Traditional Practices and Perceptions of Epilepsy Among People in Roma Communities in Bulgaria
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Town of Zlatitsa
Town of Zlatitsa The Clock Tower The Town Centre ZLATITSA MUNICIPALITY – SPIRITUAL, EDUCATIONAL, SPORTS, ENTERTAINMENT AND COMMERCIAL CENTRE OF THE SREDNOGORIE REGION, AIMING TO ACHIEVE ECONOMIC AND ENVIRONMENTAL SUSTAINABILITY AND SOCIAL JUSTICE FOR ALL ITS CITIZENS. Zlatitsa is situated in the Zlatitsa-Pirdop Hollow. To the north of it stretch the Southern slopes of the Balkan Mountain Range and the far-most village of Petrich rests in the nothern parts of Ihtimanska and Sashtinska Sredna Gora mountains. It neighbor the municipalities of Pirdop,Chavdar, Chelopech,Mirkovo and Etropole.. Zlatitsa Municipality covers three villages – Karlievo, Tsarkvishte and Petrich. The totalpopulation in them is 725 people. Half of them are involved in plant growing and animal raising. They either sell their agricultural produce or use it themselves. Most of these farmers act as sole traders and don’t associate due to the higher risks about it. Tsarkvishte Karlievo Petrich The town of Zlatitsa is set in a boundlessly beautiful and interesting natural environment. Despite the fact that there are three active industrial plants nearby, the air is relatively clean. Most of the town’s sights of interest are natural, like Spasovoto Kladenche – a water fountain in the Balkan Mountain north of Zlatitsa. That is where in a bloody fight with Turkish invaders at the end of 14 c. A.D. Spas Voyvoda, the last defender of Zlatitsa, was killed. It is him that the area was named after. The region is characterized by a favourable geographical setting and climate, beautiful natural and cultural heritage. The municipality provides excellent conditions for the development of agriculture: • In Zlatitsa large • The villages within quantities of good-quality Zlatitsa municipality farming produce are include large areas of grown. -

Annex REPORT for 2019 UNDER the “HEALTH CARE” PRIORITY of the NATIONAL ROMA INTEGRATION STRATEGY of the REPUBLIC of BULGAR
Annex REPORT FOR 2019 UNDER THE “HEALTH CARE” PRIORITY of the NATIONAL ROMA INTEGRATION STRATEGY OF THE REPUBLIC OF BULGARIA 2012 - 2020 Operational objective: A national monitoring progress report has been prepared for implementation of Measure 1.1.2. “Performing obstetric and gynaecological examinations with mobile offices in settlements with compact Roma population”. During the period 01.07—20.11.2019, a total of 2,261 prophylactic medical examinations were carried out with the four mobile gynaecological offices to uninsured persons of Roma origin and to persons with difficult access to medical facilities, as 951 women were diagnosed with diseases. The implementation of the activity for each Regional Health Inspectorate is in accordance with an order of the Minister of Health to carry out not less than 500 examinations with each mobile gynaecological office. Financial resources of BGN 12,500 were allocated for each mobile unit, totalling BGN 50,000 for the four units. During the reporting period, the mobile gynecological offices were divided into four areas: Varna (the city of Varna, the village of Kamenar, the town of Ignatievo, the village of Staro Oryahovo, the village of Sindel, the village of Dubravino, the town of Provadia, the town of Devnya, the town of Suvorovo, the village of Chernevo, the town of Valchi Dol); Silistra (Tutrakan Municipality– the town of Tutrakan, the village of Tsar Samuel, the village of Nova Cherna, the village of Staro Selo, the village of Belitsa, the village of Preslavtsi, the village of Tarnovtsi, -

