Community Profile Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Community Action of Skagit County 330 Pacific Place, Mount Vernon, WA 98273 Phone: (360) 416-7585 Email: [email protected]
Contact Information Community Action of Skagit County 330 Pacific Place, Mount Vernon, WA 98273 Phone: (360) 416-7585 Email: [email protected] Online Resource Directory www.skagitcrc.org A searchable online database that contains copies of this Revised 09/15/2016 booklet in English and Spanish as well as much more re- source information. Large Format Guides (8.5” x 11”)–available upon request. A quick guide to community services published by Community Action of Skagit County with the help of dozens of Donations organizations in Skagit County. To make a contribution towards helping us publish this guide visit www.communityactionskagit.org or call (360) 416-7585. Online version at www.skagitcrc.org 9/27/2016 For more information and resources call North Sound 2-1-1. Contact Information Community Action of Skagit County 330 Pacific Place, Mount Vernon, WA 98273 Phone: (360) 416-7585 Email: [email protected] Online Resource Directory www.skagitcrc.org A searchable online database that contains copies of this Revised 09/15/2016 booklet in English and Spanish as well as much more re- source information. Large Format Guides (8.5” x 11”)–available upon request. A quick guide to community services published by Community Action of Skagit County with the help of dozens of Donations organizations in Skagit County. To make a contribution towards helping us publish this guide visit www.communityactionskagit.org or call (360) 416-7585. Online version at www.skagitcrc.org 9/27/2016 For more information and resources call North Sound 2-1-1. Table of Contents SUBJECT Listing (alphabetical) Page Alcohol & Drug Services ...................................................................... -

Skagit Valley Food Co-Op Northwest Local Products Instore
SKAGIT VALLEY FOOD CO-OP NORTHWEST LOCAL PRODUCTS INSTORE How we define local: A product that is made or grown within a 250 miles radius or within a 4- hour drive of the Co-op. This means that apples grown in Chelan, Tomatoes grown in British Columbia, and Chocolate made in Portland are all considered "Northwest Local". Most wine grapes are grown east of the mountains, just beyond our "250 mile" definition, but are included in this list as an exception. UPDATED OCT 24, 2014 BRAND DESCRIPTION DEPARTMENT LOCATION BEER & BEERWINE BEER AMNESIA BREWING MICROBREWS BEER WASHOUGAL, WA 10 BARREL BREWING MICROBREWS BEER PORTLAND, OR BOUNDARY BAY BREWING CO MICROBREWS BEER BELLINGHAM, WA BRIDGEPORT BREWING MICROBREWS BEER PORTLAND, OR CHUCKANUT BREWERY MICROBREWS BEER BELLINGHAM, WA DESCHUTES BREWING MICROBREWS BEER PORTLAND/BEND, OR ELYSIAN BREWING MICROBREWS BEER SEATTLE, WA FISHTALE BREWING MICROBREWS BEER OLYMPIA, WA FORT GEORGE BREWING MICROBREWS BEER ASTORIA, OR FREMONT BREWING MICROBREWS BEER SEATTLE, WA GIGANTIC BREWING MICROBREWS BEER PORTLAND, OR HALE'S ALES MICROBREWS BEER SEATTLE, WA HARVESTER BREWING MICROBREWS BEER PORTLAND, OR HOPWORKS BREWING MICROBREWS BEER PORTLAND, OR LAURELWOOD BREWING MICROBREWS BEER PORTLAND, OR ODIN BREWING MICROBREWS BEER SEATTLE, WA PIKE BREWING MICROBREWS BEER SEATTLE, WA PYRAMID BREWING MICROBREWS BEER SEATTLE, WA ROGUE BREWING MICROBREWS BEER PORTLAND, OR SCUTTLEBUTT BREWING MICROBREWS BEER EVERETT, WA SKAGIT RIVER BREWING MICROBREWS BEER MOUNT VERNON SQUARE MILE BREWING CIDER BEER PORTLAND, OR TIETON -

