Resin-Bonded Bridges − the Problem Or the Solution?: Part 1 Assessment and Design
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

February 2018 (PDF File)
Member Newsletter BSSPD Annual Conference 15th/16th March 2018 Photograph: Dr. Alejandro Umanzor at Unidad de Prostodoncia Dental Pensando a future. The British Society of Prosthodontics Newsletter, Volume 24, February 2018 President’s Editorial Phil Smith I’m delighted to welcome you to the latest edition of the newsletter of the British Society of Prosthodontics. I am pleased to report that the Society has been active on several fronts over the past year. One of our functions is the delivery of suitable platform to allow Council education and CPD opportunities in Discussions to take place online without Prosthodontics and related disciplines. the need for face to face meetings. This is One way we fulfil this important gaining more importance as in recent commitment is through our annual series times it has become difficult and of Webinars. We are fortunate to have increasingly expensive for Council to take been able to assemble an impressive line- time away from clinics. We have had a up of presenters who provided our series of ‘screen tests’ and have found a members with invaluable learning updates platform that suits our needs and hopefully in a wide range of contemporary this will allow Council to become better Prosthodontic and related topics. The connected when we need to work on your Webinars attract many participants but behalf. there are some members who have yet to experience them and I would encourage BSSPD current and future Presidents have you all to sample some of them. You will also been involved in initial discussions to need to sign up to join our live Webinars, explore how we can work closer with RD- but all members are able to access our UK and BSRD on areas of mutual benefit. -
Resin-Bonded Bridges − the Problem Or the Solution? Part 1: Assessment and Design
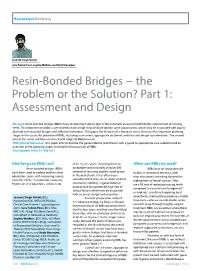
RestorativeDentistry Jasneet Singh Gulati Sara Tabiat-Pour, Sophie Watkins and Avijit Banerjee Resin-Bonded Bridges − the Problem or the Solution? Part 1: Assessment and Design Abstract: Resin-bonded bridges (RBBs) have an important role to play in the minimally invasive prosthodontic replacement of missing teeth. This treatment modality is perceived to have a high clinical failure rate by some practitioners, which may be associated with poorly planned and executed designs and adhesive techniques. This paper, the first part of a two-part series, discusses the important planning stages in the successful provision of RBBs, including assessment, appropriate abutment selection and design considerations. The second part of this series will focus on the clinical stages of RBB provision. CPD/Clinical Relevance: This paper aims to provide the general dental practitioner with a guide to appropriate case selection and an overview of the planning stages involved for the provision of RBBs. Dent Update 2016; 43: 506–521 How long can RBBs last? of 87.7% at 5 years,2 deeming them an When can RBBs be used? Resin-bonded bridges (RBBs) acceptable and minimally invasive (MI) RBBs have an important role have been used to replace teeth in short method of restoring modest-sized spaces to play in restorative dentistry, with edentulous spans with increasing success in the dental arch. It has often been their indications extending beyond the since the 1970s.1 A systematic review by considered that they are an under-utilized replacement of lateral incisors. They -

Effect of Placing Intentionally High Restorations: Randomized Clinical Trial
Journal of Dentistry 45 (2016) 26–31 Contents lists available at ScienceDirect Journal of Dentistry journal homepage: www.intl.elsevierhealth.com/journals/jden Effect of placing intentionally high restorations: Randomized clinical trial a b c, Olga Gerasimidou , Timothy Watson , Brian Millar * a Restorative Dentistry, King’s College London Dental Institute, London, United Kingdom b Biomaterials & Restorative Dentistry, King’s College London Dental Institute, London, United Kingdom c Primary Dental Care, King’s College London Dental Institute, London, United Kingdom A R T I C L E I N F O A B S T R A C T Article history: Objective: The aim of this study was to examine the behavior of posterior teeth restored with single-tooth Received 23 October 2014 restorations with intentionally high occlusal contacts. Received in revised form 2 November 2015 Methods: Consent was obtained from 17 patients who were seen a total of 5 times over 3.5 years. The Accepted 21 November 2015 restorations placed were all full occlusal coverage gold restorations. Tooth mobility was recorded using the Periotest device and tooth movement was determined from impressions and 3D imaging. Patients Keywords: were randomly assigned into two groups, the control group which received restorations with no Prosthetic dentistry/prosthodontics intentional increase of the occlusal vertical dimension; or the treatment group where they received Occlusion intentionally high restorations in 0.5 mm supraocclusion. Clinical outcomes Results: Statistical analysis showed no significant difference in mobility between visits for both the Oral rehabilitation fi Orthodontic tooth movement control and the treatment groups while a signi cant dependency and difference in tooth movement was Remodeling observed between the subjects of the two groups. -