1 I. ANNEXES 1 Annex 6. Map and List of Rural Municipalities in Bulgaria
I. ANNEXES 1 Annex 6. Map and list of rural municipalities in Bulgaria (according to statistical definition). 1 List of rural municipalities in Bulgaria District District District District District District /Municipality /Municipality /Municipality /Municipality /Municipality /Municipality Blagoevgrad Vidin Lovech Plovdiv Smolyan Targovishte Bansko Belogradchik Apriltsi Brezovo Banite Antonovo Belitsa Boynitsa Letnitsa Kaloyanovo Borino Omurtag Gotse Delchev Bregovo Lukovit Karlovo Devin Opaka Garmen Gramada Teteven Krichim Dospat Popovo Kresna Dimovo Troyan Kuklen Zlatograd Haskovo Petrich Kula Ugarchin Laki Madan Ivaylovgrad Razlog Makresh Yablanitsa Maritsa Nedelino Lyubimets Sandanski Novo Selo Montana Perushtitsa Rudozem Madzharovo Satovcha Ruzhintsi Berkovitsa Parvomay Chepelare Mineralni bani Simitli Chuprene Boychinovtsi Rakovski Sofia - district Svilengrad Strumyani Vratsa Brusartsi Rodopi Anton Simeonovgrad Hadzhidimovo Borovan Varshets Sadovo Bozhurishte Stambolovo Yakoruda Byala Slatina Valchedram Sopot Botevgrad Topolovgrad Burgas Knezha Georgi Damyanovo Stamboliyski Godech Harmanli Aitos Kozloduy Lom Saedinenie Gorna Malina Shumen Kameno Krivodol Medkovets Hisarya Dolna banya Veliki Preslav Karnobat Mezdra Chiprovtsi Razgrad Dragoman Venets Malko Tarnovo Mizia Yakimovo Zavet Elin Pelin Varbitsa Nesebar Oryahovo Pazardzhik Isperih Etropole Kaolinovo Pomorie Roman Batak Kubrat Zlatitsa Kaspichan Primorsko Hayredin Belovo Loznitsa Ihtiman Nikola Kozlevo Ruen Gabrovo Bratsigovo Samuil Koprivshtitsa Novi Pazar Sozopol Dryanovo -

Local Initiatives in the Period 1999 – 2000
LOCAL INITIATIVES IN THE PERIOD 1999 2000 SOFIA DECEMBER 1999 LOCAL INITIATIVES IN THE PERIOD 1999 - 2000 2 CONTENTS 1. PRINCIPLES OF COOPERATION WITH LOCAL GOVERNMENT ................................................................. 3 2. SPHERES AND FORMS OF COOPERATION ............ 4 3. LOCAL PARTNERS OF COALITION 2000 .................. 7 4. INTERACTION WITH OTHER NON-GOVERNMENTAL ORGANIZATIONS AND INITIATIVES .............................................................. 8 LOCAL INITIATIVES IN THE PERIOD 1999 - 2000 3 1. PRINCIPLES OF COOPERATION WITH LOCAL GOVERNMENT Coalition 2000 will continue its activities on both national and regional/ local level. Realizing that administrative corruption is the kind citizens encounter in their everyday lives, the Coalition will place special empha- sis on interaction with the representatives of local government and the other municipal agencies for enhancing the transparency in the sphere of public services. The common interests of civil society and local govern- ment allow expanding the scope of the cooperation initiated in the pilot stage of the local projects. One precondition for successful advancement in this direction is fostering a climate of dialogue and trust between the two sectors. This implies consistent efforts by both sides, as well as profes- sionalism and resolve. Openness and Transparency of Public Administration The information the public is entitled to, either by law or by the force of the existing statutes and regulations, is often left behind the curtain of the discretion of public officials. Nor is there any sufficiently sustained civil effort to lift this curtain and shed light on the gray zones of the decision- making mechanisms. The task should therefore be to launch a continuous dialogue between public institutions and civil organizations for the attain- ment of European standards of openness and accountability. -

