ROGAINE® FOAM 5% Minoxidil Foam 5
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

5 Written Questions
4/21/2020 Test: MILADY CHAPTER 11 | Quizlet NAME 5 Written questions 1. abnormal hair loss. 2. hair flowing in the same direction, resulting from follicles sloping in the same direction. 3. an amino acid that joins together two peptide strands. 4. provides natural dark brown to black to the hair and is the dark pigment predominant in black and brunette hair. https://quizlet.com/302174566/test 1/5 4/21/2020 Test: MILADY CHAPTER 11 | Quizlet 5. the number of individual hair strands on 1 square inch (2.5 square centimeters) of scalp 5 Matching questions A. (lanugo hair) short, fine, unpigmented downy hair that 1. amino acids appears on the body, with the exception of the palms of the hands and the soles of the feet. 2. vellus hair 3. peptide bond 4. dermal papilla 5. hypertrichosis B. (end bond) chemical bond that joins amino acids to each other, end to end, to form a polypeptide chain. C. (hirsuties) condition of abnormal growth of hair, characterized by the growth of terminal hair in areas of the body that normally grow only vellus hair. D. units that are joined together end to end like pop beads by strong, chemical peptide bonds to form the polypeptide chains that comprise proteins. https://quizlet.com/302174566/test 2/5 4/21/2020 Test: MILADY CHAPTER 11 | Quizlet E. plural: dermal papilla. A small, cone-shaped elevation location located at the base of the root follicle that fits into the hair bulb. 5 Multiple choice questions 1. the bonds created when disulfide bonds are broken by hydroxide chemical hair relaxers after the relaxer is rinsed from the hair. -

Topically Applied Minoxidil in Baldness
Review Topically Applied Minoxidil in Baldness ERVIN NOVAK,M.D., THOMASJ. FRANZ, M.D., JOHN T. HEADINGTON,M.D., AND RONALD C. WESTER,PH.D. From the Upjohn Company, Kalamazoo, Michigan, School idil and its metabolites can be removed by hemodi- of Medicine, University of Washington, Seattle, alysis. Washington, Medical School, University of Michigan, Ann Fluid retention and hypertrichosis are the most Arbor, Michigan, and School of Medicine and School of Pharmacy, University of California, San Francisco, California commonly occurring side effects of minoxidil. Hair regrowth in a patient with male pattern baldness was described in a case report of a hypertensive patient treated twice daily with 20 mg oral minoxidil.6 The Minoxidil, an orally administered, peripheral va- extensive hair regrowth continued after 10 months sodilator used to treat hypertension, causes hypertri- of therapy. New and increased hair growth as a side chosis in more than 80% of users. The drug reduces effect was also detected in an early clinical study elevated blood pressure by decreasing peripheral involving five of eight patients on oral minoxidil vascular resistance. Chemically, minoxidil is 2,4-di- therapy for 2 month^.^ Zappacosta' reported reversal amino-6-piperidinopyrimidine-3-oxide; it is soluble in of baldness in a patient on minoxidil for the treatment water to the extent of approximately 2 mg/ml, is of hypertension. more readily soluble in propylene glycol or ethanol, After the third week of therapy with oral minoxidil, and is nearly insoluble in acetone, chloroform, or hypertrichosis usually appears between the eyebrows ethyl acetate. Following oral administration of minox- and the hair line, in the malar and temporal areas, idil and in association with the reduction in peripheral on the backs of the arms, on the shoulders, and on vascular resistance, cardiac output is augmented, salt the legs. -

ARTICLE 17A Barbers and Cosmetologists | Chapter 61 - Professional A
ARTICLE 17A Barbers and Cosmetologists | Chapter 61 - Professional a... https://nmonesource.com/nmos/nmsa/en/item/4397/index.do?iframe=tr... ARTICLE 17A Barbers and Cosmetologists 61-17A-1. Short title. (Repealed effective July 1, 2026.) Chapter 61, Article 17A NMSA 1978 may be cited as the "Barbers and Cosmetologists Act". History: Laws 1993, ch. 171, § 1; 2013, ch. 166, § 3. ANNOTATIONS The 2013 amendment, effective June 14, 2013, added the NMSA chapter and article for the Barbers and Cosmetologists Act; and at the beginning of the sentence, deleted "Sections 1 through 24 of this act" and added "Chapter 61, Article 13 NMSA 1978". Law reviews. — For article, "Constitutional Limitations on the Exercise of Judicial Functions by Administrative Agencies," see 7 Nat. Res. J. 599 (1972). Am. Jur. 2d, A.L.R. and C.J.S. references. — 11 Am. Jur. 2d Barbers and Cosmetologists §§ 4 to 12. Places or persons within purview of statute or ordinance as to licensing of barbers, 31 A.L.R. 433, 59 A.L.R. 543. Validity, construction, and effect of statute or ordinance regulating beauty culture schools, 56 A.L.R.2d 879. 39A C.J.S. Health and Environment §§ 37 to 39. 61-17A-2. Definitions. (Repealed effective July 1, 2026.) As used in the Barbers and Cosmetologists Act: A. "barber" means a person, other than a student, who for compensation engages in barbering; B. "board" means the board of barbers and cosmetologists; C. "cosmetologist" means a person, other than a student, who for compensation engages in cosmetology; D. "electrologist" means a person, other than a student, who for compensation removes hair from or destroys hair on the human body through the use of an electric current applied to the body with a needle-shaped electrode or probe; 1 of 25 7/15/2021, 11:23 AM ARTICLE 17A Barbers and Cosmetologists | Chapter 61 - Professional a.. -

