Relations Between Age, Autism Severity, Behavioral Treatment and the Amount of Time in Regular Education Classrooms Among Students with Autism
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
An Exploration of the Rapid Prompting Method for Students with Autism Shea Manship James Madison University
James Madison University JMU Scholarly Commons Senior Honors Projects, 2010-current Honors College Spring 2018 An exploration of the Rapid Prompting Method for students with autism Shea Manship James Madison University Follow this and additional works at: https://commons.lib.jmu.edu/honors201019 Part of the Educational Methods Commons, and the Special Education and Teaching Commons Recommended Citation Manship, Shea, "An exploration of the Rapid Prompting Method for students with autism" (2018). Senior Honors Projects, 2010-current. 573. https://commons.lib.jmu.edu/honors201019/573 This Thesis is brought to you for free and open access by the Honors College at JMU Scholarly Commons. It has been accepted for inclusion in Senior Honors Projects, 2010-current by an authorized administrator of JMU Scholarly Commons. For more information, please contact [email protected]. An Exploration of the Rapid Prompting Method for Students with Autism _______________________ An Honors College Project Presented to the Faculty of the Undergraduate College of Education James Madison University _______________________ by Shea Colleen Manship May 2018 Accepted by the faculty of the Department of Educational Foundations and Exceptionalities, James Madison University, in partial fulfillment of the requirements for the Honors College. FACULTY COMMITTEE: HONORS COLLEGE APPROVAL: Project Advisor: Tiara S. Brown, Ph.D. Bradley R. Newcomer, Ph.D., Assistant Professor, Department of Dean, Honors College Educational Foundations and Exceptionalities Reader: Mira C. Williams, Ph.D. Assistant Professor, Department of Educational Foundations and Exceptionalities Reader: Keri S. Bethune, Ph.D., BCBA-D Associate Professor, Department of Educational Foundations and Exceptionalities PUBLIC PRESENTATION This work is accepted for presentation, in part or in full, at the James Madison Honors Symposium on April 18, 2018. -

The Persistence of Fad Interventions in the Face of Negative Scientific Evidence: Facilitated Communication for Autism As a Case Example
Evidence-Based Communication Assessment and Intervention ISSN: 1748-9539 (Print) 1748-9547 (Online) Journal homepage: http://www.tandfonline.com/loi/tebc20 The persistence of fad interventions in the face of negative scientific evidence: Facilitated communication for autism as a case example Scott O. Lilienfeld, Julia Marshall, James T. Todd & Howard C. Shane To cite this article: Scott O. Lilienfeld, Julia Marshall, James T. Todd & Howard C. Shane (2014) The persistence of fad interventions in the face of negative scientific evidence: Facilitated communication for autism as a case example, Evidence-Based Communication Assessment and Intervention, 8:2, 62-101, DOI: 10.1080/17489539.2014.976332 To link to this article: http://dx.doi.org/10.1080/17489539.2014.976332 Published online: 02 Feb 2015. Submit your article to this journal Article views: 5252 View related articles View Crossmark data Citing articles: 1 View citing articles Full Terms & Conditions of access and use can be found at http://www.tandfonline.com/action/journalInformation?journalCode=tebc20 Download by: [University of Lethbridge] Date: 05 October 2015, At: 05:52 Evidence-Based Communication Assessment and Intervention, 2014 Vol. 8, No. 2, 62–101, http://dx.doi.org/10.1080/17489539.2014.976332 EBP Advancement Corner The persistence of fad interventions in the face of negative scientific evidence: Facilitated communication for autism as a case example Scott O. Lilienfeld1, Julia Marshall1, James T. Todd2 & Howard C. Shane3 1Department of Psychology, Emory University, Atlanta, GA, USA, 2Department of Psychology, Eastern Michigan University, Ypsilanti, MI, USA, 3Boston Children’s Hospital, Boston, MA, USA ................................................................................................................................................. Abstract Communication disorder and mental health professionals may assume that once novel clinical techniques have been refuted by research, they will be promptly abandoned. -

Healing the Symptoms Known As Autism Is Not Intended As Medical Advice