Guide to 2003 SEG Bulgarian Field Trip
Society of Economic Geologists Guidebook Series, Volume 36, 2003 References – Guide to 2003 S.E.G. Bulgarian Field Trip Aiello, E., Bartolini, C., Boccaletti, M., Gochev, P., Karagjuleva, J., Kostadinov, V., and Manneti, P., 1977. Sedimentary features of Srednogorie zone (Bulgaria), an Upper Cretaceous intra arc basin. Sedim. Geol., v. 19, p. 39–68. Amov, B., 1999, Lead isotope data for ore deposits from Bulgaria and the possibility for their use in archaeometry. Berliner Beiträge zur Archäometrie, 16, 5–19. Amov, B., and Valkova, V., 1994, Generalized data on the isotope composition of lead in ore deposits on the territory of Bulgaria. in: Problems of the earliest metallurgy, Publ. Of MGU, No 4, p. 122–138, (in Bulgarian). Amov, B., Bogdanov, B., and Baldjieva, T., 1974, Lead isotope composition and some features concerning the genesis and the age of the ore deposits in south Bulgaria, in: Bogdanov, B., ed., Problems of Ore Deposition, Proc. 4th IAGOD Symp., v. 2, p. 13–25, (in Russian). Andrew, C., 1997, The geology and genesis of the Chelopech Au-Cu deposit, Bulgaria: Europoe’s largest gold resource. in: Harney, S. (ed.), Europe’s Major Gold Deposits, Abstracts volume, Newcastle, Northern Ireland. Irish Association for Economic Geology, p. 68–72. Angelkov, K., 1973, Geological and structural factors of formation of the copper deposit Assarel. in: 20 years of the Higher Mining and Geological Institute, v. 20, p. 94–102 (in Bulgarian). ——1974, Ore formation and sulphur isotope composition of the deposits in Panagyurishte ore region (Russian), in: Bogdanov, B., ed., Problems of Ore Deposition, Proc. -

(Jurassic) of North Bulgaria. III. Tithonian Dinoflagellate Cysts Lilia Dodekova
GEOLOGICA BALCANICA, 24, 5, Sofia, Oct. 1994, p. li-4G Dinoflagellate cysts from the Bathonian - Tithonian (Jurassic) of North Bulgaria. III. Tithonian dinoflagellate cysts Lilia Dodekova Geological Institute, Bulgarian Academy of Sciences, 1113 Sofia (Received 14 . Ofi. 1994; accrpted 1fi. 06. 1991) JJ. JloileKoaa - Lf.ucmht iJuHotp,zai!eAAam 6ama - mumoHa ( 10pa) a Ceoe pHoii DOAi!apuu . Ill. TaKco ltOAtUJ! /llU/IlOHCKIIX !{UC/Il UUHOt/JAazeAAam. J1cc,1e)lOBaHbl )lHIWUHCTbl THTOI!CKHX MOpCKHX OTJ!Oll<eHHI1 00 pa3pe3aM 34 IIe4JT51HbiX CKBalKHH H O,liHO eCTeCTBeiiOe 06I·Ia>KefiHe. 06HapylKCiibl 6oraTble II '13CTO XOpOWO COXpaHHBWIICCH KO ~ Jn JieKCbl JlHHOUHCT . 8 CT3Tbe Jtaiii>I KOpOTKHe CBe,lleHHH 0 MOfHjJOJ!Oriii!, T3KCOHOMHH, reorpa4JHlJCCKOM H CTp3THfpa4JH'leCK0~1 pacnpOCTp aiieHHH 56 T3K CO IIOIJ JlHIIOUHCT H 2 BH· JlOB aKpHrapx. Bee OHH noHBJ151IOTC51 B THTOHCKOM Hpyce . H OBble TaKCOHbl OriHCaHH bie 6oJJee )leTaJlbHO BKJJIO<JaiOT: Semicauidinium gen . n., S. mitra (D ii r r) comb. n., Amphorula monteiliae sp. n ., Cassi culosphaeridia cribrosa sp. n ., Kallosplweridium callosum sp. n ., Prolixosphaeridium? foratum sp . n ., Prolixosphaeridittm perforospineum sp. n ., Sentusidinium spatiosum sp. n ., Systematophora jubifera sp. n., Systematophora? prodigiosa sp. n., Pareodinia pauca sp . n. , Gonyaulacysta vesicula sp. n ., Lep todinium? ambiguiformis sp. n ., Leptodinium? plagatam sp . n., Pyxidinopsis? retiolum sp. n. YKa3auo crparHrpacjJH'IeCK oe pacnpocrpaHeHHe B DOJJrapHH ynmHIHYTI>IX AHHOUHCT ll ~tecrc c nepeXOJlHbniH raKCoHaMH . Ouu ycraHOBJleHHbl B II JJHrocrpaTHrpacjJH<JeCKIIX CJlHHHUax . :=ITo uccJJeJlOIJa iiiie }lonoJJ HHeT H03113IIHC KOM HJleKCOil JlHIIOUHCT TeTHCa ll KOHUe IOfJI.ol H 113 rpaHIIUe !Op a - ~teJJa. Abstract. Tithonian marine sediments from 34 boreholes and one outcrop in North Bulgaria have been palynologically examined. -
