Antiserotonin Drugs in Migraine Prophylaxis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Anti-Migraine Agents Reference Number: OH.PHAR.PPA.34 Effective Date: 01.01.21 Last Review Date: 11.20 Line of Business: Medicaid
Clinical Policy: Anti-Migraine Agents Reference Number: OH.PHAR.PPA.34 Effective Date: 01.01.21 Last Review Date: 11.20 Line of Business: Medicaid See Important Reminder at the end of this policy for important regulatory and legal information. Description • When using a preferred agent where applicable, the number of tablets/doses allowed per month will be restricted based on the manufacturer’s package insert and/or Buckeye Health plans quantity limits. CNS AGENTS: ANTI-MIGRAINE AGENTS – ACUTE MIGRANE TREATMENT NO PA REQUIRED “PREFERRED” STEP THERAPY REQUIRED PA REQUIRED “NON-PREFERRED” “PREFERRED” NARATRIPTAN (GENERIC OF AMERGE®) NURTEC™ ODT (rimegepant) ALMOTRIPTAN (generic of Axert®) RIZATRIPTAN TABLETS (GENERIC OF CAFERGOT® (ergotamine w/caffeine) MAXALT®) ELETRIPTAN (generic of Relpax®) RIZATRIPTAN ODT (GENERIC OF ERGOMAR® (ergotamine) MAXALT-MLT®) FROVA® (frovatriptan) SUMATRIPTAN TABLETS, NASAL SPRAY, MIGERGOT® (ergotamine w/caffeine) INJECTION (GENERIC OF MIGRANAL® (dihydroergotamine) IMITREX®) ONZETRA™ XSAIL™ (sumatriptan) REYVOW™ (lasmiditan) SUMAVEL DOSEPRO® (sumatriptan) TOSYMRA® (sumatriptan) TREXIMET® (sumatriptan/naproxen) UBRELVY™ (ubrogepant)* ZOLMITRIPTAN (generic of Zomig®) ZOLMITRIPTAN ODT (generic of Zomig ZMT®) ZOMIG® NASAL SPRAY (zolmitriptan) CNS AGENTS: ANTI-MIGRAINE AGENTS – CLUSTER HEADACHE TREATMENT NO PA REQUIRED “PREFERRED” PA REQUIRED “NON-PREFERRED” VERAPAMIL (Generic of Calan®) EMGALITY™ (galcanezumab) VERAPAMIL SR/ER (Generic of Calan SR®, Isoptin SR®, Verelan®) CNS AGENTS: ANTI-MIGRAINE AGENTS – PROPHYLAXIS TREATMENT NO PA REQUIRED “PREFERRED” STEP THERAPY REQUIRED PA REQUIRED “NON-PREFERRED” (Trials of at least 3 controller “PREFERRED” medications) Cardiovascular Agents: Beta-blockers AIMOVIG™ (erenumab-aooe) † EMGALITY™ (galcanezumab) CNS Agents: Anticonvulsants AJOVY™ (fremanezumab-vfrm) * CNS Agents: Serotonin-norepinephrine reuptake inhibitors CNS Agents: Tricyclic antidepressants †Initial Dose is limited to 70mg once monthly; may request dose increase if 70mg fails to provide adequate relief over two consecutive months. -

Evidence for the Involvement of Spinal Cord 1 Adrenoceptors in Nitrous
Anesthesiology 2002; 97:1458–65 © 2002 American Society of Anesthesiologists, Inc. Lippincott Williams & Wilkins, Inc. Evidence for the Involvement of Spinal Cord ␣ 1 Adrenoceptors in Nitrous Oxide–induced Antinociceptive Effects in Fischer Rats Ryo Orii, M.D., D.M.Sc.,* Yoko Ohashi, M.D.,* Tianzhi Guo, M.D.,† Laura E. Nelson, B.A.,‡ Toshikazu Hashimoto, M.D.,* Mervyn Maze, M.B., Ch.B.,§ Masahiko Fujinaga, M.D.ʈ Background: In a previous study, the authors found that ni- opioid peptide release in the brain stem, leading to the trous oxide (N O) exposure induces c-Fos (an immunohisto- 2 activation of the descending noradrenergic inhibitory chemical marker of neuronal activation) in spinal cord ␥-ami- nobutyric acid–mediated (GABAergic) neurons in Fischer rats. neurons, which results in modulation of the pain–noci- 1 In this study, the authors sought evidence for the involvement ceptive processing in the spinal cord. Available evi- Downloaded from http://pubs.asahq.org/anesthesiology/article-pdf/97/6/1458/337059/0000542-200212000-00018.pdf by guest on 01 October 2021 ␣ of 1 adrenoceptors in the antinociceptive effect of N2O and in dence suggests that at the level of the spinal cord, there activation of GABAergic neurons in the spinal cord. appear to be at least two neuronal systems that are Methods: Adult male Fischer rats were injected intraperitone- involved (fig. 1). In one of the pathways, activation of ally with ␣ adrenoceptor antagonist, ␣ adrenoceptor antago- 1 2 ␣ nist, opioid receptor antagonist, or serotonin receptor antago- the 2 adrenoceptors produces either direct presynaptic nist and, 15 min later, were exposed to either air (control) or inhibition of neurotransmitter release from primary af- 75% N2O. -