Disclaimer Healing the Symptoms Known as Autism is not intended as medical advice. This book is for informational and educational purposes only. Please consult a medical professional when the need for one is indicated. For obvious reasons neither the author, co-authors, contributing authors, the publisher, nor their associates can take medical or legal responsibility for having the contents herein considered as a prescription for everyone or anyone. You are ultimately responsible for the uses made of this book. All content, including text, graphics, images, and information, contained in this book or our website, is for general information purposes only. We take no responsibility for the accuracy of information contained herein, and such information is subject to change without notice. PDF E-Book Healing the symptoms known as AutisSecondm Edition by Kerri Rivera with Kimberly McDaniel & Daniel Bender Healing the Symptoms Known as Autism Second Edition (PDF E-Book Version) by Kerri Rivera with Kimberly McDaniel & Daniel Bender Copyright © 2014 by Kerri Rivera All rights reserved. No part of this book may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopying, recording, or by any information storage retrieval system without the written permission of the author. The only exception being by a reviewer who wishes to quote brief passages in connection with a review written for inclusion in a magazine, newspaper, blog, or broadcast. ISBN: 978-0-9892890-2-3 Library of Congress Control Number: 2013945511 (LOC# of Print Edition) 1st Edition released May 2013 2nd Edition released January 2014 Printed in the United States of America Mailing Address: AutismO2 PO Box 10334 Chicago, IL 60611 Feedback Email: [email protected] For further information: www.cdautism.org www.HealingTheSymptomsKnownAsAutism.com The Kalcker Parasite Protocol as integrated into Chapter 8 has portions Copyright ©2013 by Dr. -
Assisting Teachers and Families in Decision-Making Regarding Questionable and Pseudoscientific Interventions
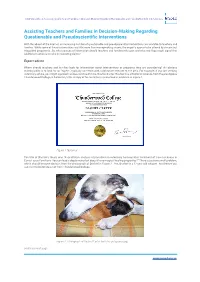
InSpEd Insights || Assisting Teachers and Families in Decision-Making Regarding Questionable and PseudoScientific Interventions Assisting Teachers and Families in Decision-Making Regarding Questionable and Pseudoscientific Interventions With the advent of the internet, an increasing number of questionable and pseudoscientific interventions are available to teachers and families. While some of these interventions are little more than moneymaking scams, the majority appear to be offered by sincere but misguided proponents. So, what sources of information should teachers and families rely upon and what red flags might signal that additional caution is needed in evaluating claims? Expert advice Where should teachers and families look for information about interventions or programs they are considering? An obvious starting point is to look for an “expert”, typically someone with a doctorate relevant to the area. For example, if you are seeking veterinary advice, you might approach a close relative of mine, Dashiel Carter. Dashiel has a Doctor of Science from the prestigious Thunderwood College in California, USA. A copy of his testamur is presented in evidence in Figure 1. Figure 1 Testamur The title of Dashiel’s thesis was “A qualitative analysis of pareidolia in veterinary homeopathic treatment of travel sickness in Canis Lupus Familiaris: You can lead a dog to water but does it have magical healing properties?” There is just one small problem, which should become obvious from the photograph of Dashiel in Figure 2 . Yes, Dashiel is a 12-year-old -
Table of Contents
(LAST UPDATED: 6/4/19_v18) A publication of the Autism Society of Southeastern Wisconsin Southeastern SocietyA publication Autism of of the RESOURCE DIRECTORY 3720 N. 124th Street Suite O, Wauwatosa, WI 53222 Phone: (414) 988-1260 Email: [email protected] Website: www.assew.org 1 BECOME A MEMBER TODAY! Our mission is to improve the lives of all that are affected by autism. We do this by providing quality programs, services and support to our nine county surrounding areas (Dodge, Jefferson, Kenosha, Milwaukee, Ozaukee, Racine, Washington, Walworth and Waukesha Counties in WI) Please fill out the enclosed Membership Application at the back of the directory or renew online at ASSEW.org Great Member Benefits Include: Information Services & Resources Phone & In-Person Support Lending Library Education & Development New to Autism for parents whose children have been diagnosed recently with an ASD. Spectrum of Support (SOS) Series Summer Bike Program TRAILS (Transition for Raising Autism Independence and Living Skills) Social Opportunities Exclusive Member Only Events are very popular! Network and socialize with families while having fun at places like: -Cool Waters Family Aquatic Park -Kids in Motion -Pump It Up -Milwaukee Brewers baseball games -Lasertag Adventure -Fun Zone and Fun Timez Social Groups for Middle Schoolers and Teens Support Support Groups are led by our qualified accredited staff and partners during the day and evenings. Morning Coffee & Evening Support Group Adults on the Spectrum Group Dad Support Group 3720 N 124th Street, Suite O Wauwatosa, WI 53222 (414)988-1260 [email protected] www.assew.org 2 Autism Society of Southeastern Wisconsin www.assew.org 414-988-1260 Autism Spectrum Disorders Resource Directory Purpose: This resource guide was designed to assist and empower parents in their journey of researching optimal services for their children with Autism Spectrum Disorders by providing information on local resources. -
