Infant Mortality Within Cleveland: an In-Depth Analysis (2012 – 2015)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

OB News August 2012 FINAL.Qxd
August 2012 Volume 34 Number 6 www.oldbrooklynconnected.com Brooklyn Centre to celebrate its bicentennial Photo by Stanislav Zadnik by Brian Cummins James Fish was the first permanent Councilman Ward 14 American settler of Brooklyn Township. He From Indian trails to treaties, oxen to came from Groton, Connecticut with his rattle snakes, stagecoach routes to freeways, family and two of his cousins, Moses and and steel mills to watersheds, on the week- Ebenezer Fish. They were accompanied by end of August 10th to 12th, Brooklyn Centre two other families from Groton and they will be celebrating 200 years of pioneers and traveled by oxen and a lumber wagon. a rich history in recognition of the neighbor- The Fish family arrived in the area of hood’s bicentennial. (See the box on page 3 Newburg in early autumn of 1811 and win- for details about all of the events.) tered in Newburg. Early in the spring of It’s a little known 1812, James crossed fact that Brooklyn the Cuyahoga River Centre, settled in 1812, alone and put up a log was already the center house on what is now of Brooklyn Township the northwest corner of Pearl Rd. and when it was formed in Both the Polish organizations and approximately 600 members of the community showed up Mapledale Ave. 1818, hence its name. for the re-opening Mass at St. Barbara Catholic Church, 1505 Denison Ave., on Sunday, July It has the distinction of being the oldest set- By 1818, over 200 people were living 22nd. In this photo of the outdoor portion of the ceremony, pastor Fr. -
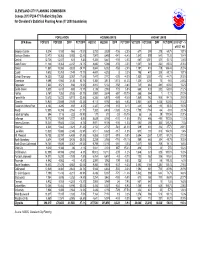
Census 2010 PL94-171 Redistricting Data for Cleveland's Statistical Planning Areas (Yr 2000 Boundaries)
CLEVELAND CITY PLANNING COMMISSION Census 2010 PL94-171 Redistricting Data for Cleveland's Statistical Planning Areas (Yr 2000 boundaries) POPULATION HOUSING UNITS VACANT UNITS SPA Name POP2010 POP2000 DIFF PCT DIFF HU2010 HU2000 DIFF PCT DIFF VCT2010 VCT2000 DIFF PCT DIFF 2010 VCT - % of TOT HU Brooklyn Centre 8,214 9,180 -966 -10.5% 3,733 3,839 -106 -2.8% 677 399 278 69.7% 18.1% Buckeye-Shaker 12,470 16,063 -3,593 -22.4% 7,947 8,488 -541 -6.4% 1,540 899 641 71.3% 19.4% Central 12,738 12,107 631 5.2% 5,306 5,441 -135 -2.5% 680 1,001 -321 -32.1% 12.8% Clark-Fulton 11,126 13,363 -2,237 -16.7% 4,890 5,066 -176 -3.5% 1,007 543 464 85.5% 20.6% Corlett 11,581 15,384 -3,803 -24.7% 5,844 6,002 -158 -2.6% 1,197 418 779 186.4% 20.5% Cudell 9,612 10,761 -1,149 -10.7% 4,401 4,393 8 0.2% 795 470 325 69.1% 18.1% Detroit-Shoreway 14,325 17,382 -3,057 -17.6% 7,447 7,772 -325 -4.2% 1,530 1,057 473 44.7% 20.5% Downtown 9,098 5,960 3,138 52.7% 5,386 3,813 1,573 41.3% 1,325 1,255 70 5.6% 24.6% Edgewater 7,633 8,571 -938 -10.9% 4,910 5,102 -192 -3.8% 745 464 281 60.6% 15.2% Euclid-Green 5,533 6,413 -880 -13.7% 3,136 2,963 173 5.8% 665 433 232 53.6% 21.2% Fairfax 5,167 7,352 -2,185 -29.7% 2,987 3,674 -687 -18.7% 865 864 1 0.1% 29.0% Forest Hills 10,612 15,723 -5,111 -32.5% 6,306 6,875 -569 -8.3% 1,869 963 906 94.1% 29.6% Glenville 15,940 23,559 -7,619 -32.3% 9,112 9,792 -680 -6.9% 2,861 1,405 1,456 103.6% 31.4% Goodrich-Kirtland Park 4,103 4,295 -192 -4.5% 2,327 2,194 133 6.1% 441 326 115 35.3% 19.0% Hough 12,805 16,359 -3,554 -21.7% 7,382 8,408 -1,026 -12.2% 1,700 1,764 -64 -3.6% 23.0% Industrial Valley 894 1,116 -222 -19.9% 177 210 -33 -15.7% 55 26 29 111.5% 31.1% Jefferson 18,172 19,949 -1,777 -8.9% 8,629 8,760 -131 -1.5% 976 486 490 100.8% 11.3% Kamms Corners 18,241 19,545 -1,304 -6.7% 8,971 9,106 -135 -1.5% 653 290 363 125.2% 7.3% Kinsman 4,021 5,842 -1,821 -31.2% 2,154 2,737 -583 -21.3% 519 631 -112 -17.7% 24.1% Lee-Miles 13,820 15,866 -2,046 -12.9% 6,511 6,628 -117 -1.8% 613 300 313 104.3% 9.4% Mt. -