Lysergic Acid on the Heart of Venus Mercenaria By
Brit. J. Pharmacol. (1962), 18, 440-450. ACTIONS OF DERIVATIVES OF -LYSERGIC ACID ON THE HEART OF VENUS MERCENARIA BY ANNE McCOY WRIGHT, MERILYN MOORHEAD AND J. H. WELSH From the Biological Laboratories, Harvard University, Cambridge, Massachusetts, U.S.A. (Received February 5, 1962) 5-Hydroxytryptamine and a number of (+ )-lysergic acid derivatives have been tested on the heart of Venus mercenaria. One group of derivatives was found to increase the amplitude and frequency of heart beat in a manner much like 5-hydroxy- tryptamine. It included the monoethylamide, diethylamide, propanolamide (ergometrine), butanolamide (methylergometrine) and certain peptide derivatives of lysergic acid without substituents in positions 1 or 2. Of these, lysergic acid diethyl- amide was the most active. Given sufficient time (up to 4 hr), as little as 10 ml. of 10"6 M lysergic acid diethylamide produced a maximum increase in amplitude and frequency in about one-half of the 80 hearts on which it was tested. Its action was very slowly reversed by washing, as was true of all lysergic acid derivatives. A second group of lysergic acid derivatives, substituted in positions 1 or 2, had weak excitor action, if any, and specific 5-hydroxytryptamine blocking action. This group consisted of 1-methyl-, I-acetyl-, and 2-bromo-lysergic acid diethylamide and 1-methyl- lysergic acid butanolamide (methysergide). Of these, the last showed least signs of excitor action, usually none up to 10' M, and it blocked 5-hydroxytryptamine in a molar ratio of about one to one. During the early studies on the pharmacology of the heart of the mollusc, Venus mercenaria, certain of the ergot alkaloids were observed to have a remarkable excitatory action that was only very slowly reversed by washing (Welsh & Taub, 1948). -

Perception of Facial Expressions in Social Anxiety and Gaze Anxiety
The Pegasus Review: UCF Undergraduate Research Journal (URJ) Volume 9 Issue 1 Article 6 2016 Perception of Facial Expressions in Social Anxiety and Gaze Anxiety Aaron Necaise University of Central Florida, [email protected] Part of the Psychology Commons Find similar works at: https://stars.library.ucf.edu/urj University of Central Florida Libraries http://library.ucf.edu This Article is brought to you for free and open access by the Office of Undergraduate Research at STARS. It has been accepted for inclusion in The Pegasus Review: UCF Undergraduate Research Journal (URJ) by an authorized editor of STARS. For more information, please contact [email protected]. Recommended Citation Necaise, Aaron (2016) "Perception of Facial Expressions in Social Anxiety and Gaze Anxiety," The Pegasus Review: UCF Undergraduate Research Journal (URJ): Vol. 9 : Iss. 1 , Article 6. Available at: https://stars.library.ucf.edu/urj/vol9/iss1/6 Necaise: Perception of Facial Expressions Social Anxiety & Gaze Anxiety Published Vol. 9.1: 40-47 October 19th, 2017 THE UNIVERSITY OF CENTRAL FLORIDA UNDERGRADUATE RESEARCH JOURNAL Analysis of the Pathomechanism and Treatment of Migraines Related to the Role of the Neuropeptide CGRP By: Marvi S. Qureshi Faculty Mentor: Dr. Mohtashem Samsam UCF Burnett School of Biomedical Sciences ABSTRACT: Migraines are a type of headache that specifically act on only one side of the head, although about 30% of patients with migraines may experience a bilateral headache. Migraines are brain disorders that typically involve issues of sensory processing taking place in the brainstem. Possible causation has been linked to blood vessels, blood flow, and oxygen levels in the brain. -