IASLT Position Statement on the Rapid Prompting Method
IASLT Position Statement on the Rapid Prompting Method. May 2017 IRISH ASSOCIATION OF SPEECH & LANGUAGE THERAPISTS May 2017 Statement The Irish Association of Speech and Language Therapists (IASLT) is the recognised professional body for speech and language therapists (SLTs) in Ireland. One of the key functions of the IASLT is to represent the views of its members to inform public policy in relation to the provision of speech and language therapy services for the best interests of service users. Since the broadcast of the RTE documentary ‘Autism and Me’ on March 13th 2017 there has been much discussion about the Rapid Prompting Method (RPM) which was used to facilitate communication for one teenage boy featured on the programme. IASLT wish to put on record our position in relation to this method - primarily our concern that there is no evidence to support its use. Over the years, Autism Spectrum Disorders (ASD) has been the target for many anecdotal commercial ‘cures’ and interventions. These continue to be readily available despite having no scientific or empirical evidence in efficacy. Assessment and treatment protocols for communication disorders should be based in the most part on empirical evidence from well-constructed and independent research. RPM has yet to produce any of this to support its claims. IASLT’s concern is that as a method it is closely related to the technique known as: "Facilitated Communication" (FC) which has been proven to be ineffective and not evidence based. Peer reviewed publications about FC report that the children’s outputs were results of the facilitators’ movements and opinions – not those of the children’s themselves. -

SAVING LITERACY SAVING Dr
SAVING LITERACY Dr. Susan Rich Sheridan is a scholar/teacher with degrees in English, Art and Education. Her Neuroconstructive, brain-based theory and marks- based practice of literacy have a twenty-year history, including teaching first grade through college. Saving Literacy introduces the Scribbling/Drawing/ Writing program for children 10 months to 6 years, including developmental SAVING LITERACY benchmarks, lesson plans, evaluation tools, and research questions designed for professional caregivers: preschool and daycare providers, elementary school teachers, child psychologists, art teachers and art therapists, speech How Marks Change pathologists and researchers in child development and education. The goals of the program are sustained attention, emotional control and connection, expanded speech and literacy. Autism and the effects of technology are Minds discussed. Dr. Sheridan has published a companion book for parents, HandMade Marks. Attention “What we most need now… is a fresh perspective on the masses of data that neurobiologists have gathered, and on the puzzles those data pose… How do brains make sense of the world (?)… (A) new general theory… requires new assumptions and new definitions. I believe that the idea of meaning, a critical concept that defines the relations of each brain to the world, is central to current debates in philosophy and cognitive science, and will Connection become so in neurobiology… Doodling can and should accompany if not even precede speaking. Language derives from the dynamics and structure of intentional behavior... and the face and hand areas of the cortex lie side by side, undergoing the same patterns of neural development. They are inextricably linked, as we know from the necessity of Literacy moving our hands and fingers as we speak to communicate meaning most effectively.” Correspondence between Dr. -

Health Promoting Behaviors of Young Adults with Chronic Lyme Disease Patricia D
Walden University ScholarWorks Walden Dissertations and Doctoral Studies Walden Dissertations and Doctoral Studies Collection 2018 Health Promoting Behaviors of Young Adults with Chronic Lyme Disease Patricia D. Bolivar Walden University Follow this and additional works at: https://scholarworks.waldenu.edu/dissertations Part of the Epidemiology Commons This Dissertation is brought to you for free and open access by the Walden Dissertations and Doctoral Studies Collection at ScholarWorks. It has been accepted for inclusion in Walden Dissertations and Doctoral Studies by an authorized administrator of ScholarWorks. For more information, please contact [email protected]. Walden University College of Health Sciences This is to certify that the doctoral dissertation by Patricia Bolivar