Cultural Resources Assessment for the Mount Vernon Downtown Flood Protection Project Mount Vernon, Skagit County, Washington
CULTURAL RESOURCES ASSESSMENT FOR THE MOUNT VERNON DOWNTOWN FLOOD PROTECTION PROJECT MOUNT VERNON, SKAGIT COUNTY, WASHINGTON BY MARGARET BERGER AND SUSAN MEDVILLE GLENN D. HARTMANN, PRINCIPAL INVESTIGATOR PREPARED FOR: PACIFIC INTERNATIONAL ENGINEERING PO BOX 1599 EDMONDS, WA 98020 TECHNICAL REPORT #342 CRC PROJECT #0711I CULTURAL RESOURCE CONSULTANTS, INC. 8001 DAY ROAD WEST, SUITE B BAINBRIDGE ISLAND, WA 98110 FEBRUARY 28, 2008 Executive Summary This report describes a cultural resources assessment for the Mount Vernon Downtown Flood Protection Project, in Mount Vernon, Skagit County, Washington. This assessment was conducted at the request of the City of Mount Vernon. This report is intended to serve as a component of preconstruction environmental review in accordance with Section 106 of the National Historic Preservation Act (NHPA), as amended. The project consists of modifications to the existing flood protection system. Project plans include raising the existing earthen levee, installing new levee and floodwall segments in some locations, and a new ring dike around the Mount Vernon Wastewater Treatment Plant. To accommodate levee improvements, seven downtown commercial buildings and a residence will be razed. Assessment methods included a review of relevant background literature and maps, archaeological field reconnaissance survey and testing, and a historic building survey. There are no archaeological sites recorded within the project. Archaeological testing conducted using a backhoe revealed thick alluvial deposits overlain, in places, by fill. No indications of buried archaeological sites were observed, and the project is considered to have a low potential to affect as-yet unknown cultural resources. No further archaeological investigations are recommended prior to commencement of the project. -

Skagit County Agriculture Statistics 2015
Photo by Adam Sanchez Photo by Chris Benedict PhotoPhoto by Don by Derek McMoran Gustafson WSU Skagit County Extension Skagit County Agriculture Statistics 2015 Greetings! Washington State University Skagit County Extension has been keeping crop records since 1922. Information is compiled from processing companies, farm organizations, growers, field representatives, media sources, and University sources. Agricultural statistics with related written details are important for several reasons: Figures show the past production history of farming in a community; Statistics show the ups and downs of agriculture in relationship to weather, economics, urban encroachment, disasters, or a shift in production to other areas; Figures give a basis on which to make important decisions for land -use planning, zoning, and economic development planning related to agriculture. Your comments and suggestions are welcomed and encouraged. Feel free to give us a call if we can help you better understand the enclosed information. Washington State University Extension engages people, organizations and communities to advance economic well- being and quality of life by connecting them to the Don McMoran knowledge base of the university and by fostering inquiry, learning, and the application of research. Don McMoran Agriculture and Natural Resources Extension Faculty Skagit County Director WSU Skagit County Extension [email protected] 2 WSU SKAGIT COUNTY EXTENSION STAFF Don McMoran Talea Price Agriculture and Natural Resources Faculty Entomology Coordinator and -
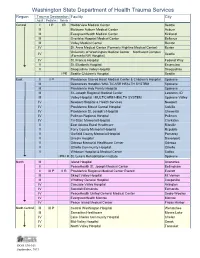
Trauma Designated
Washington State Department of Health Trauma Services Region Trauma Designation Facility City Adult Pediatric Rehab Central I I P IR Harborview Medical Center Seattle III Multicare Auburn Medical Center Auburn III EvergreenHealth Medical Center Kirkland III Overlake Hospital Medical Center Bellevue III Valley Medical Center Renton IV St. Anne Medical Center (Formerly Highline Medical Center) Burien University of Washington Medical Center – Northwest Campus IV Seattle (Formerly NW Hospital) IV St. Francis Hospital Federal Way V St. Elizabeth Hospital Enumclaw V Snoqualmie Valley Hospital Snoqualmie I PR Seattle Children’s Hospital Seattle East II II P Providence Sacred Heart Medical Center & Children’s Hospital Spokane III Deaconess Hospital / MULTICARE HEALTH SYSTEM Spokane III Providence Holy Family Hospital Spokane III St. Joseph Regional Medical Center Lewiston, ID III Valley Hospital / MULTICARE HEALTH SYSTEM Spokane Valley IV Newport Hospital & Health Services Newport IV Providence Mount Carmel Hospital Colville IV Providence St. Joseph’s Hospital Chewelah IV Pullman Regional Hospital Pullman IV Tri-State Memorial Hospital Clarkston V East Adams Rural Healthcare Ritzville V Ferry County Memorial Hospital Republic V Garfield County Memorial Hospital Pomeroy V Lincoln Hospital Davenport V Odessa Memorial Healthcare Center Odessa V Othello Community Hospital Othello V Whitman Hospital & Medical Center Colfax I PR-I R St. Luke’s Rehabilitation Institute Spokane North III Island Hospital Anacortes II PeaceHealth St. Joseph Medical Center -