Tooth Wear Exeter 100613
TTooootthh WWeeaarr Solutions for Success Techniques & Materials for dealing with worn teeth Notes to accompany the practical course for General Dental Practitioners at Exeter On Tuesday 10 th June 2013 Tutor: Brian Millar BDS, FDSRCS, PhD, FHEA Professor, Consultant in Restorative Dentistry Specialist in Prosthodontics and Restorative Dentistry Director of MClinDent (Prosthodontics) by Distance Learning Programme Director for Prosthodontics and Aesthetic Dentistry MClinDent/MSc Flexible Programmes Further info: [email protected] or [email protected] www.kcl.ac.uk/distancedentistry For further information on the KCL blended learning programmes: http://www.kcl.ac.uk/distancedentistry or email [email protected] Kings College London Dental Institute at Guy’s, King’s and St. Thomas’ Hospitals Overview Tooth Surface Loss (Tooth Wear) is an increasing problem and needs to be identified early to enable preventative measures to be put in place. TSL includes all forms of loss of tooth material not due to disease of bacterial origin (ie. caries) and is usually considered to be: Attrition Abrasion Erosion Fractures Developmental defects Dentistry should also be added to the list as we as a profession often cut bits off teeth! Always look for it at patient examination using loupes (eg 3x magnification), bright light and dry teeth. Establish a diagnosis then formulate a plan. The TSL can be monitored using photographs, study models, indices or charts. Check these are dated. The general plan is to apply prevention, monitor and avoid restorative treatment where possible. Active intervention should be non-invasive where possible to prevent further tooth loss. Principles of management: 1. -

Differential Tooth Wear, the Inman Aligner, the Dahl Principle and an Alternative to Preparo- Mental Dentistry?
Clinical excellence with CPD Differential tooth wear, the Inman Aligner, the Dahl principle and an alternative to preparo- mental dentistry? Dr Tif Qureshi, vice president of the BACD, discusses a case using the Dahl principle as a way of creating anterior space in the worn dentition Nowadays, thankfully, far more patients are dealing with Aims and objectives aesthetic issues with alignment techniques, bleaching and To discuss the Dahl principle, using a case presentation, and to bonding alone. Prepping for the sake of prepping seems outline a non-invasive technique that makes occlusal finally to be dying out (hence the title). Veneers, when used, treatments simpler and less complicated. can be far more minimally invasive now and hence much thinner with more predictable bonding to enamel. The principle Introduction Modified Lucia jigs have been used as anterior One of the questions I get asked most while teaching Inman deprogrammers to help the mandible find centric relation. Aligner (IA) therapy is about the use of the Dahl principle in Direct composites can also be used as an anterior some of my cases. In fact, I get asked so often that I decided deprogrammer. Resin composites, because of their resilience to write an article through a case presentation on the subject. and ease of manipulation even in small thicknesses, The Dahl principle is not needed for IA therapy but in represent and ideal material to restore the palatal surface many cases it can help your overall treatment plan. I have (Cardoso, Canbabarro, Myers, 2000) and the worn lower used this principle for over 12 years on probably hundreds of anterior incisal and canine edges too. -