A G R O S T a T I S T I
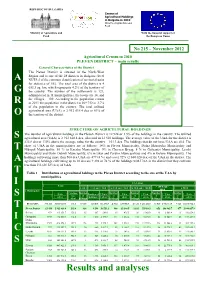
REPUBLIC OF BULGARIA Census of Agricultural Holdings in Bulgaria in 2010 Ministry of Agriculture and Food Ministry of Agriculture and With the financial support of Food the European Union No 215 – November 2012 2010 2020020052005 Agricultural Census in 2010 PLEVEN DISTRICT – main results General Characteristics of the District The Pleven District is situated in the North-West Region and is one of the 28 districts in Bulgaria (level A NUTS 3 of the common classification of territorial units for statistics of EU). The total area of the district is 4 653.3 sq. km, which represents 4.2% of the territory of G the country. The number of the settlements is 123, administered in 11 municipalities, the towns are 14, and the villages – 109. According to the population census R in 2011 the population in the district is 269 752 or 3.7% of the population in the country. The total utilized agricultural area (UAA) is 2 912 618.4 dca or 63% of O the territory of the district. STRUCTURE OF AGRICULTURAL HOLDINGS The number of agricultural holdings in the Pleven District is 12 924 or 3.5% of the holdings in the country. The utilized S agricultural area (UAA) is 2 912 618.4 dca, allocated in 12 510 holdings. The average value of the UAA for the district is 232.8 dca or 130% above the average value for the country – 101.3 dca. The holdings that do not have UAA are 414. The share of UAA in the municipalities are as follows: 14% in Pleven Municipality, Dolna Mitropolia Municipality and T Nikopol Municipality, 10 % in Knezha Municipality, 9% in Cherven Bryag, 8 % in Gulyantsi Municipality, Levski Municipality and Dolni Dabnik Municipality, 6% in Iskar and Pordim Municipalities and 4% in Belene Municipality. -

Appendix 1 D Municipalities and Mountainous
National Agriculture and Rural Development Plan 2000-2006 APPENDIX 1 D MUNICIPALITIES AND MOUNTAINOUS SETTLEMENTS WITH POTENTIAL FOR RURAL TOURISM DEVELOPMENT DISTRICT MUNICIPALITIES MOUNTAINOUS SETTLEMENTS Municipality Settlements* Izgrev, Belo pole, Bistrica, , Buchino, Bylgarchevo, Gabrovo, Gorno Bansko(1), Belitza, Gotze Delchev, Garmen, Kresna, Hyrsovo, Debochica, Delvino, Drenkovo, Dybrava, Elenovo, Klisura, BLAGOEVGRAD Petrich(1), Razlog, Sandanski(1), Satovcha, Simitly, Blagoevgrad Leshko, Lisiia, Marulevo, Moshtanec, Obel, Padesh, Rilci, Selishte, Strumiani, Hadjidimovo, Jacoruda. Logodaj, Cerovo Sungurlare, Sredets, Malko Tarnovo, Tzarevo (4), BOURGAS Primorsko(1), Sozopol(1), Pomorie(1), Nesebar(1), Aitos, Kamenovo, Karnobat, Ruen. Aksakovo, Avren, Biala, Dolni Chiflik, Dalgopol, VARNA Valchi Dol, Beloslav, Suvorovo, Provadia, Vetrino. Belchevci, Boichovci, Voneshta voda, Vyglevci, Goranovci, Doinovci, VELIKO Elena, Zlataritsa, Liaskovets, Pavlikeni, Polski Veliko Dolni Damianovci, Ivanovci, Iovchevci, Kladni dial, Klyshka reka, Lagerite, TARNOVO Trambesh, Strajitsa, Suhindol. Tarnovo Mishemorkov han, Nikiup, Piramidata, Prodanovci, Radkovci, Raikovci, Samsiite, Seimenite, Semkovci, Terziite, Todorovci, Ceperanite, Conkovci Belogradchik, Kula, Chuprene, Boinitsa, Bregovo, VIDIN Gramada, Dimovo, Makresh, Novo Selo, Rujintsi. Mezdra, Krivodol, Borovan, Biala Slatina, Oriahovo, VRATZA Vratza Zgorigrad, Liutadjik, Pavolche, Chelopek Roman, Hairedin. Angelov, Balanite, Bankovci, Bekriite, Bogdanchovci, Bojencite, Boinovci, Boicheta, -

