Subgingival Microbiome of Gingivitis in Chinese Undergraduates Ke DENG1, Xiang Ying OUYANG1, Yi CHU2, Qian ZHANG3
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

An Integrative Bayesian Dirichlet-Multinomial Regression Model for the Analysis of Taxonomic Abundances in Microbiome Data
Wadsworth et al. BMC Bioinformatics (2017) 18:94 DOI 10.1186/s12859-017-1516-0 METHODOLOGY ARTICLE Open Access An integrative Bayesian Dirichlet- multinomial regression model for the analysis of taxonomic abundances in microbiome data W. Duncan Wadsworth1, Raffaele Argiento2, Michele Guindani3, Jessica Galloway-Pena4, Samuel A. Shelburne5 and Marina Vannucci1* Abstract Background: The Human Microbiome has been variously associated with the immune-regulatory mechanisms involved in the prevention or development of many non-infectious human diseases such as autoimmunity, allergy and cancer. Integrative approaches which aim at associating the composition of the human microbiome with other available information, such as clinical covariates and environmental predictors, are paramount to develop a more complete understanding of the role of microbiome in disease development. Results: In this manuscript, we propose a Bayesian Dirichlet-Multinomial regression model which uses spike-and-slab priors for the selection of significant associations between a set of available covariates and taxa from a microbiome abundance table. The approach allows straightforward incorporation of the covariates through a log-linear regression parametrization of the parameters of the Dirichlet-Multinomial likelihood. Inference is conducted through a Markov Chain Monte Carlo algorithm, and selection of the significant covariates is based upon the assessment of posterior probabilities of inclusions and the thresholding of the Bayesian false discovery rate. We design a simulation study to evaluate the performance of the proposed method, and then apply our model on a publicly available dataset obtained from the Human Microbiome Project which associates taxa abundances with KEGG orthology pathways. The method is implemented in specifically developed R code, which has been made publicly available. -

Probiotic Alternative to Chlorhexidine in Periodontal Therapy: Evaluation of Clinical and Microbiological Parameters
microorganisms Article Probiotic Alternative to Chlorhexidine in Periodontal Therapy: Evaluation of Clinical and Microbiological Parameters Andrea Butera , Simone Gallo * , Carolina Maiorani, Domenico Molino, Alessandro Chiesa, Camilla Preda, Francesca Esposito and Andrea Scribante * Section of Dentistry–Department of Clinical, Surgical, Diagnostic and Paediatric Sciences, University of Pavia, 27100 Pavia, Italy; [email protected] (A.B.); [email protected] (C.M.); [email protected] (D.M.); [email protected] (A.C.); [email protected] (C.P.); [email protected] (F.E.) * Correspondence: [email protected] (S.G.); [email protected] (A.S.) Abstract: Periodontitis consists of a progressive destruction of tooth-supporting tissues. Considering that probiotics are being proposed as a support to the gold standard treatment Scaling-and-Root- Planing (SRP), this study aims to assess two new formulations (toothpaste and chewing-gum). 60 patients were randomly assigned to three domiciliary hygiene treatments: Group 1 (SRP + chlorhexidine-based toothpaste) (control), Group 2 (SRP + probiotics-based toothpaste) and Group 3 (SRP + probiotics-based toothpaste + probiotics-based chewing-gum). At baseline (T0) and after 3 and 6 months (T1–T2), periodontal clinical parameters were recorded, along with microbiological ones by means of a commercial kit. As to the former, no significant differences were shown at T1 or T2, neither in controls for any index, nor in the experimental -
