Hip and Knee Total Joint Replacement
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Knee Flow Chart Acute
Symptom chart for acute knee pain START HERE Did the knee pain begin Does the knee joint You may have a fracture or Stop what you are doing immediately and go to a hospital emergency room YES YES suddenly, with an injury, appear deformed, or dislocated patella. or an orthopedic surgeon specializing in knee problems. slip, fall, or collision? out of position? If possible, splint the leg to limit the movement of the knee until you reach NO the doctor. Do not put any weight on the knee. Use a wheelchair, a cane, or NO crutch to prevent putting any weight on the leg, which might cause further damage to the joint. GO TO FLOW CHART #2 Go to an orthopedic surgeon Stop what you are doing. Continuing activity despite the feeling that the knee ON CHRONIC KNEE Did you hear a “pop” YES immediately, you may have is unstable can cause additional damage to other ligaments, meniscus , and PROBLEMS THAT DEVELOP and does your knee feel torn your anterior cruciate, or cartilage. Try ice on the knee to control swelling. Take anti-in ammatories OR WORSEN OVER TIME. unstable or wobbly? other ligaments in the knee. like Advil or Nuprin until your doctor’s appointment. About a third of ligament tears get better with exercises, a third may need a brace, and a third may need sur gery. NO Use R•I•C•E for sore knees Does your knee hurt YES You may have damaged the articular Try anti-in ammatories, as directed on the bottle, for two days to reduce R: Rest as you bend it? cartilage on the bottom of the the chronic in ammation. -

Total HIP Replacement Exercise Program 1. Ankle Pumps 2. Quad
3 sets of 10 reps (30 ea) 2 times a day Total HIP Replacement Exercise Program 5. Heel slides 1. Ankle Pumps Bend knee and pull heel toward buttocks. DO NOT GO Gently point toes up towards your nose and down PAST 90* HIP FLEXION towards the surface. Do both ankles at the same time or alternating feet. Perform slowly. 2. Quad Sets Slowly tighten thigh muscles of legs, pushing knees down into the surface. Hold for 10 count. 6. Short Arc Quads Place a large can or rolled towel (about 8”diameter) under the leg. Straighten knee and leg. Hold straight for 5 count. 3. Gluteal Sets Squeeze the buttocks together as tightly as possible. Hold for a 10 count. 7. Knee extension - Long Arc Quads Slowly straighten operated leg and try to hold it for 5 sec. Bend knee, taking foot under the chair. 4. Abduction and Adduction Slide leg out to the side. Keep kneecap pointing toward ceiling. Gently bring leg back to pillow. May do both legs at the same time. Copywriter VHI Corp 3 sets of 10 reps (30 ea) 2 times a day Total HIP Replacement Exercise Program 8. Standing Stair/Step Training: Heel/Toe Raises: 1. The “good” (non-operated) leg goes Holding on to an immovable surface. UP first. Rise up on toes slowly 2. The “bad” (operated) leg goes for a 5 count. Come back to foot flat and lift DOWN first. toes from floor. 3. The cane stays on the level of the operated leg. Resting positions: To Stretch your hip to neutral position: 1. -
Arthroscopic and Open Anatomy of the Hip 11
CHAPTER Arthroscopic and o'pen Anatomy of the Hip Michael B. Gerhardt, Kartik Logishetty, Morteza lV1eftah, and Anil S. Ranawat INTRODUCTION movements that they induce at the joint: 1) flexors; 2) extensors; 3) abductors; 4) adductors; 5) external rotators; and 6) interI12 I The hip joint is defined by the articulation between the head rotators. Although some muscles have dual roles, their primary of the femur and the aeetahulum of the pelvis. It is covered by functions define their group placem(:)nt, and they all have ullique :l large soft-tissue envelope and a complex array of neurovascu- neurovascular supplies (TIt ble 2-1). lar and musculotendinous structures. The joint's morphology The vascular supply of tbe hip stems from the external and anu orientation are complex, and there are wide anatomi c varia- internal iLiac ancries. An understanding of the course of these tions seen among individuals. The joint's deep location makes vessels is critical fo r ,lVo iding catasu"ophic