New Cases of Leprosy in the Cross River Region, Nigeria
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Implementing the Surge Hiv Response in Akwa Ibom an Accelerated Hiv Epidemic Control Drive Content
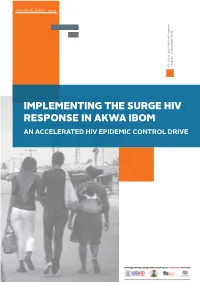
TECHNICAL BRIEF - 2019 A technical guide for local program local program for guide A technical Ibom State... in Akwa managers IMPLEMENTING THE SURGE HIV RESPONSE IN AKWA IBOM AN ACCELERATED HIV EPIDEMIC CONTROL DRIVE CONTENT 1 Understanding the shape of the HIV epidemic in Akwa Ibom 2 Rationale for the surge HIV response 3 Overaching themes of the surge HIV response 4 Community antiretroviral therapy management (CAM) 5 Preimplementation activities 6 The community antiretroviral therapy management team 7 HIV case finding; the fulcrum point of the surge HIV response 8 Linkage to antiretroviral therapy 9 Viral load services in the context of community ART services 10 Coordination and monitoring of CAM services 11 Conclusion 12 Annex TECHNICAL GUIDANCE TECHNICAL GUIDE PAGE 3 UNDERSTANDING THE SHAPE OF THE HIV EPIDEMIC IN AKWA IBOM STATE Fig 1: HIV prevalence in Nigeria (NAIIS 2018) Nigeria has made progress in the fight against HIV/AIDS. The just concluded national AIDS indicator impact survey (NAIIS) revealed that the national Estimated 13,000 new cases prevalence of HIV is 1.4% with an estimated 1.9 million people infected with per year Adolescents 15-19 years the virus. With a mixed epidemic, only 7 out of the 36 states in the country account for 5000 cases % Incidence among cohabiting partners: 1.60 ---- AKAIS account for over 50% of this burden. The top 3 states by burden include Rivers, Benue and Akwa Ibom states. Akwa Ibom state has the highest prevalence in the country at 5.5% with an estimated burden of 178,000 people living with HIV. -

Socioeconomic Development Inequalities Among Geographic Units in Akwa Ibom State, Nigeria Umoren, V
Ethiopian Journal of Environmental Studies and Management Vol. 6 No.3 2013 SOCIOECONOMIC DEVELOPMENT INEQUALITIES AMONG GEOGRAPHIC UNITS IN AKWA IBOM STATE, NIGERIA UMOREN, V. E. http://dx.doi.org/10.4314/ejesm.v6i3.11 Received 12th February 2013; accepted 17th April 2013 Abstract Socio-economic development inequality among geographic units is a phenomenon common in both the developed and developing countries. Regional inequality may result in dissension among geographic units of the same state due to the imbalance in socio-economic development. This study examines the inequality and the pattern in socio-economic development in Akwa Ibom State. Data on socio-economic development indicators was collected using field survey, questionnaire and data from relevant agencies across the 24 areas or nodes selected out of the 31 areas or nodes. The factor analysis technique was applied to the 26 variables to achieve a parsimonious description and identify the major factors to indicate the socio-economic dimensions. From the analysis seven major factors were identified. Factor 1 identified and named as education/communication factor, factor 2 identified and named Health institution/small scale industry factor, factor 3 identified and named as means of transport factor, factor 4 identified and named as land area factor, factor 5 identified and named as distance factor, factor 6 identified and named as income/household size factor and factor 7 identified and named as car ownership factor. The total variance for the factors is 82%. The study revealed that there exist variation and patterns in the socio-economic development in the study area.The pattern shows factor 1 has Essien Udium and Onna indicating high performance .Factor 2 , has 3 areas that indicate high performance Okobo, Ibeno, and Oruk Anam.Factor 3 has 3 areas that indicate high performance Ibesikpo Asutan, Abak and Etinan. -

September 2020 Covid 19 Budget