Oxytocin Versus Methylergometrine in the Active Management of Third Stage of Labour
Open Journal of Obstetrics and Gynecology, 2014, 4, 666-671 Published Online August 2014 in SciRes. http://www.scirp.org/journal/ojog http://dx.doi.org/10.4236/ojog.2014.411093 Oxytocin versus Methylergometrine in the Active Management of Third Stage of Labour Ajantha Boopathi1*, Sujir Radhakrishnan Nayak2, Arun Rao2, Bharathi Rao2 1Andal Hospital, Cuddalore, India 2Department of Obstetrics and Gynecology, Kasturba Medical College (A Constituent of Manipal University), Mangalore, India Email: *[email protected] Received 19 June 2014; revised 15 July 2014; accepted 10 August 2014 Copyright © 2014 by authors and Scientific Research Publishing Inc. This work is licensed under the Creative Commons Attribution International License (CC BY). http://creativecommons.org/licenses/by/4.0/ Abstract Objective: To compare the efficacy of Oxytocin versus Methylergometrine in active management of third stage of labour in reducing risk of postpartum hemorrhage. Methods: This study was carried out by randomly assigning into two groups with 150 women in each group. Group 1 included pa- tients who received injection Oxytocin 10 IU intramuscular within one minute of the birth of the baby. Injection Methylergometrine (0.2 mg) was given intravenously at the delivery of anterior shoulder of the baby to women in Group 2. Outcome measures were the duration of third stage, blood loss, pre and post-delivery hematocrit, side effects and incidence of PPH. Statistical analysis was done using Chi square test, Fischers test, Mann Whitney test, and t test. p < 0.05 was consi- dered significant. Results: Mean duration of third stage of labour, mean blood loss, post-delivery fall in hematocrit and need for additional uterotonics were significantly less in the Group 2. -

Potential Mechanisms of Prospective Antimigraine Drugs: a Focus on Vascular (Side) Effects
CORE Metadata, citation and similar papers at core.ac.uk Provided by Elsevier - Publisher Connector Pharmacology & Therapeutics 129 (2011) 332–351 Contents lists available at ScienceDirect Pharmacology & Therapeutics journal homepage: www.elsevier.com/locate/pharmthera Associate Editor: John Fozard Potential mechanisms of prospective antimigraine drugs: A focus on vascular (side) effects Kayi Y. Chan a, Steve Vermeersch b, Jan de Hoon b, Carlos M. Villalón c, Antoinette MaassenVanDenBrink a,⁎ a Division of Vascular Medicine and Pharmacology, Department of Internal Medicine, Erasmus Medical Center, P.O. Box 2040, 3000 CA Rotterdam, The Netherlands b Center for Clinical Pharmacology, University Hospitals Leuven, Campus Gasthuisberg, (K.U. Leuven), Leuven, Belgium c Departamento de Farmacobiología, Cinvestav-Coapa, Czda. de los Tenorios 235, Col. Granjas-Coapa, Deleg. Tlalpan, C.P. 14330, México D.F., Mexico article info abstract Available online 2 December 2010 Currently available drugs for the acute treatment of migraine, i.e. ergot alkaloids and triptans, are cranial vasoconstrictors. Although cranial vasoconstriction is likely to mediate—at least a part of—their therapeutic Keywords: effects, this property also causes vascular side-effects. Indeed, the ergot alkaloids and the triptans have been Antimigraine drugs reported to induce myocardial ischemia and stroke, albeit in extremely rare cases, and are contraindicated in Neuropeptides patients with known cardiovascular risk factors. In view of these limitations, novel antimigraine drugs -

The Serotonergic System in Migraine Andrea Rigamonti Domenico D’Amico Licia Grazzi Susanna Usai Gennaro Bussone