vascular injury. fn both arthroscopic and open access challenging. To avoid iatro- addition, the blood supply to the fel11()ra l head is vulnerahle to genic injury while establishing functional and efficient access, both traumatic and iatrogenic injury; the disruption of this sup- the hip surgeon should possess a sound ana tomic knowledge of ply can result in avascular necrosis (Figure 2-2). the hip. T he human "hip" can be subdivided into three categories: I) the superficial surface anatomy; 2) the deep femoroacetabu- la r Joint and capsule; and 3) the associated structures, including the muscles, nerves, and vasculature, all of which directly affeet HIP MUSCULATURE its function. -

Hip Extensor Mechanics and the Evolution of Walking and Climbing Capabilities in Humans, Apes, and Fossil Hominins
Hip extensor mechanics and the evolution of walking and climbing capabilities in humans, apes, and fossil hominins Elaine E. Kozmaa,b,1, Nicole M. Webba,b,c, William E. H. Harcourt-Smitha,b,c,d, David A. Raichlene, Kristiaan D’Aoûtf,g, Mary H. Brownh, Emma M. Finestonea,b, Stephen R. Rossh, Peter Aertsg, and Herman Pontzera,b,i,j,1 aGraduate Center, City University of New York, New York, NY 10016; bNew York Consortium in Evolutionary Primatology, New York, NY 10024; cDepartment of Anthropology, Lehman College, New York, NY 10468; dDivision of Paleontology, American Museum of Natural History, New York, NY 10024; eSchool of Anthropology, University of Arizona, Tucson, AZ 85721; fInstitute of Ageing and Chronic Disease, University of Liverpool, Liverpool L7 8TX, United Kingdom; gDepartment of Biology, University of Antwerp, 2610 Antwerp, Belgium; hLester E. Fisher Center for the Study and Conservation of Apes, Lincoln Park Zoo, Chicago, IL 60614; iDepartment of Anthropology, Hunter College, New York, NY 10065; and jDepartment of Evolutionary Anthropology, Duke University, Durham, NC 27708 Edited by Carol V. Ward, University of Missouri-Columbia, Columbia, MO, and accepted by Editorial Board Member C. O. Lovejoy March 1, 2018 (received for review September 10, 2017) The evolutionary emergence of humans’ remarkably economical their effects on climbing performance or tested whether these walking gait remains a focus of research and debate, but experi- traits constrain walking and running performance. mentally validated approaches linking locomotor -
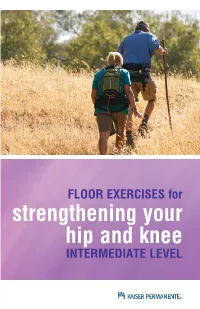
FLOOR EXERCISES for Strengthening Your Hip and Knee INTERMEDIATE LEVEL THIGH STRENGTHENING 3
FLOOR EXERCISES for strengthening your hip and knee INTERMEDIATE LEVEL THIGH STRENGTHENING 3 HIP STRENGTHENING ON YOUR SIDE 5 HIP STRENGTHENING ON YOUR BACK 8 ALL 4’S WITH LEG LIFT 10 hen you have pain or an injury to your knee or lower extremity, Wit’s necessary to strengthen muscles in your whole lower body to have the best recovery possible, even if your injury is just in one area. The hip and trunk muscles support your knee, ankle and foot, and they all work together when you move. The exercises in this booklet will help you strengthen these muscles to help you recover. Please read the instructions carefully and follow the advice of your physical therapist or doctor when starting or progressing an exer- cise program such as this. If your symptoms get worse while doing these exercises, please read the instructions again to be sure you are doing the exercises exactly as described. If your symptoms con- tinue to worsen, talk to your health care provider. Equipment needed: • exercise ball • pillow • foam • towel(s) • exercise band ________ (color) or resistance band 2 THIGH (QUADRICEPS) STRENGTHENING q Quadriceps set: Place a small towel roll under your knee. Straighten your knee by tightening your thigh muscles. Press the back of your knee into the floor or towel and hold for 5-10 seconds. This may also be done sitting. FREQUENCY_____________ q Straight leg raise: Lie on your back with your affected leg straight and your other leg bent. Tighten your thigh muscle then lift your straight leg no higher than the other knee without allow- ing your knee to bend. -

BJH24901 Hip Replacement