AKWA IBOM STATE GOVERNMENT MONTHLY COVID-19 BUDGET IMPLEMENTATION REPORT BY ECONOMIC CLASSIFICATION PERIOD: AS AT SEPTEMBER, 2020 YEAR TO DATE FINAL BUDGET Code Name INITIAL BUDGET AMENDMENT SEPTEMBER, 2020 ACTUAL AMOUNT =N= A B C =A+B D E Monthly 33010110 12,000,000.00 0.00 12,000,000.00 Business/Entrepreneurship clinic Opening, grading and 32020202 stabilization of specific 200,000,000.00 0.00 200,000,000.00 approved roads Grading of Roads, Patching of 32020202 Potholes on roads across the 500,000,000.00 (200,000,000.00) 300,000,000.00 state Provision for Margin for 33010121 Increased Cost (Covid 19 Special 6,025,115,880.00 (1,168,761,350.00) 4,856,354,530.00 81,500,000.00 Intervention Fund and Others) Green Brigade(AKS 22021177 Environmental Protection and 1,500,000,000.00 0.00 1,500,000,000.00 Waste Management Agency) Margin for Increased Cost / 22021170 Emergency Provision 7,440,000,000.00 3,824,380,000.00 11,264,380,000.00 100,110,000.00 806,180,000.00 (Subvention) Fumigation of the entire State 22021021 0.00 600,000,000.00 600,000,000.00 20,000,000.00 against COVID 19 Purchase and distribution of 31 32010302 11,000,000.00 0.00 11,000,000.00 No. Palm –oil processing mills Purchase and distribution of 31 32010302 9,000,000.00 0.00 9,000,000.00 No. Cassava processing mills Purchase and distribution of 16 32010302 No. Emel Industrial Sewing 2,189,660.00 0.00 2,189,660.00 machines Purchase of 16 No. -

Development of Road Infrastructure As a Tool of Transforming Ibiono Ibom Local Government Area
53 GLOBAL JOURNAL OF SOCIAL SCIENCES VOL 8, NO. 2, 2009: 53-59 COPYRIGHT© BACHUDO SCIENCE CO. LTD PRINTED IN NIGERIA. ISSN 1596-6216 DEVELOPMENT OF ROAD INFRASTRUCTURE AS A TOOL OF TRANSFORMING IBIONO IBOM LOCAL GOVERNMENT AREA V. UMOREN, E. E. IKUREKONG, A. EMMANUEL AND A.A. UDIDA (Received 25, March 2009; Revision Accepted 18, September 2009) ABSTRACT The need for road infrastructure arises from the fact that there is a greater need for accessibility and smooth movement of abundant agricultural products especially from the rural areas to the markets in urban centres. The improvement of transportation network in the rural area in this regard becomes imperative. This study was conducted to reveal the importance of development of road infrastructure as a panacea for socio-economic advancement in the rural areas. The study area was stratified into three zones i.e Ibiono Central, Ibiono Northern and Ibiono Southern. The Gamma index was used to determine the level of connectivity of each zone in relation to the distribution of socio-economic activity or services in the area. In analysis of the road network connectivity the gamma Index was used. The results indicate a low connectivity, index of 0.26 for zone A, 0.40 for zone B and 0.31 for zone C, in each of the three zones. This implies that there is poor accessibility, poor connectivity, which result in low level of socio-economic activity in the area. The analysis of the socio-economic development variables was carried out based on quality point assigned to the variables. Finally the correlation analysis was employed to determine the relationship between road infrastructure and socio-economic development. -
Projected Population 2007 - 2015
GOVERNMENT OF AKWA IBOM STATE OF NIGERIA PROJECTED POPULATION 2007 - 2015 MINISTRY OF ECONOMIC DEVELOPMENT UYO, AKWA IBOM STATE April, 2014 PREFACE This is the first edition of the publication on the projected population of Akwa Ibom State. It covers the period 2007 – 2015 and gives the projected population of the State by year, sex, residence, age group and Local Government Area. The projection was obtained from 2006 population census figure for Akwa Ibom State using the acceptable growth rate of 3.4 per cent all round. The growth rate was obtained from the National Population Commission, Akwa Ibom State Office, Uyo. The projection was done by staff of the Directorate of Statistics, Ministry of Economic n Development and is based on the Compound Interest Formula, P n = P o + (1 + r) , where; Pn = projected population for year n Po = 2006 population census figure 1 = constant r = population growth rate for Akwa Ibom State n = number of years On behalf of the Permanent Secretary and staff of Ministry of Economic Development, I wish to thank His Excellency, the Executive Governor of Akwa Ibom State, Chief Godswill O. Akpabio (CON), for the love and support to enhance the production of quality and timely statistics in the State. It is hoped that this publication will be useful to politicians, academicians, researchers, Non-Governmental Organizations (NGOs), students, industrialists and the general public in their day-to-day activities. Akan Okon Honourable Commissioner Ministry of Economic Development Akwa Ibom State April, 2014 i TABLE -