Xiexin Tang Improves the Symptom of Type 2 Diabetic Rats by Modulation of the Gut Microbiota
www.nature.com/scientificreports OPEN Xiexin Tang improves the symptom of type 2 diabetic rats by modulation of the gut microbiota Received: 30 August 2017 Xiaoyan Wei, Jinhua Tao , Suwei Xiao, Shu Jiang, Erxin Shang, Zhenhua Zhu, Dawei Qian Accepted: 13 February 2018 & Jinao Duan Published: xx xx xxxx Type 2 diabetes mellitus (T2DM), a chronic metabolic disease which severely impairs peoples’ quality of life, currently attracted worldwide concerns. There are growing evidences that gut microbiota can exert a great impact on the development of T2DM. Xiexin Tang (XXT), a traditional Chinese medicine prescription, has been clinically used to treat diabetes for thousands of years. However, few researches are investigated on the modulation of gut microbiota community by XXT which will be very helpful to unravel how it works. In this study, bacterial communities were analyzed based on high-throughput 16S rRNA gene sequencing. Results indicated that XXT could notably shape the gut microbiota. T2DM rats treated with XXT exhibited obvious changes in the composition of the gut microbiota, especially for some short chain fatty acids producing and anti-infammatory bacteria such as Adlercreutzia, Alloprevotella, Barnesiella, [Eubacterium] Ventriosum group, Blautia, Lachnospiraceae UCG-001, Papillibacter and Prevotellaceae NK3B31 group. Additionally, XXT could also signifcantly ameliorate hyperglycemia, lipid metabolism dysfunction and infammation in T2DM rats. Moreover, the correlation analysis illustrated that the key microbiota had a close relationship with the T2DM related indexes. The results probably provided useful information for further investigation on its active mechanism and clinical application. T2DM, a chronic metabolic disease characterized by hyperglycemia as a result of insufcient insulin secretion, insulin action or both1, is estimated that its numbers in the adults will increase by 55% by 20352. -

Microbiological, Lipid and Immunological Profiles in Children
Original Article http://dx.doi.org/10.1590/1678-77572016-0196 Microbiological, lipid and immunological SUR¿OHVLQFKLOGUHQZLWKJLQJLYLWLVDQG type 1 diabetes mellitus Abstract Cristiane DUQUE1 Objective: The aim of this study was to compare the prevalence of SHULRGRQWDOSDWKRJHQVV\VWHPLFLQÀDPPDWRU\PHGLDWRUVDQGOLSLGSUR¿OHVLQ Mariana Ferreira Dib JOÃO2 type 1 diabetes children (DM) with those observed in children without diabetes Gabriela Alessandra da Cruz (NDM), both with gingivitis. Material and methods: Twenty-four DM children Galhardo CAMARGO3 and twenty-seven NDM controls were evaluated. The periodontal status, 3 Gláucia Schuindt TEIXEIRA JO\FHPLF DQG OLSLG SUR¿OHV ZHUH GHWHUPLQHG IRU ERWK JURXSV 6XEJLQJLYDO Thamiris Santana MACHADO3 samples of periodontal sites were collected to determine the prevalence of Rebeca de Souza AZEVEDO3 SHULRGRQWDOPLFURRUJDQLVPVE\3&5%ORRGVDPSOHVZHUHFROOHFWHGIRU,/ǃ Flávia Sammartino MARIANO2 TNF-D and IL-6 analysis using ELISA kits. Results: Periodontal conditions of DM Natália Helena COLOMBO1 and NDM patients were similar, without statistical differences in periodontal indices. When considering patients with gingivitis, all lipid parameters Natália Leal VIZOTO2 evaluated were highest in the DM group; Capnocytophaga sputigena and Renata de Oliveira Capnocytophaga ochracea were more prevalent in the periodontal sites of DM 2 MATTOS-GRANER children. “Red complex” bacteria were detected in few sites of DM and NDM groups. Fusobacterium nucleatum and Campylobacter rectus were frequently IRXQGLQERWKJURXSV6LPLODUOHYHOVRI,/ǃ71)D -