Brooklyn YMCA to Close; Building to Be Sold
28 YEARS OF SERVING THE COMMUNITY OldOld BrooklynBrooklyn NewsNews A Publication of the Old Brooklyn Community Development Corporation, Cleveland, Ohio www.oldbrooklyn.com June 2006, Volume 28 Number 4 Brooklyn YMCA to close; building to be sold by Sheila Long No. It’s a done deal. We have long-time [email protected] employees — Debbie Natal at the desk; she’s been here for ten years. She sat at the table and said, `This isn’t a job; this is part of After a half century of service to my family.’ What do you say to her? I have Brooklyn Centre, Old Brooklyn and sur- been a member for 34 years.” rounding neighborhoods, the Brooklyn Despite Boester’s obvious shock and YMCA on Pearl Road will be closing its concern, he acknowledged that Haley’s doors and put on the market for sale. assessments of the financial forecast for the Glenn Haley, the president and CEO of the Brooklyn Y were grim and somewhat com- YMCA of Greater Cleveland made the pelling. public announcement on Tuesday, May 30. “In terms of a membership,” Haley The Downtown YMCA also will be said. “You have a 60,600 square-foot facili- placed up for private sale but will continue ty that has 519 membership units. To main- as a membership branch in a contingency tain the organization and the operations, the of sale lessee relationship with the buyer. Brooklyn Y would need 2200-2500 mem- In a May 30 letter to the Brooklyn Y’s bership units just to sustain it. Over the last membership (the first notice that members Photo by Sandy Worona two years, we’ve got it up by barely 100 and received of any potential closure), Haley that is not sufficient.” wrote: In 1919, Karl Kist founded the Brooklyn branch of the YMCA; its first home was a second- floor office (with one phone) at 4145 Pearl Road shared with the YWCA and the editor of the Fiscal woes have plagued the YMCA of “The Brooklyn YMCA will be placed Brooklyn News. -

W25 Transit Development Strategy
w25 transit development strategy Community Planning Process Final Report | April 2015 Cover Photograph: W25 Aerial Courtesy Bing Maps & Cleveland Neighborhood Progress © 2015 Microsoft Corporation Participants Cleveland Neighborhood Progress Steering Committee Public Meeting Participants Daniel Brown | Evelyn Burnett | Ayden Ergun Sara Byrnes Maier | George Cantor | Joe Anthony Alto | Ingrid Angel | Shelly Belak Peter Moser | John Motl | Rosemary Mudry | Justin Fleming | Lynn Friedel | Jeff Kipp Cimperman | Fred Collier | Gerardo Colon | Anthony Brancatelli | Millie Caraballo | | Eduardo Munoz | Scott Nagy | Lourdes | Emily Miller | Wayne Mortensen | Zoe | Jenice Contreras | John Corlett | Glenn Salathiel Carter | Tom Collins | Alice Colon Negron-McDaniel | Ryan Noles | Mary Rose Mueller | Joel Ratner | Wendy Sattin | Linda Coyne | Brian Cummins | Rob Curry | Tim | Suzanne Davidson | Jaime Declet | Sandra Oahar | Alexandra Pagan | Selina Pagan | Warren Donovan | MariBeth Feke | Anne Hill | Kevin DelValle | Cynthia Fareed | Lydia Fernandez Greg Peckham | Marilyn Pena-Bagley | Ken Kelley | Donald Malone | Mark McDermott | | Rick Foran | Alan Forman | Vince Frantz Pendergast | Jason Powers | Matt Provolt Parsons Brinckerhoff Tom McNair | Juan Molina Crespo | Wayne | Camille Garcia | Bob Gardin | Janice | Nelson Ramirez | Paul Rentas | Elizabeth Ken Liwag | Caroline Nardi | Tim Rosenberger Mortensen | Zoe Mueller | Scott Pollock | Gonzalez | Keisha Gonzalez | Kristie Groves Richards | Barbara Riley | Erick Rodriguez Jeff Ramsey | Joel Ratner -