has been found to be complete and satisfactory in all respects, and that any and all revisions required by the review committee have been made. Review Committee Dr. Harold Griffin, Committee Chairperson, Public Health Faculty Dr. Lee Bewley, Committee Member, Public Health Faculty Dr. Vincent Agboto, University Reviewer, Public Health Faculty Chief Academic Officer Eric Riedel, Ph.D. Walden University 2018 Abstract Health Promoting Behaviors of Young Adults with Chronic Lyme Disease by Patricia D. Bolivar MS, California State University Los Angeles, 2001 BS, California State University Los Angeles, 1984 Dissertation Submitted in Partial Fulfillment of the Requirements for the Degree of Doctor of Philosophy Public Health Walden University February 2018 Abstract Lyme disease is the most prevalent arthropod-borne (tick) disease in North America. The disease is more prevalent in some Eastern and Central states than in Western states. The general problem is that, in southern California especially in Los Angeles County, both patients and practitioners fail to recognize the disease, resulting in misdiagnosis and delayed treatment. -

Understanding Autism Through Rapid Prompting Method Free Download
UNDERSTANDING AUTISM THROUGH RAPID PROMPTING METHOD FREE DOWNLOAD Soma Mukhopadhyay | 296 pages | 30 Oct 2008 | Outskirts Press | 9781432729288 | English | Parker CO, United States Rapid prompting method Mind Tree PoemsMarch. This is a preview of subscription content, log in to check access. American Speech-Language-Hearing Association. Overview Soma Mukhopadhyay, like so many mothers, would not accept the conventional wisdom when her son Tito was diagnosed with severe autism. Valle, C. Learn how to enable JavaScript on your browser. Retrieved 4 January Thanks for your feedback! Google Scholar. General Understanding Autism Through Rapid Prompting Method Alternative medicine Alternative veterinary medicine Quackery Health fraud History of alternative medicine Rise Understanding Autism Through Rapid Prompting Method modern medicine Pseudoscience Antiscience Skepticism Skeptical movement National Center for Complementary and Integrative Health Terminology of alternative medicine. Exceptionality, 18 131— Retrieved 9 April Biklen, D. Spitz, H. Strange son: Two mothers, two sons, and the quest to unlock the hidden world of autism. Tito, now an adult, is still profoundly autistic but Understanding Autism Through Rapid Prompting Method also developed talents as a poet, writer, and teacher. New York Times. Elliot, James. Autistic sociality. Sensory integration and the child. Strange Son. Blakeslee, S. Alternative medical systems Mind —body intervention Biologically-based therapy Manipulative methods Energy therapy. Curriculum guide for autism using rapid prompting method: With lesson plan suggestions. Facilitated communication and its legitimacy: 21st century developments. Skeptical Inquirer. Outskirts Press, Inc. Sign up for our Health Tip of the Day newsletter, and receive daily tips that will help you live your healthiest life. RPM presumes competence to increase students' interest, confidence and self-esteem. -

Representing Neurological Difference in Contemporary Autism Novels
MAKAI PÉTER KRISTÓF BRIDGING THE EMPATHY GAP: REPRESENTING NEUROLOGICAL DIFFERENCE IN CONTEMPORARY AUTISM NOVELS Supervisors: Kérchy Anna and Cristian Réka Mónika 2015 University of Szeged Faculty of Arts Doctoral School for Literary Studies Anglophone Literatures and Cultures in Europe and North America programme (2011-2014) - 1 - Dedicated to the loving memory of Gálik Julianna Katalin (1990-2013), and her RuneScape character, Tavarisu B, the best Dungeoneering partner one could ask for. We shall respawn. - 2 - TABLE OF CONTENTS Acknowledgements ......................................................................................................................... 2 Personal Preface: How I Got Here .................................................................................................. 7 Chapter 1 – Introduction: Literature, Science and The Humanities Meet Autism ....................... 11 Chapter 2 – The Use of Consilient Literary Interpretation in Reading the Autism Novel ........... 27 Chapter 3 – Autism’s Career in Psychology: Lighting Candles in A Dark Maze ........................ 37 Chapter 4 – Autism as Disability: Critical Studies of the Condition ............................................ 53 Chapter 5 – The Travelling Concept of ‘Theory of Mind’ in Philosophy, Psychology, Literary Studies and its Relation to Autism ................................................................................................ 75 Chapter 6 – Contextualising the Autism Novel in Contemporary Culture: Constructing Fascinating Narratives -

Rapid Prompting Method (RPM): a Suitable Intervention for Students with ASD?