Gut Microbiome Composition Remains Stable in Individuals with Diabetes-Related Early to Late Stage Chronic Kidney Disease
biomedicines Article Gut Microbiome Composition Remains Stable in Individuals with Diabetes-Related Early to Late Stage Chronic Kidney Disease Ashani Lecamwasam 1,2,3,*, Tiffanie M. Nelson 4, Leni Rivera 3, Elif I. Ekinci 2,5, Richard Saffery 1,6 and Karen M. Dwyer 3 1 Epigenetics Research, Murdoch Children’s Research Institute, VIC 3052, Australia; [email protected] 2 Department of Endocrinology, Austin Health, VIC 3079, Australia; [email protected] 3 School of Medicine, Faculty of Health, Deakin University, VIC 3220, Australia; [email protected] (L.R.); [email protected] (K.M.D.) 4 Menzies Health Institute Queensland, Griffith University, QLD 4222, Australia; [email protected] 5 Department of Medicine, University of Melbourne, VIC 3010, Australia 6 Department of Paediatrics, University of Melbourne, VIC 3010, Australia * Correspondence: [email protected]; Tel.: +613-8341-6200; Fax: +613-9348-1391 Abstract: (1) Background: Individuals with diabetes and chronic kidney disease display gut dysbiosis when compared to healthy controls. However, it is unknown whether there is a change in dysbiosis across the stages of diabetic chronic kidney disease. We investigated a cross-sectional study of patients with early and late diabetes associated chronic kidney disease to identify possible microbial differences between these two groups and across each of the stages of diabetic chronic kidney disease. (2) Methods: This cross-sectional study recruited 95 adults. DNA extracted from collected stool samples were used for 16S rRNA sequencing to identify the bacterial community in the Citation: Lecamwasam, A.; Nelson, gut. (3) Results: The phylum Firmicutes was the most abundant and its mean relative abundance T.M.; Rivera, L.; Ekinci, E.I.; Saffery, was similar in the early and late chronic kidney disease group, 45.99 ± 0.58% and 49.39 ± 0.55%, R.; Dwyer, K.M. -
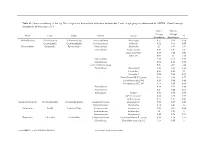
Genus Contributing to the Top 70% of Significant Dissimilarity of Bacteria Between Day 7 and 18 Age Groups As Determined by SIMPER
Table S1: Genus contributing to the top 70% of significant dissimilarity of bacteria between day 7 and 18 age groups as determined by SIMPER. Overall average dissimilarity between ages is 51%. Day 7 Day 18 Average Average Phyla Class Order Family Genus % Abundance Abundance Actinobacteria Actinobacteria Actinomycetales Actinomycetaceae Actinomyces 0.57 0.24 0.74 Coriobacteriia Coriobacteriales Coriobacteriaceae Collinsella 0.51 0.61 0.57 Bacteroidetes Bacteroidia Bacteroidales Bacteroidaceae Bacteroides 2.1 1.63 1.03 Marinifilaceae Butyricimonas 0.82 0.81 0.9 Sanguibacteroides 0.08 0.42 0.59 CAG-873 0.01 1.1 1.68 Marinifilaceae 0.38 0.78 0.91 Marinifilaceae 0.78 1.04 0.97 p-2534-18B5 gut group 0.06 0.7 1.04 Prevotellaceae Alloprevotella 0.46 0.83 0.89 Prevotella 2 0.95 1.11 1.3 Prevotella 7 0.22 0.42 0.56 Prevotellaceae NK3B31 group 0.62 0.68 0.77 Prevotellaceae UCG-003 0.26 0.64 0.89 Prevotellaceae UCG-004 0.11 0.48 0.68 Prevotellaceae 0.64 0.52 0.89 Prevotellaceae 0.27 0.42 0.55 Rikenellaceae Alistipes 0.39 0.62 0.77 dgA-11 gut group 0.04 0.38 0.56 RC9 gut group 0.79 1.17 0.95 Epsilonbacteraeota Campylobacteria Campylobacterales Campylobacteraceae Campylobacter 0.58 0.83 0.97 Helicobacteraceae Helicobacter 0.12 0.41 0.6 Firmicutes Bacilli Lactobacillales Enterococcaceae Enterococcus 0.36 0.31 0.64 Lactobacillaceae Lactobacillus 1.4 1.24 1 Streptococcaceae Streptococcus 0.82 0.58 0.53 Firmicutes Clostridia Clostridiales Christensenellaceae Christensenellaceae R-7 group 0.38 1.36 1.56 Clostridiaceae Clostridium sensu stricto 1 1.16 0.58 -

Activity of Chlorhexidine Formulations on Oral Microorganisms and Periodontal Ligament Fibroblasts