Washington State's Scenic Byways & Road Trips
waShington State’S Scenic BywayS & Road tRipS inSide: Road Maps & Scenic drives planning tips points of interest 2 taBLe of contentS waShington State’S Scenic BywayS & Road tRipS introduction 3 Washington State’s Scenic Byways & Road Trips guide has been made possible State Map overview of Scenic Byways 4 through funding from the Federal Highway Administration’s National Scenic Byways Program, Washington State Department of Transportation and aLL aMeRican RoadS Washington State Tourism. waShington State depaRtMent of coMMeRce Chinook Pass Scenic Byway 9 director, Rogers Weed International Selkirk Loop 15 waShington State touRiSM executive director, Marsha Massey nationaL Scenic BywayS Marketing Manager, Betsy Gabel product development Manager, Michelle Campbell Coulee Corridor 21 waShington State depaRtMent of tRanSpoRtation Mountains to Sound Greenway 25 Secretary of transportation, Paula Hammond director, highways and Local programs, Kathleen Davis Stevens Pass Greenway 29 Scenic Byways coordinator, Ed Spilker Strait of Juan de Fuca - Highway 112 33 Byway leaders and an interagency advisory group with representatives from the White Pass Scenic Byway 37 Washington State Department of Transportation, Washington State Department of Agriculture, Washington State Department of Fish & Wildlife, Washington State Tourism, Washington State Parks and Recreation Commission and State Scenic BywayS Audubon Washington were also instrumental in the creation of this guide. Cape Flattery Tribal Scenic Byway 40 puBLiShing SeRviceS pRovided By deStination -

The 2019 Skagit Valley Tulip Festival Our Thirty-Sixth Anniversary Elcome to the Wonder of the Skagit Valley Tulip Festival
Welcome to the 2019 Skagit Valley Tulip Festival Our Thirty-Sixth Anniversary elcome to the wonder of the Skagit Valley Tulip Festival. Our for everyone. This brochure is your guide everything from field locations, festival celebrates the beauty of fields filled with blooming where to stay and daily events. Whether you live locally or are traveling Wtulips of all colors and varieties. The growers at RoozenGaarde from afar, Skagit Valley Washington is ready for your and Tulip Town offer display gardens worthy of that special photo and discovery. Don’t forget your boots! those unique souvenirs to commemorate your visit. Throughout the month of April, there are many events to enjoy. From the Street Fair or the Lisa Knowles LaConner Parade to a scenic drive through the valley, there is something President, Skagit Valley Tulip Festival Board of Directors Tips on Touring the Festival WHEN to COME? In April! – Least crowded times: Weekdays! Weekends www.tulips.com/bloommap, call us at (360) 428-5959, go to www.tulipfes- are very busy; arrive before 10 am to beat the crowds. The festival is a tival.org, visit www.Facebook.com/SkagitValleyTulipFestival. Tulip crops driving tour, with events MILES apart. Our brochure map is not to scale. rotate, so you WILL need a new map each year. PARKING – Park FREE at the two gardens, RoozenGaarde and Tulip Town. TULIPS – There will be tulips for you to see ALL of April. Tulip Town parking is on Bradshaw Road. RoozenGaarde on Beaver Marsh PLEASE NOTE: Drones are not allowed in the gardens or the fields. -