J Headache Pain (2001) 2:S43–S46 © Springer-Verlag 2001 MIGRAINE AND PATHOPHYSIOLOGY Massimo Leone The serotonergic system in migraine Andrea Rigamonti Domenico D’Amico Licia Grazzi Susanna Usai Gennaro Bussone Abstract Serotonin (5-HT) and induce migraine attacks. Moreover serotonin receptors play an impor- different pharmacological preventive tant role in migraine pathophysiolo- therapies (pizotifen, cyproheptadine gy. Changes in platelet 5-HT content and methysergide) are antagonist of are not casually related, but they the same receptor class. On the other may reflect similar changes at a neu- side the activation of 5-HT1B-1D ronal level. Seven different classes receptors (triptans and ergotamines) of serotoninergic receptors are induce a vasocostriction, a block of known, nevertheless only 5-HT2B-2C neurogenic inflammation and pain M. Leone • A. Rigamonti • D. D’Amico and 5HT1B-1D are related to migraine transmission. L. Grazzi • S. Usai • G. Bussone (౧) syndrome. Pharmacological evi- C. Besta National Neurological Institute, Via Celoria 11, I-20133 Milan, Italy dences suggest that migraine is due Key words Serotonin • Migraine • e-mail: [email protected] to an hypersensitivity of 5-HT2B-2C Triptans • m-Chlorophenylpiperazine • Tel.: +39-02-2394264 receptors. m-Chlorophenylpiperazine Pathogenesis Fax: +39-02-70638067 (mCPP), a 5-HT2B-2C agonist, may The 5-HT receptor family is distinguished from all other 5- Introduction 1 HT receptors by the absence of introns in the genes; in addi- tion all are inhibitors of adenylate cyclase [1]. Serotonin (5-HT) and serotonin receptors play an important The 5-HT1A receptor has a high selective affinity for 8- role in migraine pathophysiology. -

Current and Prospective Pharmacological Targets in Relation to Antimigraine Action
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Erasmus University Digital Repository Naunyn-Schmiedeberg’s Arch Pharmacol (2008) 378:371–394 DOI 10.1007/s00210-008-0322-7 REVIEW Current and prospective pharmacological targets in relation to antimigraine action Suneet Mehrotra & Saurabh Gupta & Kayi Y. Chan & Carlos M. Villalón & David Centurión & Pramod R. Saxena & Antoinette MaassenVanDenBrink Received: 8 January 2008 /Accepted: 6 June 2008 /Published online: 15 July 2008 # The Author(s) 2008 Abstract Migraine is a recurrent incapacitating neuro- (CGRP1 and CGRP2), adenosine (A1,A2,andA3), glutamate vascular disorder characterized by unilateral and throbbing (NMDA, AMPA, kainate, and metabotropic), dopamine, headaches associated with photophobia, phonophobia, endothelin, and female hormone (estrogen and progesterone) nausea, and vomiting. Current specific drugs used in the receptors. In addition, we have considered some other acute treatment of migraine interact with vascular receptors, targets, including gamma-aminobutyric acid, angiotensin, a fact that has raised concerns about their cardiovascular bradykinin, histamine, and ionotropic receptors, in relation to safety. In the past, α-adrenoceptor agonists (ergotamine, antimigraine therapy. Finally, the cardiovascular safety of dihydroergotamine, isometheptene) were used. The last two current and prospective antimigraine therapies is touched decades have witnessed the advent of 5-HT1B/1D receptor upon. agonists (sumatriptan and second-generation triptans), which have a well-established efficacy in the acute Keywords 5-HT. Antimigraine drugs . CGRP. treatment of migraine. Moreover, current prophylactic Noradrenaline . Migraine . Receptors treatments of migraine include 5-HT2 receptor antagonists, Ca2+ channel blockers, and β-adrenoceptor antagonists. Despite the progress in migraine research and in view of its Introduction complex etiology, this disease still remains underdiagnosed, and available therapies are underused. -