Activity of chlorhexidine formulations on oral microorganisms and periodontal ligament fibroblasts Accepted for publication December 17, 2020 Alexandra Stähli1, Irina Liakhova1, Barbara Cvikl2, Adrian Lussi3, Anton Sculean1, Sigrun Eick1* 1Department of Periodontology, School of Dental Medicine, University of Bern, Switzerland 2Department of Conservative Dentistry, Sigmund Freud University, Vienna, Austria 3Department of Operative Dentistry and Periodontology, Faculty of Dentistry, University Medical Centre, Freiburg, Germany and School of Dental Medicine, University of Bern, Switzerland Keywords: biofilm; antiseptics; cytotoxicity Correspondence: Sigrun Eick, Klinik für Parodontologie, Labor Orale Mikrobiologie, Freiburgstrasse 7, CH-3010 Bern e-mail: [email protected]; phone +41 31 623 2542 1 Abstract Given the importance of microorganisms in the pathogenesis of the two most prevalent oral diseases (i.e. caries and periodontitis), antiseptics are widely used. Among the antiseptics chlorhexidine (CHX) is still considered as gold standard. The purpose of this in-vitro-study was to determine the antimicrobial activity of new CHX digluconate containing formulations produced in Switzerland. Two test formulations, with 0.1% or 0.2% CHX (TestCHX0.1, TestCHX0.2) were compared with 0.1% and 0.2% CHX digluconate solutions (CHXph0.1, CHXph0.2) without additives and with a commercially available formulation containing 0.2% CHX digluconate (CHXcom0.2). The minimal inhibitory concentrations (MIC) of the CHX formulations were determined against bacteria associated with caries or periodontal disease. Then the anti-biofilm activities of CHX preparations were tested regarding inhibition of biofilm formation or against an existing biofilm. Further, the cytotoxicity of the CHX preparations against periodontal ligament (PDL) fibroblasts was measured. There were no or only minor differences of the MIC values between the CHX preparations. -

Role of Actinobacteria and Coriobacteriia in the Antidepressant Effects of Ketamine in an Inflammation Model of Depression
Pharmacology, Biochemistry and Behavior 176 (2019) 93–100 Contents lists available at ScienceDirect Pharmacology, Biochemistry and Behavior journal homepage: www.elsevier.com/locate/pharmbiochembeh Role of Actinobacteria and Coriobacteriia in the antidepressant effects of ketamine in an inflammation model of depression T Niannian Huanga,1, Dongyu Huaa,1, Gaofeng Zhana, Shan Lia, Bin Zhub, Riyue Jiangb, Ling Yangb, ⁎ ⁎ Jiangjiang Bia, Hui Xua, Kenji Hashimotoc, Ailin Luoa, , Chun Yanga, a Department of Anesthesiology, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan 430030, China b Department of Internal Medicine, The Third Affiliated Hospital of Soochow University, Changzhou 213003, China c Division of Clinical Neuroscience, Chiba University Center for Forensic Mental Health, Chiba 260-8670, Japan ARTICLE INFO ABSTRACT Keywords: Ketamine, an N-methyl-D-aspartic acid receptor (NMDAR) antagonist, elicits rapid-acting and sustained anti- Ketamine depressant effects in treatment-resistant depressed patients. Accumulating evidence suggests that gut microbiota Depression via the gut-brain axis play a role in the pathogenesis of depression, thereby contributing to the antidepressant Lipopolysaccharide actions of certain compounds. Here we investigated the role of gut microbiota in the antidepressant effects of Gut microbiota ketamine in lipopolysaccharide (LPS)-induced inflammation model of depression. Ketamine (10 mg/kg) sig- nificantly attenuated the increased immobility time in forced swimming test (FST), which was associated with the improvements in α-diversity, consisting of Shannon, Simpson and Chao 1 indices. In addition to α-diversity, β-diversity, such as principal coordinates analysis (PCoA), and linear discriminant analysis (LDA) coupled with effect size measurements (LEfSe), showed a differential profile after ketamine treatment. -