Where Can I Sell My Products and How Do I Get Them to Market?
Where can I sell my products and how do I get them to market? There are many resources in Pierce County that will help you get your products to market, whether you are selling at a Farmer’s Markets, directly to consumers, or through a distributor. This fact sheet includes purchasers, distributors, and aggregators. To visit a webpage, click on the title or copy and paste the link into your browser. Charlie’s Produce Charlie's Produce supplies restaurants, grocery stores, institutions, wholesalers and the marine industry with a full range of conventional, organic and specialty agricultural products. http://www.charliesproduce.com Duck Delivery of Washington, Inc. Duck Delivery of Washington, Inc. supplies customers and restaurants with quality fresh fruits, vegetables, and custom-cut produce. http://www.duckdelivery.com/ FoodHub FoodHub gathers food producers, professional food buyers, and the associations and suppliers that serve them both, in one dynamic marketplace and interactive directory. FoodHub engages the entire food community, including retail grocers, schools, institutional buyers, caterers, restaurants, farmers, ranchers, fishermen, vintners, plus the associations, service providers and industry suppliers that serve them all. http://food-hub.org/ Fresh Food Revolution Fresh Food Revolution is a non-profit cooperative of farmers, ranchers, food producers and the consumers who love to buy local. Their goal is to increase the amount of food purchased and eaten locally by providing an avenue for farmers to connect with consumers, restaurants, and institutions through local online markets. http://www.localfoodmarketplace.com/freshfoodrevolution/ Full Circle Full Circle is an artisan grocer and organic produce delivery service in Washington, Oregon, California, Alaska and Idaho. -

Mapping of Major Latest Pleistocene to Holocene Eruptive Episodes from the Glacier Peak Volcano, Washington—A Record of Lahar
MAPPING OF MAJOR LATEST PLEISTOCENE TO HOLOCENE ERUPTIVE EPISODES FROM THE GLACIER PEAK VOLCANO, WASHINGTON—A RECORD OF LAHARIC INUNDATION OF THE PUGET LOWLANDS FROM DARRINGTON TO THE PUGET SOUND 123° 122° 121° 49° Benjamin W. Stanton and Joe D. Dragovich, Washington Department of Natural Resouces, Division of Geology and Earth Resources, 1111 Washington St SE, Olympia, WA 98504-7007, [email protected] and [email protected] map area Bellingham SAN WHA TCOM 20 JUAN Volcanic hazards in the Pacific Northwest are typically associated with more visible stratovolcanoes, such as Mount Rainier. Glacier Peak, a North Cascade dacitic stratovolcano near Darrington, Washington, has produced at least three large eruptive episodes See Figure 2 14 path of lahars since the culmination of the last continental glaciation with each episode likely lasting a few hundred years. Data from recent detailed geologic mapping, new C ages, stratigraphic relations, clast petrographic analyses, geochemical analyses, and laharic SKAGIT to lower Skagit Valley ISLAND sand composition indicate that three large eruptive episodes occurred in the latest Pleistocene and Holocene—the information refines and expands on the pioneering work of Beget (1981). These voluminous events traveled up to 135 km downvalley of the path of lahars to lower Stillaguamish Valley Glacier Peak edifice and reached the Puget Sound via the ancient Skagit and Stillaguamish deltas. Glacier Peak has erupted dacite of similar composition throughout its history. Hypersthene-hornblende-(augite)-phyric vesicular lahar clasts found from Glacier Peak to La volcano 48° SNOHMISH Conner, Washington have similar geochemistry to dacite flows sampled on the volcano. Radiocarbon dating of the White Chuck assemblage shows an eruptive episode of ~11,900 yrs B.P. -

