • Strengthen the link between urban and rural areas • Invest in digital and transport infrastructure • Manage territorial market failures • Support entrepreneurship and innovation capacity in sparsely populated areas • Take advantage of the potential for a green transition Promote a place-based development approach The regional economy in the NSPA area remains vulnerable due certain geographical and structural challenges, such as long distances and sparsely populated areas with aging populations. A lack of critical mass as well as an economy based on natural resources, highly sensitive to global market fluctuations, are severe structural challenges to tackle. At the same time, the regions in the European Arctic delivers added value to the whole of Europe, not least in terms of raw materials. The NSPA regions have great potential to lead the way for a green transition and a sustainable growth, given adapted policies and investments. -

Structure of Earnings 2009
Wages, Salaries and Labour Costs 2011 Structure of Earnings 2009 Growth of earnings was fastest in Satakunta and slowest in Central Ostrobothnia in 2009 Corrected on 7 October 2011. Data on the structure of earnings statistics for the year 2009 have been corrected. In the statistics on private sector hourly wages, the data for 2009 were corrected, which also had an effect on the data on the structure of earnings statistics. The data for 2009 were corrected as concerns monthly salaries and hourly wages. In connection with the correction of the error, the numbers have become slightly revised, because the estimation method was reviewed. The erroneous figures for 2009 have now been corrected to the statistical releases and databases. In 2009, the average monthly earnings were the highest in Uusimaa at EUR 3,285 per month. The regions with the lowest earnings were Etelä-Savo at EUR 2,648 and North Karelia at EUR 2,661. The growth of earnings was fastest in Satakunta at 6.4 per cent from the respective time period of the previous year. Earnings rose most slowly in Central Ostrobothnia where they went up by 1.5 per cent. Helsinki 8.4.2011 Quoting is encouraged provided Statistics Finland is acknowledged as the source. Monthly earnings of employees and pay differentials in the regions in 2009 Region Number Total earnings, EUR / month Mean growth of earnings,% Pay gap Growth of pay gap, % Total 1 387 953 2 971 3,3 2,33 -0,8 01 Uusimaa 475 305 3 285 2,6 2,61 -0,7 02 Varsinais-Suomi 113 585 2 831 3,8 2,23 0,0 04 Satakunta 56 776 2 852 6,4 2,17 0,8 -

Country Information Guide Finland
Country Information Guide Finland A guide to information sources on the Republic of Finland, with hyperlinks to information within European Sources Online and on external websites Contents Information sources in the ESO database .......................................................... 2 General information ........................................................................................ 2 Agricultural information................................................................................... 2 Competition policy information ......................................................................... 2 Culture and language information..................................................................... 2 Defence and security information ..................................................................... 3 Economic information ..................................................................................... 3 Education information ..................................................................................... 3 Employment information ................................................................................. 3 Energy information ......................................................................................... 4 Environmental information .............................................................................. 4 European policies and relations with the European Union .................................... 4 Geographic information and maps ................................................................... -

In Central Ostrobothnia
Lithium Cluster in Central Ostrobothnia A Wide-ranging Opportunity for Mining Companies and Businesses in the Field The Area of the Lithium Province of Central Ostrobothnia is Over 500 Square Kilometres The first indications of a lithium-rich mineral, spodumene, in prospecting work, GTK will continue to conduct an extensive the bedrock of Kaustinen were the boulders found by Arvo survey of lithium potential, covering an area of almost 1,000 Puumala in 1959 at Nikula village. The find sparked wide area square kilometres, based on the analysis of till specimens. The surveys by Suomen Mineraali Oy. This led to locating the Western Finland Office of GTK is also operating in the ”Kaus- Emmes and Jänislampi deposits in Alaveteli along with the tisen seudun litiumvarannot” project (lithium resources in the major Länttä deposit in Ullava. Partek Ltd conducted exten- Kaustinen area) funded by the ERDF. This has partly speeded sive surveys to utilise the deposits, but the world market was up the resource mapping. not in favour of starting lithium production. The Norwegian and Finnish-owned company Keliber Ltd have The Geological Survey of Finland (GTK) has been explored the been researching the lithium resources in the area. The com- lithium resources in the area since 2003. The most significant pany has a mining concession and several claims in the area. new locations found by GTK, Leviäkangas and Syväjärvi, have The company aims to begin mining in the next few years. The been reported to the Ministry of Employment and the Econ- prospects are good since the lithium spodumene resources omy to enable an international tender process. -

Finnish Rescue Services' Pocket Statistics 2013- 2017
D-sarja: Muut [3/2018] Finnish Rescue Services’ Pocket Statistics 2013- 2017 Johannes Ketola, Esa Kokki FINNISH RESCUE SERVICES’ POCKET STATISTICS 2013–2017 CONTENTS 1 INTRODUCTION 1 2 RESCUE SERVICE SYSTEM AND RESOURCES 2 3 ACCIDENT PREVENTION 8 4 RESCUE MISSIONS 12 5 ACCIDENT DAMAGES 30 6 RESCUE OPERATIONS 33 Further Inquiries: Emergency Services College Johannes Ketola, Planning Officer [email protected] Esa Kokki, Director of Research [email protected] prontonet.fi Emergency Services College Publication D-series: Other 3/2018 ISBN: 978-952-7217-08-5 (pdf) ISSN: 2342-9305 pdf 1 INTRODUCTION In Finland, the responsibility for the functions of rescue services is divided between 22 rescue service regions. The rescue services on the Åland Islands are regulated by re- gional legislation. The functions of rescue service regions include accident prevention, rescue operations and civil defence, etc. The pocket statistics is based on the data in the rescue services resource and accident statistics program (PRONTO) from 2013–2017, unless indicated otherwise. PRONTO is maintained by the regional rescue departments. The data in the statistics were gathered directly from PRONTO without a nationwide check. In the statistics rescue operations refer to those incidents when a fire brigade was alerted by an emergency response centre, excluding ambulance service. The number of build- ing fires includes the number of risk of building fires. The data related to rescue operations have been tabulated in PRONTO based on the primary type of an emergency. The secondary types of emergencies have been counted into those tables which deal with accidents, causes for automatic fire calls and property damages.