REACH Journal of Special Needs Education in Ireland, Vol. 29.2 (2016), 92–100. Rapid Prompting Method (RPM): A suitable intervention for students with ASD? Rapid Prompting Method (RPM) has been suggested as an intervention suitable for use with individuals with Autistic Spectrum Disorders (ASD). The authors present a review of current research in the area. Three studies qualified for inclusion and findings were summarised into four categories. Findings appear to indicate an association between RPM and a decrease in repetitive behaviours. Further research in the area of RPM is warranted in order for it to be considered as a qualifying evidence-based practice. EVELYN DEACY, FIONA JENNINGS and AILBHE O’ HALLORAN are lecturers in the Centre for SEN, Inclusion and Diversity (CSENID) in St. Angela’s College, Sligo. INTRODUCTION Social media, conference presentations and commercial activity indicate the growth in popularity of Rapid Prompting Method (RPM) in Ireland. A growing demand for and widespread dissemination of RPM has led to its adoption in schools and by parents. As a result, the Minister for Education and Skills has been requested to support the use of RPM in schools (Parliamentary Debates, 2014). Consequently, a review of the literature and evidence base for this intervention is warranted due to the increased promotion for evidence-based practice in the education of students with Autistic Spectrum Disorders (ASD) (Simpson, 2005). Rapid Prompting Method was created by Soma Mukhopadhyay, a parent of a son (Tito) with autism. Through RPM, Tito Mukhopadhyay has written books, short stories and poetry on his experiences. In 2000, RPM was highlighted in the media by the BBC in Tito’s Story and subsequently in ‘Sixty Minutes’ (2003), and on CNN in 2008 in the US. -

How One Communication Tool May Fail Some Autistic People
Spectrum | Autism Research News https://www.spectrumnews.org DEEP DIVE How one communication tool may fail some autistic people BY BRENDAN BORRELL 1 JULY 2020 Illustration by Francesco Zorzi Aulton Grubbs sits in a chair against the wall of a small white room. A skinny teenager in athletic attire, he covers his eyes and ears with his hands while making a creaking noise with his vocal cords. The only word Aulton ever says, albeit sporadically, is “done.” Like roughly a quarter of people with autism, he struggles to communicate, which is why his mother has brought him to this two-story brick building in a leafy neighborhood in Austin, Texas. It is late February and this is Aulton’s third day working with educator Soma Mukhopadhyay, who glides into the room wearing an oversized tan work shirt atop an elegant red sari. Her diminutive frame and hushed, lilting voice belie her intensity. She makes a beeline toward Aulton, ignoring the adults in the room. “Today, you decide what should we do,” she says to Aulton as she holds up a plastic board with the alphabet on it in front of him. “‘S’ for ‘science’ or ‘P’ for ‘poetry.’” She peels Aulton’s right hand from his face. He gingerly extends his pointer finger toward the board, gazing in a different direction. His finger lands on the ‘Q’ first and then the ‘P.’ “P, that’s right,” Mukhopadhyay says. She shifts the letter board to the right to bring the ‘O’ closer to his finger. “You’re right, you’re right,” she says.