HYDROGEOCHEMICAL CHARACTERIZATION of GROUNDWATER in AKWA IBOM STATE, NIGERIA Beka J
Beka J. E_et al., IJSIT, 2014, 3(5),423-435 HYDROGEOCHEMICAL CHARACTERIZATION OF GROUNDWATER IN AKWA IBOM STATE, NIGERIA Beka J. E1, Udom G.J2 and Akpokodje E.G3 1,2,3Department of Geology, University of Port Harcourt, Port Harcourt, Nigeria ABSTRACT Detailed study of the physical and chemical quality analyses of groundwater samples was carried out in Akwa Ibom State in order to delineate aquifers for the drilling of productive boreholes and evaluate the groundwater quality. Detailed analysis of borehole lithologic samples shows a multi-aquifer system, with a sub-regional trend of upper unconfined aquifer and locally restricted subjacent second and third aquifers. The regionally extensive upper unconfined aquifer was logged across boreholes in Abak, Etim Ekpo, Etinan, Ibiono Ibom, Ikono, Ini, Itu, Nsit Atai, Nsit Ibom, Obot Akara, Okobo, Oron, Uruam and Uyo. The depth of this aquifer varies from 10 - 67 meters from coastal to central areas, and 22.5 - 120 meters towards the north.. Thirty two groundwater samples were analyzed for their physico–chemical and microbiological properties, using standard methods. The average temperature of groundwater samples is 27oC. The water is slightly acidic to slightly alkaline with pH values ranging from 4.28 – 8.92. Electrical conductivity (EC) values range from 20.3 µs/cm to 343.1 µs/cm. Chloride contents in some boreholes are up to 31.30 mg/l, possibly indicating saltwater encroachment in those locations (Ibeno, Mbo, Onna and Udung Uko).. Total Dissolved Solids (TDS) range from 12.60 – 147 mg/l. Total Iron (Fe) values range from 0.01 - 8.5 mg/l. -

The Church and Community Development in Nigeria: the Church in Etinan As an Illustration
Research on Humanities and Social Sciences www.iiste.org ISSN (Paper)2224-5766 ISSN (Online)2225-0484 (Online) Vol.4, No.6, 2014 The Church and Community Development in Nigeria: The Church in Etinan as an Illustration Dr. John Arierhi Ottuh Vicar, Winners Baptist Church, P.O. Box 1214, Effurun, Delta State, Nigeria Email: [email protected] Abstract It is not enough to preach the gospel verbally; it must also address human physical and spiritual needs. The Church in Etinan was involved in community development in such a way that the community felt the positive impact of such developments. The church preached the Gospel side by side with physical developments. This act shows that the Gospel the church preached did not only address the spiritual salvation of man but also the physical salvation of man. Etinan is a semi-Urban area in Etinan Local Government Area of Akwa Ibom State. Etinan is the headquarter of the above named Local Government Area. Using the evaluative method, the aim of this study therefore, is to examine the role of the church in community development, using the Church in Etinan as an illustration. Doing this can challenge the contemporary Church in Etinan to follow the stride of community development that has already been laid down as foundation. In order to effectively do this, oral interviews were carried out. Secondary sources were also consulted. It was discovered that Christianity has made socio-religious, educational, political, medical and economic impacts in the development of Etinan community, and it is still capable of doing more in the contemporary times. -

Independent National Electoral Commission (INEC)