Clark-Fultonclark Elem Meeting Hall ! R CLARK AV !
å å Walton Elem Ceska Sin Sokol D West 25th/Clark Retail District Clark-FultonClark Elem Meeting Hall ! R CLARK AV ! å FIRE COMPANY 24 N Æc O ²µ T Community Assets - 2006 L U F å Buhrer Elem Legend Merrick House ! D R Cleveland Municipal Schools å St Rocco Elem N kj O kj Other Schools Lincoln-West High T N å A Miscellaneous R C S EMS ²µ Fire Luther Memorial Elem ! # Health kj Meyer Pool Metro Lofts qÆ Hospital ! Parks (see below) _ Police Steelyard Commons ! Service Shopping Center ! Utilities Æc Library EMS (2005) METROHEALTH MEDICAL CENTER Parks qÆ EMS (2005) Historic District 2ND DISTRICT POLICE HQ ENGLINDALE _ Jones Children Home ! ! Milford Place Æc D Riverside Cemetery EN I ! SO N AV y a w Brooklyn Centre Historic District y B y Æc a w l a Brookside Park T n S a ! H Y C T K 5 E P 2 Aerial: Airphoto USA 2005 & N W O O T L U F T S Clark-Fulton V D N A R I RA Connecting Cleveland3 L O2020 Citywide Plan - Retail District Strategies 7 Cudell W Detroit-Shoreway Ohio City CLARK AV Clark-Fulton T S - Focus redevelopment efforts on West 25th/ H T Clark intersection 5 T 6 - Redevelop vacant & underutilized buildings S and properties D W R - Develop streetscape enhancement plan for 3 7 portions of Clark Ave and West 25th St Tremont - Consolidate Latino-oriented businesses on W West Boulevard West 25th St into regional retail destination D R N D O R T T N S N O A Clark-Fulton H T R L T C U 5 F 2 S Stockyards W - Establish consolidated retail district centered around K-Mart Plaza along West 65th St between West 67th Pl and West 65th St - -

Big Creek Watershed News & Notes
December 2020 Big Creek Watershed News & Notes YEAR END REPORT RECAP OF 2020 s 2020 comes to a close, we want share with you some of our accomplishments during the year A and to thank you for your ongoing support. With the COVID-19 pandemic, this has been a challenging year. We have been limited with scheduling clean-ups and other events involving or engaging with the community. And most of our popular stream monitoring programs with local school students have been put on hold. However, we have continued to work with West Creek Conservancy, Cleveland Metroparks, the Northeast Ohio Regional Sewer District, and other partners on our stream restoration and green infrastructure projects. In this newsletter, we update you on some of those projects, showcase our watershed signage project, explore how stormwater in our watershed functions, and provide a guide for our year ahead. We also want to thank our supporters for the work we’ve been able to accomplish and wish everyone a healthy and prosperous new year. GREEN INFRASTRUCTURE AND STREAM RESTORATION UPDATES he Caribe Bakery Green Infrastructure Project is nearly complete, while groundbreaking for the T Barrio Distribution Center Green Campus project should begin in the fall of 2021. Under management by project partner West Creek Conservancy, the Stickney Creek Restoration project in Brooklyn’s Memorial Park should be breaking ground in February. Cleveland Metroparks’ Brookside parking lot project will break ground in the spring, where bioretention cells will manage stormwater runoff entering Big Creek. BCC is playing a small part in the project with financial assistance and outreach efforts. -