Priority Public Investments for Wastewater Treatment and Landfill of Waste
Environmentally and Socially Sustainable Develonment Europe and Central Asia Region 32051 BULGARIA Public Disclosure Authorized ENVIRONMENTAL SEQUENCING STRATEGIES FOR EU ACCESSION PriorityPublic Investments for Wastewater Treatment and Landfill of Waste *t~~~~~~~~~~~~~~~~~~~~~~~ Public Disclosure Authorized IC- - ; s - o Fk - L - -. Public Disclosure Authorized The World Bank Public Disclosure Authorized May 2004 - "Wo BULGARIA ENVIRONMENTAL SEQUENCING STRATEGIES FOR EU ACCESSION Priority Public Investments for Wastewater Treatment and Landfill of Waste May 2004 Environmentally and Socially Sustainable Development Europe and Central Asia Region Report No. 27770 - BUL Thefindings, interpretationsand conclusions expressed here are those of the author(s) and do not necessarily reflect the views of the Board of Executive Directors of the World Bank or the governments they represent. Coverphoto is kindly provided by the external communication office of the World Bank County Office in Bulgaria. The report is printed on 30% post consumer recycledpaper. TABLE OF CONTENTS Acknowledgements ..................................................................... i Abbreviations and Acronyms ..................................................................... ii Summary ..................................................................... iiM Introduction.iii Wastewater.iv InstitutionalIssues .xvi Recommendations........... xvii Introduction ...................................................................... 1 Part I: The Strategic Settings for -

Health Insurance Actpdf / 7.08 MB
Health Insurance Act Promulgated, State Gazette No. 70/19.06.1998, amended, SG No. 93/11.08.1998, SG No. 153/23.12.1998, effective 1.01.1999, SG No. 62/9.07.1999, SG No. 65/20.07.1999, amended and supplemented, SG No. 67/27.07.1999, effective 28.08.1999, amended, SG No. 69/3.08.1999, effective 3.08.1999, amended and supplemented, SG No. 110/17.12.1999, effective 1.01.2000, SG No. 113/28.12.1999, SG No. 64/4.08.2000, effective 1.10.2001, supplemented, SG No. 41/24.04.2001, effective 24.04.2001, amended and supplemented, SG No. 1/4.01.2002, effective 1.01.2002, SG No. 54/31.05.2002, effective 1.12.2002, supplemented, SG No. 74/30.07.2002, effective 1.01.2003, amended and supplemented, SG No. 107/15.11.2002, supplemented, SG No. 112/29.11.2002, amended and supplemented, SG No. 119/27.12.2002, effective 1.01.2003, amended, SG No. 120/29.12.2002, effective 1.01.2003, amended and supplemented, SG No. 8/28.01.2003, effective 1.03.2003, supplemented, SG No. 50/30.05.2003, amended, SG No. 107/9.12.2003, effective 9.12.2003, supplemented, SG No. 114/30.12.2003, effective 1.01.2004, amended and supplemented, SG No. 28/6.04.2004, effective 6.04.2004, supplemented, SG No. 38/11.05.2004, amended and supplemented, SG No. 49/8.06.2004, amended, SG No. 70/10.08.2004, effective 1.01.2005, amended and supplemented, SG No. -

Electoral Geography and Sustainable Regional Development in Bulgaria: Case Study of North�West Bulgaria and Vidin District