FEDERAL REPUBLIC OF NIGERIA Independent National Electoral Commission (INEC) AKWA IBOM STATE DIRECTORY OF POLLING UNITS Revised January 2015 DISCLAIMER The contents of this Directory should not be referred to as a legal or administrative document for the purpose of administrative boundary or political claims. Any error of omission or inclusion found should be brought to the attention of the Independent National Electoral Commission. INEC Nigeria Directory of Polling Units Revised January 2015 Page i Table of Contents Pages Disclaimer.................................................................................. i Table of Contents …………………………………………………. ii Foreword................................................................................... iv Acknowledgement..................................................................... v Summary of Polling Units.......................................................... 1 LOCAL GOVERNMENT AREAS Abak……………………………………………………….….. 2-7 Eastern Obolo………………………………………………... 8-11 Eket……………………………………………………………. 12-17 Esit Eket (Uquo)……………………………………………… 18-21 Essien Udim………………………………………………….. 22-28 Etim Ekpo…………………………………………………….. 29-33 Etinan…………………………………………………………. 34-39 Ibeno………………………………………………………….. 40-43 Ibesikpo Asutan……………………………………………… 44-49 Ibiono Ibom…………………………………………………… 50-57 Ika……………………………………………………………… 58-62 Ikono…………………………………………………………... 63-68 Ikot Abasi……………………………………………………... 69-73 Ikot Ekpene…………………………………………………… 74-79 Ini………………………………………………………………. 80-84 Itu……………………………………………………………… 85-89 Mbo……………………………………………………………. -

The Contributions of Akadep to Food Security in Eket And
British Journal of Education Vol.2, No.4, pp.31-49, September 2014 Published by European Centre for Research Training and Development UK (www.eajournals.org) FOOD SECURITY IN RURAL COMMUNITIES: AN ASSESSMENT OF THE EFFECTIVENESS OF GOVERNMENT INTERVENTION IN EKET AND ONNA LOCAL GOVERNMENT AREAS OF AKWA IBOM STATE, NIGERIA. 1989-2010 Ekaette Umanah EKONG ABSTRACT: This study examines the agricultural projects initiated by AKADEP in its effort at achieving food security in the two local government areas under study. It takes a close look at its objectives, goals, achievements and challenges and assesses the problems that have militated against the successful realization of AKADEP projects 24 years after its inception. The study posits that women who make up over 75 percent of the farmers in these communities have been largely ignored by policy makers. Limited access to land, proliferation of very small land holdings along with the traditional land tenure system (leaving large portions of arable land fallow for several years) have conspired to negate meaningful agricultural development. Besides, poor entrepreneurial skills of 90 percent of the farmers interviewed, poor funding of agricultural development projects, incoherent government policies, insincerity on the part of government at all levels and a clear distrust of government intentions by farmers all threaten food security in these rural areas. KEYWORDS: Onna, Eket, Akadep (Akwa Ibom Agricultural Development Programme) INTRODUCTION In the last five decades, successive governments at the federal level have increasingly assigned the agricultural sector an ambitions role in its strategic planning frameworks. Virtually all the strategic development documents for national development and poverty alleviation in Nigeria and efforts to jump-start the economy on the path to success have always had agriculture at its nerve-centre. -

A Study of Access to Sanitation Profiles of Rural Upland and Coastal Communities of Akwa Ibom State, Nigeria
DOI: https://dx.doi.org/10.4314/gjpas.v23i2.1 GLOBAL JOURNAL OF PURE AND APPLIED SCIENCES VOL. 23, 2017: 207-212 COPYRIGHT© BACHUDO SCIENCE CO. LTD PRINTED IN NIGERIA ISSN 1118-0579 207 www.globaljournalseries.com , Email: [email protected] A STUDY OF ACCESS TO SANITATION PROFILES OF RURAL UPLAND AND COASTAL COMMUNITIES OF AKWA IBOM STATE, NIGERIA A. J. OKON, M. E. EJA AND R. E. KALU (Received 24 March 2017; Revision Accepted 23 June 2017) ABSTRACT In developing countries, e.g., Nigeria, several communities have limited access to sanitation and sanitation facilities, thus such communities dump their solid and liquid wastes indiscriminately. The aim of this study was to assess access to sanitation, and compare basic sanitation facilities between upland and coastal communities of Akwa Ibom State. With a cross-sectional design, 420 respondents were selected and administered questionnaires to obtain information on sanitation and sanitation facilities of the communities using a multi-stage random sampling technique. Result shows that faecal disposal facilities available for upland and coastal communities were respectively 187(89.05%) and 98(46.67%). 30(26.79%) of households defecate in open bodies of water in the coastal areas, while upland communities do not. Also, 9(39.13%) and 64(57.14%) of upland and coastal areas respectively, defecate in bushes/swamps, while 14(60.87%) and 18(16.07%) bury their faeces in pits. On the whole, improved sanitation coverage recorded 61.90% and 38.10% respondents for the rural upland and coastal communities respectively, while unimproved sanitation coverage for upland and coastal communities recorded 31.43% and 68.57% respectively. -