Periodontal Health, Gingival Diseases and Conditions 99 Section 1 Periodontal Health
CHAPTER Periodontal Health, Gingival Diseases 6 and Conditions Section 1 Periodontal Health 99 Section 2 Dental Plaque-Induced Gingival Conditions 101 Classification of Plaque-Induced Gingivitis and Modifying Factors Plaque-Induced Gingivitis Modifying Factors of Plaque-Induced Gingivitis Drug-Influenced Gingival Enlargements Section 3 Non–Plaque-Induced Gingival Diseases 111 Description of Selected Disease Disorders Description of Selected Inflammatory and Immune Conditions and Lesions Section 4 Focus on Patients 117 Clinical Patient Care Ethical Dilemma Clinical Application. Examination of the gingiva is part of every patient visit. In this context, a thorough clinical and radiographic assessment of the patient’s gingival tissues provides the dental practitioner with invaluable diagnostic information that is critical to determining the health status of the gingiva. The dental hygienist is often the first member of the dental team to be able to detect the early signs of periodontal disease. In 2017, the American Academy of Periodontology (AAP) and the European Federation of Periodontology (EFP) developed a new worldwide classification scheme for periodontal and peri-implant diseases and conditions. Included in the new classification scheme is the category called “periodontal health, gingival diseases/conditions.” Therefore, this chapter will first review the parameters that define periodontal health. Appreciating what constitutes as periodontal health serves as the basis for the dental provider to have a stronger understanding of the different categories of gingival diseases and conditions that are commonly encountered in clinical practice. Learning Objectives • Define periodontal health and be able to describe the clinical features that are consistent with signs of periodontal health. • List the two major subdivisions of gingival disease as established by the American Academy of Periodontology and the European Federation of Periodontology. -

A Histologic Bioassay of the Effect of Endotoxin of Escherichia Coli 0111:B4 Strain Injected Into Guinea Pig Oral Mucosa
Loyola University Chicago Loyola eCommons Master's Theses Theses and Dissertations 1983 A Histologic Bioassay of the Effect of Endotoxin of Escherichia coli 0111:B4 Strain Injected Into Guinea Pig Oral Mucosa Juan Jose de Obarrio Loyola University Chicago Follow this and additional works at: https://ecommons.luc.edu/luc_theses Part of the Periodontics and Periodontology Commons Recommended Citation de Obarrio, Juan Jose, "A Histologic Bioassay of the Effect of Endotoxin of Escherichia coli 0111:B4 Strain Injected Into Guinea Pig Oral Mucosa" (1983). Master's Theses. 3280. https://ecommons.luc.edu/luc_theses/3280 This Thesis is brought to you for free and open access by the Theses and Dissertations at Loyola eCommons. It has been accepted for inclusion in Master's Theses by an authorized administrator of Loyola eCommons. For more information, please contact [email protected]. This work is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 3.0 License. Copyright © 1983 Juan Jose de Obarrio A HISTOLOGIC BIOASSAY OF THE EFFECT OF ENDOTOXIN OF ESCHERICHIA COLI 0111:84 STRAIN INJECTED INTO GUINEA PIG ORAL MUCOSA BY Juan Jose de Obarrio A Thesis Submitted to the Faculty of the Graduate School of Loyola University of Chicago in Partial Fulfillment of the Requirements for the Degree of Master of Science May 1982 DEDICATION To my loving parents, Juan Luis and Helga, for their caring, understanding and who made possible my postgraduate education. To my fiance, Rocio, for her love and support. ii ACKNOWLEDGEMENTS I wish to express my sincere gratitude and appreciation to my Director, Dr. Patrick D. -