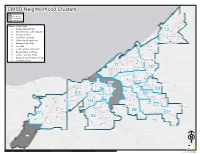
Number Cluster Name 01 Kamm's
CCMMSSDD NNeeiigghhbboorrhhoooodd CClluusstteerrss Oliver H Perry Cleveland Boundary " Cluster Boundary 2012 SPA Boundary North Shore Collinwood 2014 Ward Boundary Memorial " Hannah Gibbons Number Cluster Name " 01 Kamm's - Bellaire-Puritas Ginn Academy 1122 " 02 Detroit Shoreway - Cudell - Edgewater Collinwood-Nottingham 03 Ohio City - Tremont East Clark " Collinwood College Board Academy Euclid Park 04 Clark-Fulton - Stockyards " " Euclid-Green 05 Old Brooklyn - Brooklyn Center Iowa-Maple " Kenneth W Clement Boys' Leadership Academy 06 Broadway - Slavic Village " Glenville Career and College Readiness Academy 07 Lee - Miles " Franklin D Roosevelt 08 Central - Kinsman - Mt. Pleasant " Glenville Patrick Henry 09 Buckeye-Shaker - Larchmere " Michael R White STEM " 10 Glenville - University - Fairfax St.Clair-Superior Willson 11 Downtown - St. Clair-Superior - Hough " Cleveland School of the Arts at Harry E. Davis " Mary M Bethune East Professional Center " 12 Collinwood - Euclid " Daniel E Morgan Wade Park " Case " " Hough 1111 Goodrich-Kirtland Pk Martin Luther King Jr " Mary B Martin School SuccessTech Academy Design Lab - Early College @ Health Careers " MC2STEM " " 1100 Downtown" University Campus International School " John Hay- Cleveland School of Science and Medicine John Hay - Cleveland Early College High School "John Hay - Cleveland School of Architecture and Design George Washington Carver STEM " Marion-Sterling "Jane Addams Business Careers Center Fairfax " Bolton Alfred A Benesch " Central " East Tech Community Wraparound " -

Brooklyn Centre Neighborhood Plan Summary
BROOKLYN CENTRE NEIGHBORHOOD PLAN SUMMARY Description. Brooklyn Centre became a part of Cleveland with the annexation of Brooklyn Village in 1894. Although first settled in the 1820s along Pearl Street, the lifeline to Cleveland, a substantial business district developed around the intersection of Pearl and Denison after the extension of a streetcar line 1869. The oldest remaining houses in Brooklyn Centre date from the middle of the 19th century. Most residential development occurred, however, after annexation between 1900 and 1915 and is a mix of one- and two-families and small multi-family buildings. Pearl Road is still the neighborhood’s main commercial street and industrial uses are located in and near the Big Creek Valley and Cuyahoga River. Assets. Among the neighborhood’s most significant assets are: • MetroHealth Medical Center which is one of the region’s main trauma centers • historic residential and commercial buildings and Riverside Cemetery which form the basis for the Brooklyn Centre Historic District • Pearl Road retail including Aldi’s and the Brooklyn Centre Shopping Center • good freeway access to interstate 71 and state route 176 • proximity to Brookside Reservation and the Metroparks Zoo Challenges. Among the challenges faced by the Brooklyn Centre neighborhood today are: • physical condition of apartment buildings and absentee-owned single and two-family homes on residential side streets • vacant former Brooklyn YMCA building on Pearl Road at Seltzer Avenue • poor condition of streetscape along West 25th Street and Denison Avenue • lack of direct access to Lower Big Creek Valley and Ohio & Erie Canal Towpath Trail • hillside subsidence and ongoing property loss along rim of Lower Big Creek Valley Vision. -