ORTHOPEDICS Hip Replacement Surgery PRIMARY TOTAL HIP REPLACEMENT HEALTHY HIP A primary total hip replacement is a first time hip replacement surgery. Socket lined with cartilage Muscle (acetabulum) Why have a hip replaced? The goals of a hip replacement are to get rid of hip pain and help Tendon you be more active. A hip that is stiff and painful can be replaced with an artificial joint. This is called hip prosthesis. Hip replacements also help with damaged hips caused by Ball covered arthritis, rheumatoid arthritis and other hip-related issues. with cartilage (head of the thighbone) Pelvic bone How the hip works Thighbone The hip is a ball-and-socket-joint. In this case, the ball component (femur) is attached to the top of the femur (long bone of the thigh). The acetabulum (socket) is part of the pelvis. The ball rotating in the socket helps you move your leg. With a healthy hip, smooth cartilage covering the ends of the thigh Image courtesy of Krames StayWell bone and pelvis allows the ball to glide easily inside the socket. DAMAGED HIP DAMAGED HIP With a damaged hip, the worn cartilage no longer serves as a cushion. The surfaces of these bones become rough. This Cartilage Joint damage Tendon inflammation causes pain when they rub together. The cartilage may wear away, leaving nothing to help the bones move smoothly. Arthritis can cause inflammation and swelling around the joint. This causes pain and stiffness in the hip. (continued) Images courtesy of Krames StayWell ORTHOPEDICS PRIMARY TOTAL HIP REPLACEMENT (continued) PROBLEMS FROM SURGERY Although hip replacement can help with pain, there’s also the chance that surgery will cause problems. -

Medial Collateral Ligament (MCL) Sprain
INFORMATION FOR PATIENTS Medial collateral ligament (MCL) sprain This leaflet intends to educate you on Knee ligament sprains are graded in the immediate management of your severity from one to three: knee injury. It also contains exercises to prevent stiffening of your knee, Grade one: Mild sprain with ligaments whilst your ligament heals. stretched but not torn. Grade two: Moderate sprain with some What is an MCL injury? ligaments torn. Grade three: Severe sprain with There are two collateral ligaments, one complete tear of ligaments. either side of the knee, which act to stop side to side movement of the knee. The Symptoms you may experience medial collateral ligament (MCL) is most commonly injured. It lies on the inner side Pain in the knee, especially on the of your knee joint, connecting your thigh inside, particularly with twisting bone (femur) to your shin bone (tibia) and movements. provides stability to the knee. Tenderness along the ligament on the inside. Injuries to this ligament tend to occur Stiffness. when a person is bearing weight and the Swelling and some bruising. knee is forced inwards, such as slipping depending on the grade of the injury. on ice or playing sports, e.g. skiing, You may have the feeling the knee will football and rugby. In older people, this give way or some unstable feeling can be injured during a fall. An MCL injury can be a partial or complete tear, or overstretching of the ligament. Knee ligament injuries are also referred to as sprains. It’s common to injure one of your cruciate ligaments (the two ligaments that cross in the middle of your knee which help to stabilise), or your meniscus (cartilage discs that help provide a cushion between your thigh and shin bone), at the same time as your MCL. -

ERAS for Hip and Knee (THA and TKA) Arthroplasty – a Need to Look Beyond LOS
ASERalert November 2016 | Volume 1, Issue 1 ERAS for Hip and Knee (THA and TKA) Arthroplasty – A Need to Look Beyond LOS OFFICIAL also in this issue PUBLICATION OF ERAS for Total Enhanced ERAS for Spine Joint Arthroplasty: Recovery for Surgery: A New Past, Present and Orthopedic Frontier ASER ALERT • VOLUME 1, ISSUE 1 • aserhq.org Future Surgery 1 ANNUAL CONGRESS OF ENHANCED RECOVERY AND 2017 PERIOPERATIVE MEDICINE APRIL 27TH-29TH, 2017 HYATT REGENCY WASHINGTON ON CAPITOL HILL 400 NEW JERSEY AVE NW, WASHINGTON, D.C. 20001 For more information please visit www.aserhq.org 2 ASER ALERT • VOLUME 1, ISSUE 1 • aserhq.org Board of Directors President’s Message