Geographica Timisiensis, vol. 19, nr. 1, 2010 (pp. 155-162) ● ELECTORAL GEOGRAPHY AND SUSTAINABLE REGIONAL DEVELOPMENT IN BULGARIA: CASE STUDY OF NORTH-WEST BULGARIA AND VIDIN DISTRICT Marin ROUSSEV Faculty of Geology and Geography, Sofia University “St. Kliment Ohridski”, Bulgaria Abstract : The transition to sustainable development depends on political factors, concerning regional disproportions, principles of regional policy and local self-government. They are dependent on the electoral behavioral models in society. The change of social conditions in Bulgaria demands an actualization of research methods and indicators so that territorial division is optimized. Electoral geography has a great potential for such actualization. Main operative statistical units in this study are the administrative regions and municipalities as well as their macroelectoral compounding. This approach is combined with the correlative-typological potential of the “geographic passport” method. It is used for the derivation of traditional electoral types of administrative units and macroelectoral regions. Their characteristics are distinguished by clearly expressed dependencies between natural and social features on the one hand and electoral behavioral models, on the other hand. The North- West region is characterized by an unfavorable combination of natural potential and negative social tendencies – broken age structure, negative migration balance, low economic activity and agricultural specialization. This economic basis is combined with a left political orientation. The most typical example for this is the Vidin district. During the last 2-3 years there are social tendencies which lead to the assumption that Bulgaria is entering a new electoral cycle that is to replace the post communist governmental model of the last two decades. -

Decision No 129 of 5 March 2009 on the Opening of a Procedure for Granting of Authorisation for Prospecting and Exploration Of
C 118/4 EN Official Journal of the European Union 27.5.2009 PROCEDURES RELATING TO THE IMPLEMENTATION OF THE COMPETITION POLICY COMMISSION DECISION No 129 of 5 March 2009 on the opening of a procedure for granting of authorisation for prospecting and exploration of oil and gas — underground natural resources in accordance with Article 2(1)(3) of the Underground Natural Resources Act, at Block 1-6 ‘Pelovo’, located in the province of Pleven and notification concerning the envisaged competition for granting of authorisation (2009/C 118/04) REPUBLIC OF BULGARIA COUNCIL OF MINISTERS Pursuant to Article 5(2), Article 42(1)(1) and Article 44(3) of the Underground Natural Resources Act, and having regard to Article 4(2)(16) and Article 1(24a) of the Energy Act, THE COUNCIL OF MINISTERS HAS DECIDED: 1. to open a procedure for granting authorisation for prospecting and exploration of crude oil and natural gas in Block 1-6 ‘Pelovo’, with a surface area of 615,08 km 2 and with coordinates of the boundaries 1 to 20 in accordance with the Annex. The concession areas ‘Dolni Dabnik’, ‘Gorni Dabnik’, ‘Dolni Lukovit’ and ‘Staroseltsi’ shall be excluded from the prospecting and exploration area; 2. to announce that the granting of authorisation pursuant to point 1 will be based on a competition; 3. to specify that the period covered by the authorisation for prospecting and exploration will be five years after the date of the entry into force of the prospecting and exploration contract, with a right to extension of this period pursuant to Article 31(3) of the Underground Natural Resources Act; 4.