OB NEWS MARCH 08 FINAL.Qxd
Old Brooklyn Community Development Corporation Old Brooklyn News Serving Old Brooklyn, Brooklyn Centre & surrounding areas for 30 years www.oldbrooklyn.com March 2008 Volume 30; Number 1 Old Brooklyn News marks thirty years by Lynette Filips [email protected] of serving the community With the publication of this March about the upcoming annual meeting were mailed to them, but other folks had to pick issue, the Old Brooklyn News marks its 30th also on page one. one up at neighborhood churches and busi- anniversary. While there won’t be a big cel- On page two, in addition to two smaller nesses. ebration like the one the Old Brooklyn articles, the pastor of Brooklyn Presbyterian Home delivery of the OBN started in Community Development Corporation Church wrote about his congregation’s sev- December, 1978; that issue billed the paper (OBCDC) hosted in April of 2006, six entieth anniversary. (That’s one similarity, as being published “approximately” every months after its thirtieth anniversary, a little since we just carried a story about their one- other month. (May, 2007 was the last nostalgia and historical perspective still hundredth anniversary in last month’s month for home delivery, but as in the seems to be in order. After all, OBCDC is OBN.) past, OBCDC members receive a copy by the only community development corpora- Deaconess Hospital was a major stake- mail.) tion in the city which has its own monthly holder in the neighborhood in those days, in In May, 1981, the month that newspaper! terms of providing advertising dollars for the OBCDC accomplished its goal of pur- Although there had been local newspa- paper and support for the community devel- chasing the Broadvue Theatre, the Old pers covering this neighborhood during pre- opment corporation in general. -

Cleveland 2014 SPA's
M a C p le l vel e and c l iff R Ca d nter bury Rd In La g nd le see si W r R de ind d R w d ard Rd T E a as H Pawnee Ave rr t iller 2 ym P Sc Ave 01 a h 4 e SP o r n Mohawk Ave A k e 's r l y e D Har Av R r land e d Ave Arrowhead Ave Cherokee Ave Kildeer Ave Bellaire-Puritas V ir gi Rd nia on A ert t v g Kewanee Ave S e Ed Nor h th t V Broad Il Rd 7 way l se -S 9 lavic Village a Ree A 1 n g E e E l S hore a G r 2 D le a D 0 Bro n ll 0 o r e klyn C f en i B t t re e ld h Rd S t C t S ollinwood n w Rd ro t B B w uckey S e-S e haker Squ i are v h la t l Vi 8 6 Pythias Ave 1 C D h t elav ard E an on B S Av R uckeye-Woodhill e d h t O Grovewood Ave 0 t v 7 C e 1 t o r Parkgrove Ave l B l a o S E f o f o C h u entra n l t k Huntmere Ave B n D 7 P i e 6 a acauley Ave E t a M w 1 l rcade Ave C A w r e o k 1 v k E o 6 A o c D Ridpath Ave o e a d 5 s r Ir y d rafalgar Ave C T t o lar k-Fu u n lt h on D w c N oo D a d r Lucknow Ave S r Ave r y t S E d d Shasta Ct 1 R 7 R 9 t Upton Ave t s d d h r Co t llinwood o - Not R t u in o g S ha m S e t v h d Jean A rw h i o n t F o e iel Ave 5 w n P Westropp Ave a 8 d D e 1 R Cud C ell E d R l Hale Ave loo e er r at m W d S o R E loo n Othello Ave er t at 1 W R Cuyahoga V Thames Ave 7 alley 1 d s E t Darwin Ave S 1 t 7 t 2 S Jenne Ave n d d D Diana Ave etroit n Shoreway S t 2 t d S Darley Ave c R 6 ta a 1 in an P r E e Kelso Ave Sa v A Downtow e n Argus Ave n la Eaglesmere Ave P C Kuhlman Ave a Col t Ed linwood-Nottin a ge gh d wa am l te E r p e A R a v Pepper Ave t A 1 W lh d R al 5 a n d ob 6 h m la -

Ward 12 News ~ Winter 2019, Council Member Anthony Brancatelli