1. Skagit Basin Overview
1. Skagit Basin Overview Abstract Since the 1850s, the Skagit River basin has been altered by human activities such as logging, diking, and the construction of dams, roads, levees, and tide gates. Logging and construction of levees and dikes converted coniferous forest and wetlands to farmland, industrial, and urban/suburban residential development. Dams constructed in the Skagit River not only generate hydropower but also provide flood control, recreation opportunities, and diverse ecosystem services. Major highways constructed through Skagit County promoted both economic and population growth in Skagit County. These human developments have dramatically impacted the hydrology and geomorphology of the basin and have impacted or reduced habitat for a wide range of species, including multiple species of native anadromous fish historically reliant on Skagit River Basin tributaries. Low-lying farms, urban development, and other lands in the floodplain are currently vulnerable to river flooding and sea level rise. The economy of the Skagit River basin in the 19th and early 20th centuries was focused primarily on logging, mining, and agriculture, but has diversified through the second half of the 20th century. Rapid increases in population in the 21st century are projected for Skagit Co., which, under the Growth Management Act and the Skagit County Comprehensive Plan, will direct future growth primarily in urban areas. 1.1 Overview of the Skagit River Basin The Skagit River basin is located in southwestern British Columbia in Canada and northwestern Washington in the United States (Figure 1.1) and drains an area of 3,115 square miles (Pacific International Engineering, 2008). Major tributaries in the basin are the Baker River, Cascade River, and Sauk River. -
Resource Guide
Skagit County Public Health Developmental Disabilities Program Resource Guide To request additional copies, please contact: Skagit County Public Health Developmental Disabilities Program 700 South 2nd Street, #301 Mount Vernon, WA 98273 (360) 416-1500 www.skagitcounty.net/Departments/PHCS For additions or corrections, please send comments to: [email protected] Inclusion in this directory does not constitute endorsement, nor is any omission an intention. Updated January 2017 2 Welcome! Navigating through heaps of resources can feel overwhelming at times. We hope this guide can help you find what you’re looking for. This guide has information about public, private and non-profit agencies for individuals with developmental disabilities. Because we could not fit every resource into one guide, we would like to refer you to another community resource for basic needs such as food and shelter, as well as drug and alcohol treatment, counseling, and volunteerism. Community Action of Skagit County is a community-based organization that provides services and advocates for the needs of those experiencing poverty. Community Action has 39 anti-poverty programs, including the Critical Needs program, Energy Assistance Program, Women, Infants & Children Program (WIC), and the Veteran’s Assistance Program. Please contact Community Action of Skagit County for more information about these programs or other resources not found in this guide. Community Action of Skagit County 330 Pacific Place, Mount Vernon (360) 416-7585 or visit www.communityactionskagit.org Community Information Line: Telephone information regarding resources and services including rental assistance, counseling, support groups, food, clothing, donations, volunteering, transportation, emergency shelter and more. Call 2-1-1. -

Olympic Consortium Washington State - Workforce Development Area 1
Olympic Consortium Washington State - Workforce Development Area 1 INTEGRATED WORKFORCE PLAN Program Years 2020 to 2024 pg. 1/68 This page is intentionally left blank. pg. 2/68 EXECUTIVE SUMMARY Foreword- The growing impact of the COVID-19 pandemic is changing the workforce development landscape in the United States, the State of Washington, and Clallam, Jefferson and Kitsap Counties. As this plan was completed, the County leadership recognized the need for a swift reaction to this economic emergency and the need for long-term recovery efforts. These issues will be addressed in the coming weeks as staff work with Elected leadership in the three Counties to develop strategies for successful navigation of this crisis.1 See Goal One in required Section III. The Olympic Workforce Development Council (OWDC)- The OWDC serves Clallam, Jefferson, and Kitsap Counties and is an expert in support of the region's workforce development efforts. The Olympic Consortium Board, comprised of County Commissioners from the three Counties, and the OWDC, comprised of business, labor representatives, and public sector leaders, are dedicated to the development of a workforce system that supports employers and jobseekers. The OWDC serves as a hub for gathering and disseminating information about the area's labor market and business employment needs. The OWDC includes members representing business, education, state agencies, and nonprofits with a focus on finding innovative solutions for workforce challenges. These efforts include working closely with the K-12 system and especially the Career and Technical Education Directors across the three-County area. OWDC staff work closely with colleges, business, and nonprofits via Business Services programs to assist in meeting the needs of jobseekers and employers alike.