Proposed Generic Heading
King’s Research Portal Document Version Peer reviewed version Link to publication record in King's Research Portal Citation for published version (APA): Gulati, J., Watkins, S., Tabiat-Pour, S., & Banerjee, A. (2016). Resin bonded bridges – the problem or the solution? Part 1 – assessment and design. Dental Update, 43, 506-521. Citing this paper Please note that where the full-text provided on King's Research Portal is the Author Accepted Manuscript or Post-Print version this may differ from the final Published version. If citing, it is advised that you check and use the publisher's definitive version for pagination, volume/issue, and date of publication details. And where the final published version is provided on the Research Portal, if citing you are again advised to check the publisher's website for any subsequent corrections. General rights Copyright and moral rights for the publications made accessible in the Research Portal are retained by the authors and/or other copyright owners and it is a condition of accessing publications that users recognize and abide by the legal requirements associated with these rights. •Users may download and print one copy of any publication from the Research Portal for the purpose of private study or research. •You may not further distribute the material or use it for any profit-making activity or commercial gain •You may freely distribute the URL identifying the publication in the Research Portal Take down policy If you believe that this document breaches copyright please contact [email protected] providing details, and we will remove access to the work immediately and investigate your claim. -

Complex Esthetic a Rehabilitation with P an Additive
DPN CASE REPORT 53 Complexp Esthetic a Rehabilitation with an Additive Minimally Invasive Restorative Approach AUTHOR: DR CHRISTOPHER CK HO, AUSTRALIA www.careimplants.com.au Frontal view of teeth suffering from erosion. The treatment of the patient with extensive tooth wear presents complex challengesenges, due to diagnosis of often a multi-factorial etiology, and the definitive manaanagement of the patient. Patients may seekeek dentald care to improve their esthetic appearance, without fully comprehendinding theth complexity or problems associated with tooth wear. Typical symptoms that patientsp present with include poor esthetics, chipping/thinning of teeth, dentinaldentin hypersensitivity, reduced occlusal vertical dimension, and minimal toothoth heihe ght. Historically the management of patients presentiting withw extensive tooth wear was with conventional fixed prosthodontics. This would involve preparation with crowns on the teeth where tooth structures wereere alreadyal compromised. This would increase the biomechanical risk to the dentitiontition due to the reduction of tooth structures, which negatively impact the structural rigidity of the teeth. Edelhoff and Sorenssen [1] found that 62% to 73% of tooth structure can be removed undertaking the preparation to receiveceive either a full coverage all-ceramic crown or porcelain fuseded to metal crown. Additionally a conventional approach could result inn a losslo of pulpal vitality of the teeth. Teeth requiring fixed prosthesess havehav a 6-11% requirement for endodontic treatment. This approach is moremo invasive and is irreversible. [2, 3] 266 www.dentalnetasia.com CASE REPORT DPN 53 Clinical case overview The patient is a 26-ye6-year-olda female who presents with her chief concernconce being that off the short nature of her teeth and the ensuing poor esthetics.cs A comprcomprehensive history and examination was performed. -
Overcoming Inertia Making a Difference by Doing Things ‘Anybody Can Do’
2014 Journal of the European section international college of dentists Overcoming Inertia making a difference by doing things ‘anybody can do’ COMMITTEES European ICD sponsors Interview with WHO publication Ljubo Marion Phillip Dowell “Contribution to Society” COLOPHON Austria OFFICERS OF THE Belgium EUROPEAN SECTION Mission Bulgaria President The International College of Dentists Croatia Ljubo Marion is a leading honorary dental organi- Cyprus sation dedicated to the recognition President-Elect of outstanding professional achieve- Czech Republic Tom Feeney ment and meritorious service and the Denmark continued progress of the profession England Vice-President of dentistry for the benefit of all man- Corrado Paganelli kind. Estonia Finland Editor Motto Walter van Driel Recognising Service as well as the France Opportunity to Serve. Germany Registrar Greece Argirios Pissiotis Objectives • To provide a universal forum for the Hungary Treasurer cultivation of cordial relations within Iceland Henk Donker the profession. • To foster the growth and diffusion Ireland Immediate Past President of dental knowledge. Israel Henrik Harmsen • To recognise distinguished service Italy to the profession and to the public International Councillors worldwide. Latvia Phillip Dowell • To promote post-graduate study and Lithuania Frans Kroon research in the field of oral health. Luxembourg Argirios Pissiotis • To contribute to the advancement of the profession of dentistry inter- Malta nationally. Moldavia ICDigest • To encourage and support projects of a humanitarian nature. Monaco Editor in Chief • To uphold the highest standard of Montenegro Walter van Driel professional competence and per- Netherlands sonal ethics. Editorial Board • To assist in preserving the highest Norway Gil Alves Alcoforado public perception of the profession. -