Serotonin Receptor Knockouts: a Moody Subject David Julius* Department of Cellular and Molecular Pharmacology, University of California, San Francisco, CA 94143-0450
Proc. Natl. Acad. Sci. USA Vol. 95, pp. 15153–15154, December 1998 Commentary Serotonin receptor knockouts: A moody subject David Julius* Department of Cellular and Molecular Pharmacology, University of California, San Francisco, CA 94143-0450 The neurotransmitter serotonin (5-hydroxytryptamine; 5-HT) receptors are expressed in a number of brain regions to which is believed to play a significant role in determining one’s serotonergic neurons project, including the hippocampus, ce- emotional state. Indeed, serotonergic synapses are sites of rebral cortex, and amygdala (11, 12). As in the case of action for a number of mood-altering drugs, including the presynaptic autoreceptors, activation of postsynaptic 5-HT1A now-legendary antidepressant Prozac (fluoxetine) (1). As a receptors leads to hyperpolarization of the neuron and the result, there has been tremendous interest in identifying consequent inhibition of neurotransmitter release. This effect molecular components of the serotonergic system, including appears to be mediated through a biochemical signaling path- cell surface receptors and transporters, and understanding way in which 5-HT1A receptors activate a G protein (Gi)- whether and how these proteins contribute to the regulation of coupled inwardly rectifying potassium channel (13, 14). mood and emotion. This quest is driven, in part, by the In light of the pharmacological evidence that 5-HT1A re- possibility that behavioral disorders, such as depression or ceptors exert negative ‘‘feedback’’ control on serotonergic anxiety, may be linked to deficits in one or more components neurons, one would predict that mice lacking this receptor of this signaling system. Such information could, in turn, focus should show elevated levels of extraneuronal serotonin, or an attention on specific targets for the development of novel increase in the amount of serotonin released after nerve drugs with which to treat psychiatric disorders. -
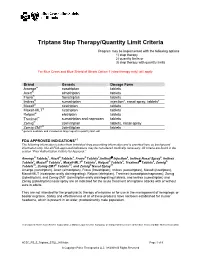
Triptans Step Therapy/Quantity Limit Criteria
Triptans Step Therapy/Quantity Limit Criteria Program may be implemented with the following options 1) step therapy 2) quantity limits or 3) step therapy with quantity limits For Blue Cross and Blue Shield of Illinois Option 1 (step therapy only) will apply. Brand Generic Dosage Form Amerge® naratriptan tablets Axert® almotriptan tablets Frova® frovatriptan tablets Imitrex® sumatriptan injection*, nasal spray, tablets* Maxalt® rizatriptan tablets Maxalt-MLT® rizatriptan tablets Relpax® eletriptan tablets Treximet™ sumatriptan and naproxen tablets Zomig® zolmitriptan tablets, nasal spray Zomig-ZMT® zolmitriptan tablets * generic available and included as target agent in quantity limit edit FDA APPROVED INDICATIONS1-7 The following information is taken from individual drug prescribing information and is provided here as background information only. Not all FDA-approved indications may be considered medically necessary. All criteria are found in the section “Prior Authorization Criteria for Approval.” Amerge® Tablets1, Axert® Tablets2, Frova® Tablets3,Imitrex® injection4, Imitrex Nasal Spray5, Imitrex Tablets6, Maxalt® Tablets7, Maxalt-MLT® Tablets7, Relpax® Tablets8, Treximet™ Tablets9, Zomig® Tablets10, Zomig-ZMT® Tablets10, and Zomig® Nasal Spray11 Amerge (naratriptan), Axert (almotriptan), Frova (frovatriptan), Imitrex (sumatriptan), Maxalt (rizatriptan), Maxalt-MLT (rizatriptan orally disintegrating), Relpax (eletriptan), Treximet (sumatriptan/naproxen), Zomig (zolmitriptan), and Zomig-ZMT (zolmitriptan orally disintegrating) tablets, and Imitrex (sumatriptan) and Zomig (zolmitriptan) nasal spray are all indicated for the acute treatment of migraine attacks with or without aura in adults. They are not intended for the prophylactic therapy of migraine or for use in the management of hemiplegic or basilar migraine. Safety and effectiveness of all of these products have not been established for cluster headache, which is present in an older, predominantly male population. -