Suppression of Murine Lymphocyte Mitogen Responses by Exopolysaccharide from Capnocytophaga Ochracea RONALD W
INFECTION AND IMMUNITY, Jan. 1983, p. 476-479 Vol. 39, No. 1 0019-9567/83/010476-04$02.00/0 Copyright C 1983, American Society for Microbiology Suppression of Murine Lymphocyte Mitogen Responses by Exopolysaccharide from Capnocytophaga ochracea RONALD W. BOLTON* AND JOHN K. DYER Department of Oral Biology, College of Dentistry, University of Nebraska Medical Center, Lincoln, Nebraska 68583-0740 Received 26 July 1982/Accepted 5 October 1982 An extracellular polysaccharide was purified from culture supernatants of Capnocytophaga ochracea 25, a gram-negative bacillus associated with human periodontal disease. The extracellular polysaccharide suppressed in vitro mito- genic responses of murine splenic lymphocytes to concanavalin A and lipopoly- saccharide. This suppression was dose dependent, persisted up to 120 h, and was not caused by direct toxicity of the extracellular polysaccharide. Modulation of immune responses by bacterial C. ochracea 25, a gift from S. S. Socransky, components has received considerable attention Forsythe Dental Center, Boston, was cultivated in recent years (1, 2, 4, 5). Since a number of at 37°C in Trypticase soy broth supplemented these substances are produced by members of with 1% yeast extract and 0.1% NaHCO3. After the normal bacterial flora, they may have con- 48 h the cultures were centrifuged at 10,000 x g siderable impact on host-parasite interactions. for 15 min at 4°C. EP was isolated from liquid Indeed, there are several diseases of microbial culture supernatants by cold 95% ethanol pre- etiology, both clinical and experimental, which cipitation. The precipitate was dissolved in wa- have been associated with immune suppression ter and treated with cold 10% trichloroacetic or enhancement (reviewed in reference 12). -

Prevotella Intermedia
The principles of identification of oral anaerobic pathogens Dr. Edit Urbán © by author Department of Clinical Microbiology, Faculty of Medicine ESCMID Online University of Lecture Szeged, Hungary Library Oral Microbiological Ecology Portrait of Antonie van Leeuwenhoek (1632–1723) by Jan Verkolje Leeuwenhook in 1683-realized, that the film accumulated on the surface of the teeth contained diverse structural elements: bacteria Several hundred of different© bacteria,by author fungi and protozoans can live in the oral cavity When these organisms adhere to some surface they form an organizedESCMID mass called Online dental plaque Lecture or biofilm Library © by author ESCMID Online Lecture Library Gram-negative anaerobes Non-motile rods: Motile rods: Bacteriodaceae Selenomonas Prevotella Wolinella/Campylobacter Porphyromonas Treponema Bacteroides Mitsuokella Cocci: Veillonella Fusobacterium Leptotrichia © byCapnophyles: author Haemophilus A. actinomycetemcomitans ESCMID Online C. hominis, Lecture Eikenella Library Capnocytophaga Gram-positive anaerobes Rods: Cocci: Actinomyces Stomatococcus Propionibacterium Gemella Lactobacillus Peptostreptococcus Bifidobacterium Eubacterium Clostridium © by author Facultative: Streptococcus Rothia dentocariosa Micrococcus ESCMIDCorynebacterium Online LectureStaphylococcus Library © by author ESCMID Online Lecture Library Microbiology of periodontal disease The periodontium consist of gingiva, periodontial ligament, root cementerum and alveolar bone Bacteria cause virtually all forms of inflammatory