Officers By Tong J (TJ) Gan, MD, MHS, FRCA, President President Tong J (TJ) Gan, MD, MHS, FRCA President-Elect Julie Thacker, MD t is my great pleasure to announce Vice-President the inaugural issue of the ASER Timothy Miller MB, ChB, FRCA Newsletter. Founded in 2014, Treasurer ASER is a multi-specialty nonprofit Roy Soto, MD Iorganization with an international Secretary membership and is dedicated to the Stefan D. Holubar MD, MS, FACS, FASCRS practice of enhanced recovery in the perioperative patient through education Directors and research. We are experiencing a period of tremendous expansion and Keith A. (Tony) Jones, MD growth, as is evidenced by the great Anthony Senagore, MD interest to implement the enhanced Maxime Cannesson, MD, PhD recovery pathway in hospitals around Terrence Loftus, MD, MBA, FACS the country. Andrew Shaw MB, FRCA, FFICM, FCCM Desiree Chappel, CRNA The ASER Mission is to advance the practice of perioperative enhanced recovery and to contribute to its pathways. -

Patient Education Total Knee Arthroplasty
Patient Education Total Knee Arthroplasty Explanation of Diagnosis and Procedure The knee is the largest joint in the body. Normal knee function is required to perform most everyday activities. The knee is made up of the lower end of the thighbone (femur), which rotates on the upper end of the shin bone (tibia), and the kneecap (patella), which slides in a groove on the end of the femur. Large ligaments attach to the femur and tibia to provide stability. The long thigh muscles give the knee strength. Normal Knee Anatomy The joint surfaces where these three bones touch are covered with articular cartilage, a smooth substance that cushions the bones and enables them to move easily. Medical Illustration © 2012 Nucleus Medical Media, Inc. All remaining surfaces of the knee are covered by a thin, smooth tissue liner called the synovial membrane. This membrane releases a special fluid that lubricates the knee, reducing friction to nearly zero in a healthy knee. Normally, all of these components work in harmony. But disease or injury can disrupt this harmony, resulting in pain, muscle weakness, and reduced function. Knee with Arthritis The most common cause of chronic knee pain and disability is arthritis. Osteoarthritis, rheumatoid arthritis, and traumatic arthritis are the most common forms of this disease. • Osteoarthritis usually occurs in people 50 years of age and older and often in individuals with a family history of arthritis. The cartilage that cushions the bones of the knee softens and wears away. The bones then rub against one another, causing knee pain and stiffness. • Rheumatoid arthritis is a disease in which the synovial membrane becomes thickened and inflamed, producing too much synovial fluid that overfills the joint space. -
Modern Advances in Joint Replacement and Rapid Recovery
Modern Advances in Joint Replacement and Rapid Recovery UCSF Osher Mini-Med School Lecture Series Jeffrey Barry, M.D. Assistant Professor of Orthopaedic Surgery Division of Adult Reconstruction University of California, San Francisco Disclosures . No relevant disclosures to this talk About Me . Bay Area Native . UCSF - U Can Stay Forever Outline . Burden of Disease and Epidemiology . The Basics of Hip and Knee Replacement . What’s improving over the last decade - Longevity - Pain Management - Hospital Stay - Thromboembolism prophylaxis - Risk Reduction Question What is the most common inpatient surgery performed in the US? 1. Percutaneous coronary angioplasty 2. Total hip replacement 3. Lumbar Laminectomy 4. Appendectomy 5. Total knee replacement Burden of Disease . Arthritis = most common cause of disability in the US . 