(DMT), Harmine, Harmaline and Tetrahydroharmine: Clinical and Forensic Impact
pharmaceuticals Review Toxicokinetics and Toxicodynamics of Ayahuasca Alkaloids N,N-Dimethyltryptamine (DMT), Harmine, Harmaline and Tetrahydroharmine: Clinical and Forensic Impact Andreia Machado Brito-da-Costa 1 , Diana Dias-da-Silva 1,2,* , Nelson G. M. Gomes 1,3 , Ricardo Jorge Dinis-Oliveira 1,2,4,* and Áurea Madureira-Carvalho 1,3 1 Department of Sciences, IINFACTS-Institute of Research and Advanced Training in Health Sciences and Technologies, University Institute of Health Sciences (IUCS), CESPU, CRL, 4585-116 Gandra, Portugal; [email protected] (A.M.B.-d.-C.); ngomes@ff.up.pt (N.G.M.G.); [email protected] (Á.M.-C.) 2 UCIBIO-REQUIMTE, Laboratory of Toxicology, Department of Biological Sciences, Faculty of Pharmacy, University of Porto, 4050-313 Porto, Portugal 3 LAQV-REQUIMTE, Laboratory of Pharmacognosy, Department of Chemistry, Faculty of Pharmacy, University of Porto, 4050-313 Porto, Portugal 4 Department of Public Health and Forensic Sciences, and Medical Education, Faculty of Medicine, University of Porto, 4200-319 Porto, Portugal * Correspondence: [email protected] (D.D.-d.-S.); [email protected] (R.J.D.-O.); Tel.: +351-224-157-216 (R.J.D.-O.) Received: 21 September 2020; Accepted: 20 October 2020; Published: 23 October 2020 Abstract: Ayahuasca is a hallucinogenic botanical beverage originally used by indigenous Amazonian tribes in religious ceremonies and therapeutic practices. While ethnobotanical surveys still indicate its spiritual and medicinal uses, consumption of ayahuasca has been progressively related with a recreational purpose, particularly in Western societies. The ayahuasca aqueous concoction is typically prepared from the leaves of the N,N-dimethyltryptamine (DMT)-containing Psychotria viridis, and the stem and bark of Banisteriopsis caapi, the plant source of harmala alkaloids. -

Diapositiva 1
Characterization of the 5-HT7 receptor as a new therapeutic target for the treatment of pain Àlex Brenchat Barberà ADVERTIMENT. La consulta d’aquesta tesi queda condicionada a l’acceptació de les següents condicions d'ús: La difusió d’aquesta tesi per mitjà del servei TDX (www.tdx.cat) ha estat autoritzada pels titulars dels drets de propietat intel·lectual únicament per a usos privats emmarcats en activitats d’investigació i docència. No s’autoritza la seva reproducció amb finalitats de lucre ni la seva difusió i posada a disposició des d’un lloc aliè al servei TDX. No s’autoritza la presentació del seu contingut en una finestra o marc aliè a TDX (framing). Aquesta reserva de drets afecta tant al resum de presentació de la tesi com als seus continguts. En la utilització o cita de parts de la tesi és obligat indicar el nom de la persona autora. ADVERTENCIA. La consulta de esta tesis queda condicionada a la aceptación de las siguientes condiciones de uso: La difusión de esta tesis por medio del servicio TDR (www.tdx.cat) ha sido autorizada por los titulares de los derechos de propiedad intelectual únicamente para usos privados enmarcados en actividades de investigación y docencia. No se autoriza su reproducción con finalidades de lucro ni su difusión y puesta a disposición desde un sitio ajeno al servicio TDR. No se autoriza la presentación de su contenido en una ventana o marco ajeno a TDR (framing). Esta reserva de derechos afecta tanto al resumen de presentación de la tesis como a sus contenidos.