Jaja-Ibeno War of 1881: the Ibeno Account and the Refugee Settlements (Pp
An International Multi-Disciplinary Journal, Ethiopia Vol. 3 (2), January, 2009 ISSN 1994-9057 (Print) ISSN 2070-0083 (Online) Jaja-Ibeno War of 1881: The Ibeno Account and the Refugee Settlements (Pp. 119-133) J. H. Enemugwem - Department of History and Diplomatic Studies, Faculty of Humanities, University of Port Harcourt, Port Harcourt, Nigeria [email protected] Abstract This essay deliberates on the Ibeno account and refugee settlements of the Jaja-Ibeno War of 1881 which was untouched by the previous researchers. Its contributions include the causes and course of the war, the mercenaries hired by King Jaja of Opobo, the casualties and entreaties such as the deaths of the Ibeno monarch: King Uko Utong and his son Prince Nso, Jaja’s rehabilitation of the Ibeno to prevent another war and the refugee camps. The need to give this history a balanced view made the paper to analyze the Ibeno relationship with Opobo and Jaja’s establishment of his kingdom in Obolo (Andoni) country which led to his intrusion in the Kwa Ibo palm produce trade. Keywords: Conflict, European trade, Opobo, Ibeno, impact, Refugee Settlements Introduction There are copious literatures on the Atlantic Trade and the Jaja-Ibeno War of 1881. Dike (1956) gave the fact that Atlantic Trade started with human cargo from 1400 to 1700. This was when Europe explored the Americas for sugar, cotton and coffee and needed enormous work force. Although Dike touched Copyright: IAARR, 2009 www.afrrevjo.com 119 Indexed African Journals Online: www.ajol.info African Research Review Vol. 3 (2), January, 2009. Pp. 119-133 on the Jaja-Ibeno War, he neither considers the Ibeno version nor the refugee settlements. -
STRENGTHENING the AKWA IBOM HEALTH SYSTEM for Improved HIV Response
STRENGTHENING THE AKWA IBOM HEALTH SYSTEM for improved HIV response The PEPFAR/USAID-funded Program to Build Leadership and Accountability in Nigeria’s Health System (PLAN-Health), managed by Management Sciences for Health (MSH), is a five year project (2010 – 2015) aimed to strengthen the institutional capacity, leadership, and management skills of public sector institutions and civil society organizations for better HIV/AIDS and other health services delivery to vulnerable groups in Nigeria. STRENGTHENING THE AKWA IBOM HEALTH SYSTEM FOR IMPROVED HIV RESPONSE HIV: A CRITICAL SITUATION IN AKWA IBOM STATE kwa Ibom State located in Nigeria’s Niger Delta, in the coastal south of the country, has a population of 3,920,051.1 Created in 1987, it is A made up of 31 Local Government Areas (LGAs). Akwa Ibom ranks six out of Nigeria’s 36 states for the highest number of people living with HIV. The 2012 National AIDS and Reproductive Health Survey showed the state as having a prevalence rate of 6.5%, which is higher than the national prevalence rate of 3.4%. The maternal mortality rate is 77 per 100,000 live births2 and infant mortality is 72 per 1,000 live births.2, 3 Minimal use of antenatal care (ANC) services by pregnant women and deliveries outside the formal sector are contributing factors. Available data indicate that 57.2% of pregnant women attend 4 or more ANC sessions while only 39.7% deliveries are attended by skilled birth attendants.2 Figure 1: Map of Akwa Ibom State Ini Obot Ikono Akara Ibiono Ikot Ibom Ekpene Itu Essien Udim Uruan Abak Ika Uyo Etim Ekpo Ibesikpo Asutan Okobo Ukanafun Nsit Ibom Nsit Atai Orukanam Etinan Oron Nsit Ubium Mkpat Udung Uko Enin Urue Oong Oruko Esit Eket Ikot Abasi Eket Mbo Onna Ibeno Eastern Obolo 1 National Census figure.