The Determinants and Control of Soft Drinks-Incited Dental Erosion
ISSN 1807-5274 Rev. Clín. Pesq. Odontol., Curitiba, v. 5, n. 2, p. 141-154, maio/ago. 2009 Licenciado sob uma Licença Creative Commons THE DETERMINANTS AND CONTROL OF SOFT DRINKS-INCITED DENTAL EROSION Determinantes e controle da erosão dental induzida por refrigerantes CT Bamisea, KA Kolawolb, EO Oloyedec a BChD, FMCDS, Lecturer/Consultant, Department of Restorative Dentistry, Faculty of Dentistry, Obafemi Awolowo University, Ile-Ife, Nigeria, e-mail: [email protected] b BChD, FWACS, Lecturer/Consultant, Department Child Dental Health, Faculty of Dentistry, Obafemi Awolowo University, Ile-Ife, Nigeria. c PhD, Senior Lecturer, Department of Curriculum Studies, Faculty of Education, Obafemi Awolowo University, Ile-Ife, Nigeria. Abstract OBJECTIVE: The aim of this paper has been to review the past and current literature on the determinants and control of soft drinks-incited dental erosion. METHODS: The authors used Medline to find relevant literature published until March 2009. Abstracts and full articles were read to identify studies and reviews describing various modifying factors and determinants of dental erosion. Additional information was obtained using manual library search. RESULTS AND CONCLUSION: Excessive exposure to various acid sources can contribute to the chemical erosion of tooth surfaces. While these acid sources have the potential to erode teeth, various chemical, biological and behavioral factors determines the erosive action of the acids they contain. Several interceptive and preventive means have been proposed to minimize damage to the dentition. Keywords: Dental erosion. Acidic drinks. Modifying factors. Treatment. Resumo OBJETIVOS: O objetivo deste artigo foi revisar a literatura passada e atual sobre os determinantes e controle da erosão dentária induzida por refrigerantes. -

Crowns and Bridges
Planning and Making Crowns and Planning and Making Smith Bridges Howe Crowns and Fourth Edition This highly successful text, which has achieved wide acclaim among practitioners and is a Crowns and Bridges recommended text in the major dental schools, has again been revised and updated to keep it at the forefront of clinical practice. As before, the intention is to help solve real clinical problems by guiding dentists to make the right initial decision and then carry it through. Bridges This new edition includes significantly expanded material on veneers and implants in particular, so as to help dentists advise patients in their choice of what to do and how to make informed choices. FROM REVIEWS OF PREVIOUS EDITIONS: Fourth Edition 'well thought out and exceedingly well presented. I can wholeheartedly recommend this work as a worthwhile addition to any practitioner's bookshelf.' British Dental Review 'the greatest strength of the book lies in the sensible and comprehensive way it provides descriptions of clinical procedures' British Dental Journal Planning and Making 'must be considered a "best buy" for every practitioner interested in a planned approach to crown and bridgework' Dental Update ‘should be on every dentist’s bookshelf’ Dental Practice WITH OVER 600 COLOUR AND BLACK-AND-WHITE PHOTOGRAPHS CONTENTS: Indications and contraindications for crowns • Types of crown • Designing crown preparations • Occlusal considerations • Planning and making crowns • Clinical techniques for making crowns • Indications for bridges compared with partial dentures and implant-retained prostheses • Types of bridge • Components of bridges: retainers, pontics and connectors • Designing and planning bridges • Clinical techniques for bridge construction • Dental implants • Fixed splints • Crown and bridge failures and repairs Bernard GN Smith, BDS, PhD, MSc, MRD, FDSRCSEng, FDSRCSEdin, studied at the Universities of London and Michigan and spent a number of years in general practice. -