Ward 12 News Anthony Brancatelli, Councilman | WINTER 2019 | www.clevelandcitycouncil.org A message from Come Out for Councilman Brancatelli Super Saturday SUPER SATURDAY Dear Ward 12 neighbor: Get your taxes prepared free by Free Tax Prep Event! I wish you and your an IRS-certified volunteer WHEN: families a happy and On Saturday, February 16, the Cuyahoga EITC February 16, 2019 • 9:00 am - 3:00 pm prosperous New Year. Coalition will provide FREE tax preparation LOCATION: Last spring our at Cleveland Central Catholic High School Cleveland Central Catholic High School, neighborhood of (6550 Baxter Ave.), 9:00 am - 3:00 pm. Radio 6550 Baxter Ave. Brooklyn Centre on station Z 107.9 will be broadcasting live and the west side of the on location from 10:00 am to noon. This event ward finally saw the is done in partnership with Neighborhood demolishing of the Housing Services of Greater Cleveland and YMCA building and adjacent vacant Third Federal Savings & Loan. factory building on Pearl Road. Soon we Be sure to visit www.refundohio.org or will see a $12 million investment of a 71- call 2-1-1 for more information about this unit apartment on the site. We also held and other upcoming tax preparation events and to schedule an appointment. a ribbon cutting celebrating the long awaited opening of W.C. Reed Field WHAT TO BRING FOR SUPER SATURDAY: 3 Bank account and routing number if Park, off Denison Avenue. 3 Government issued photo ID using direct deposit to receive tax refund In the Tremont neighborhood, work 3 Social Security or ITIN cards for each 3 Child care provider information is underway for Stage 3 of the Towpath person on the tax return Trail, which will extend the trail 1.9 3 Last year’s tax return if possible miles from Steelyard Commons to 3 All income documents such as W2’s, Literary Avenue. -

Brooklyn Centre Celebrates 200 Years of Pioneers Brooklyn Centre
Summer 2012 Ward 14 News Serving Brooklyn Centre, Clark Fulton and portions of the Stockyard, Tremont and Ohio City Neighborhoods Brooklyn Centre Celebrates 200 Years of Pioneers This year marks 200 years, 1812 – 2012, since the arrival of the first clearing the forest and developing a village progressed, and the area American settlers on the western bank of the Cuyahoga River, in the from the Big Creek to Scranton Road became the center of Brooklyn neighborhood that we now know as Brooklyn Centre. Township. On June 1, 1818, Brooklyn Township was formally orga- The Community is commemorating its Bicentennial with exciting ac- nized. The village of Brooklyn served as the center of the township until tivities designed to bring neighbors together through celebratory events the early 1830s. Through the late 1830s, the neighborhood was known (see “Bicentennial Events,” on page 2), and to educate and encourage as Brooklyn Centre, and was where the region’s settlers came to vote, local residents and businesses to make physical improvements through- attend church, and purchase goods. out the neighborhood. The Bicentennial started on Memorial Day, with a ceremony at the From Annexation to the Twentieth Century Brooklyn Centre Burying Grounds, located at 2300 Garden Avenue, be- hind Aldi’s. The Brooklyn Centre Burying Ground’s first interment was From the 1830s until its annexation to Cleveland in 1867, Brook- in 1823, and the cemetery was deeded with the name Brooklyn Centre lyn Centre was a fashionable suburb between the forests, farmlands and when it was founded in 1835. Memorial Day ceremonies have taken small towns to the South and the growing city of Cleveland to the north.