22.7% of adults have doctor-diagnosed arthritis - 43.2% of patients with arthritis report activity limitations due to disease . By 2030: - 3.5 million TKA (673%) - 570,000 THA (174%) . Curve updated 2014 – just as predicted! Causes of Increased Utilization . Aging Population . Patients receiving arthroplasty at a younger age - Improvements in technology - Obesity Why Replace a Joint? Arthritis arthro – joint itis – inflammation What is Arthritis – Disease of Cartilage . Cartilage Degeneration - Pain - Limp - Swelling - Loss of range of motion - Eventual deformity Arthritis Affects on Your Life • Quality of Life • Independence • Movement, Walking, Exercise • Self-image • Self-esteem • Family Life • Sleep • Everything and Everybody Causes of Arthritis . Osteoarthritis - “wear and tear” . Inflammatory arthritis . Trauma, old fractures . Infection . Osteonecrosis - “lack of oxygen to the bone” . Childhood/ developmental disease Diagnosis . Clinical Symptoms + Radiographic . Radiographs – Standing or Weight bearing! . MRI is RARELY needed!!! - Expensive - Brings in other issues - Unnecessary treatment - Unnecessary explanations Knee Arthritis . -

Knee Joint Distraction Compared with Total Knee Arthroplasty a RANDOMISED CONTROLLED TRIAL
KNEE Knee joint distraction compared with total knee arthroplasty A RANDOMISED CONTROLLED TRIAL J. A. D. van der Woude, Aims K. Wiegant, Knee joint distraction (KJD) is a relatively new, knee-joint preserving procedure with the R. J. van Heerwaarden, goal of delaying total knee arthroplasty (TKA) in young and middle-aged patients. We S. Spruijt, present a randomised controlled trial comparing the two. P. J. E m ans , Patients and Methods S. C. Mastbergen, The 60 patients ≤ 65 years with end-stage knee osteoarthritis were randomised to either F. P. J. G. Lafeber KJD (n = 20) or TKA (n = 40). Outcomes were assessed at baseline, three, six, nine, and 12 months. In the KJD group, the joint space width (JSW) was radiologically assessed, From UMC Utrecht, representing a surrogate marker of cartilage thickness. Utrecht, The Netherlands Results In total 56 patients completed their allocated treatment (TKA = 36, KJD = 20). All patient reported outcome measures improved significantly over one year (p < 0.02) in both groups. J. A. D. van der Woude, MD, At one year, the TKA group showed a greater improvement in only one of the 16 patient- PhD, Resident in Orthopaedic Surgery, Limb and Knee related outcome measures assessed (p = 0.034). Outcome Measures in Rheumatology- Reconstruction Unit, Department of Orthopaedic Osteoarthritis Research Society International clinical response was 83% after TKA and 80% Surgery after KJD. A total of 12 patients (60%) in the KJD group sustained pin track infections. In the R. J. van Heerwaarden, MD, PhD, Orthopaedic Surgeon, KJD group both mean minimum (0.9 mm, standard deviation (SD) 1.1) and mean JSW (1.2 mm, Limb and Knee Reconstruction Unit, Department of SD 1.1) increased significantly (p = 0.004 and p = 0.0003). -

Medical Terminology Abbreviations Medical Terminology Abbreviations
34 MEDICAL TERMINOLOGY ABBREVIATIONS MEDICAL TERMINOLOGY ABBREVIATIONS The following list contains some of the most common abbreviations found in medical records. Please note that in medical terminology, the capitalization of letters bears significance as to the meaning of certain terms, and is often used to distinguish terms with similar acronyms. @—at A & P—anatomy and physiology ab—abortion abd—abdominal ABG—arterial blood gas a.c.—before meals ac & cl—acetest and clinitest ACLS—advanced cardiac life support AD—right ear ADL—activities of daily living ad lib—as desired adm—admission afeb—afebrile, no fever AFB—acid-fast bacillus AKA—above the knee alb—albumin alt dieb—alternate days (every other day) am—morning AMA—against medical advice amal—amalgam amb—ambulate, walk AMI—acute myocardial infarction amt—amount ANS—automatic nervous system ant—anterior AOx3—alert and oriented to person, time, and place Ap—apical AP—apical pulse approx—approximately aq—aqueous ARDS—acute respiratory distress syndrome AS—left ear ASA—aspirin asap (ASAP)—as soon as possible as tol—as tolerated ATD—admission, transfer, discharge AU—both ears Ax—axillary BE—barium enema bid—twice a day bil, bilateral—both sides BK—below knee BKA—below the knee amputation bl—blood bl wk—blood work BLS—basic life support BM—bowel movement BOW—bag of waters B/P—blood pressure bpm—beats per minute BR—bed rest MEDICAL TERMINOLOGY ABBREVIATIONS 35 BRP—bathroom privileges BS—breath sounds BSI—body substance isolation BSO—bilateral salpingo-oophorectomy BUN—blood, urea, nitrogen