The Maltese Dental Journal
ISSUE 75 SEP20 The Maltese Dental Journal ISSN 2076-6181 ® DENTAL ASSOCIATION OF MALTA Variolink Esthetic The Professional Centre, Sliema Road, Gzira The esthetic luting composite Tel: 21 312888 Fax: 21 343002 Editorial Email: [email protected] By Dr David Muscat Dear colleagues, The Dental Profession has St Apollonia Celebration: implemented the Covid guidelines and we have braved the summer. It is rather unfair that we have been TheEarly Years excluded from the 50% reduction in electricity bills. By George E. Camilleri In this issue I have asked a few Oral historical evidence attributes Golden Bay Hotel (Figs 3 & 4). Dental dentists to contribute articles as we the origin of the celebration of the students (Class 1957 and Class 1960), have not been able to organise many feast of St Apollonia (February 9th) to myself included, were invited. events this year. the outings organised by dentist Mr September 2020 – Issue 75 Anthony Ciappara (is-Sur Nin) for The event seems to have lapsed again On the 18th September 2020 the children from the orphanages. until 1966 when Mass was celebrated DAM arranged a free online at St Franics Church Valletta. International Congress with MOI The first documentary evidence of (Masters of Implantology, Goethe participation by dentaI surgeons I remember that the side altar of Sts University) for its paid-up members is from the Times of Malta which Cosmos and Damian was used and who wished to attend. stated that on Saturday February 7th a painting of St Apollonia put up. 1948 a number of dental surgeons In January 1975 I, as Dean of Dental The front cover is by the accomplished and dentists attended Mass in the Surgery, received a letter from Mr 3 artist Jacqui Agius, entitled ‘Aerial Hamrun Parish Church followed by Ciappara deploring that the custom View of Mdina’ from a photo taken lunch at the Riviera Hotel, Ghajn had been discontinued (Fig 5). -

Tooth Surface Loss (TSL)
Tooth Surface Loss (TSL) Sumamry This lesson is intended to give an overview of what to consider when treating patients with TSL, including the causes and management. Tooth surface loss can be physiological or pathological. These are distinguished by taking into account the patient’s age and the severity of tooth wear e.g. in a young person with severe TSL would be pathological, whereas in an older person with moderate TSL this may be physiological from normal use over the years. Buzz words: Erosion Abrasion Attrition Abfraction Tooth Wear Index (TWI) Basic Erosive Wear Examination (BEWE) Occlusal Vertical Dimension (OVD) Centric Occlusion (CO) Retruded contact position (RCP) Intercuspal position (ICP) Dahl Effect Diagnostic wax up Mock upsReviseDental.com Conformative Reorganised Splints (Michigan and Tanner, soft and bilaminar) Epidemiology (1) 77% of the adult population have tooth wear of some degree. (2) 15% of dentate adults exhibited moderate tooth wear (exposing substantial dentine) 2% of adults suffered from severe tooth wear (exposing secondary dentine or pulp) More prevalent in men (70%) than women (61%) Causes: There are 4 causes of tooth surface loss: 1. Erosion 2. Abrasion (Think abrasion= brushing aka an object other than an opposing tooth) 3. Attrition (Think attrition = teeth) 4. Abfraction Tooth surface loss is often a multifactorial problem. The different causes often appear simultaneously which potentiate their effects. It is important to identify the etiological factors of tooth wear so that the patient can be advised of ways to manage it. ReviseDental.com Erosion (3) Erosion is the loss of tooth substance by chemical action, not involving bacteria.