Is This Hair Professional Enough?
HUMANITIES | ENCOUNTERS Is this hair professional enough? n Cite as: CMAJ 2021 February 16;193:E254-5. doi: 10.1503/cmaj.201871 was eight years old when my mother sent me to school with Bantu knots in my hair. This hairstyle, which origi- Inated with the Zulu people of southern Africa, was worn for centuries on the Afri- can continent before becoming widely adopted by the diaspora. I returned home that afternoon in tears. My classmates, unaccustomed to a hairstyle of that sort, had spent all day laughing, pointing and comparing my hair to excrement. The tiny shred of pride I had had in my natural kinky-textured hair was crushed. I told my mother never to style it like that again and begged her for a chemical hair relaxer; she finally caved in about two years later. I spent the ensuing years, into early adulthood, chemically straightening my hair and adopting a variety of protective styles: braids, cornrows, hair extensions and wigs. Women of African descent com- monly use these styles to protect our hair from overmanipulation and to permit undisrupted growth of the hair. Unfortunately, these styles, along with the use of chemical relaxers for perma- nent hair straightening, have been strongly linked to a form of hair loss known as traction alopecia. One study found that a third of Black women suffer from this condition, which can lead to Image copyright iStock.com/GeorgePeters. No standalone file use permitted. permanent hair loss if not detected and treated early.1 In addition, Black women women in my environment, I subscribed The end of my undergraduate degree who use relaxers have been shown to to that belief and happily shelled out hun- and the beginning of my journey in medi- have a higher likelihood of developing dreds of dollars in pursuit of these looks. -
Label-Free Cell Phenotypic Profiling Decodes the Composition And
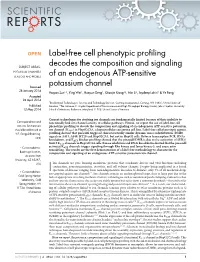
OPEN Label-free cell phenotypic profiling SUBJECT AREAS: decodes the composition and signaling POTASSIUM CHANNELS SENSORS AND PROBES of an endogenous ATP-sensitive Received potassium channel 28 January 2014 Haiyan Sun1*, Ying Wei1, Huayun Deng1, Qiaojie Xiong2{, Min Li2, Joydeep Lahiri1 & Ye Fang1 Accepted 24 April 2014 1Biochemical Technologies, Science and Technology Division, Corning Incorporated, Corning, NY 14831, United States of Published America, 2The Solomon H. Snyder Department of Neuroscience and High Throughput Biology Center, Johns Hopkins University 12 May 2014 School of Medicine, Baltimore, Maryland 21205, United States of America. Current technologies for studying ion channels are fundamentally limited because of their inability to Correspondence and functionally link ion channel activity to cellular pathways. Herein, we report the use of label-free cell requests for materials phenotypic profiling to decode the composition and signaling of an endogenous ATP-sensitive potassium should be addressed to ion channel (KATP) in HepG2C3A, a hepatocellular carcinoma cell line. Label-free cell phenotypic agonist Y.F. (fangy2@corning. profiling showed that pinacidil triggered characteristically similar dynamic mass redistribution (DMR) com) signals in A431, A549, HT29 and HepG2C3A, but not in HepG2 cells. Reverse transcriptase PCR, RNAi knockdown, and KATP blocker profiling showed that the pinacidil DMR is due to the activation of SUR2/ Kir6.2 KATP channels in HepG2C3A cells. Kinase inhibition and RNAi knockdown showed that the pinacidil * Current address: activated KATP channels trigger signaling through Rho kinase and Janus kinase-3, and cause actin remodeling. The results are the first demonstration of a label-free methodology to characterize the Biodesign Institute, composition and signaling of an endogenous ATP-sensitive potassium ion channel. -

Acquired Hypertrichosis of the Periorbital Area and Malar Cheek
PHOTO CHALLENGE Acquired Hypertrichosis of the Periorbital Area and Malar Cheek Caitlin G. Purvis, BS; Justin P. Bandino, MD; Dirk M. Elston, MD An otherwise healthy woman in her late 50s with Fitzpatrick skin type II presented to the derma- tology department for a scheduled cosmetic botulinum toxin injection. Her medical history was notable only for periodic nonsurgical cosmetic procedures including botulinum toxin and dermal fillers, and she was not taking any daily systemic medications. Duringcopy the preoperative assess- ment, subtle bilateral and symmetric hypertricho- sis with darker terminal hair formation was noted on the periorbital skin and zygomatic cheek. Uponnot inquiry, the patient admitted to purchas- ing a “special eye drop” from Mexico and using it regularly. After instillation of 2 to 3 drops per eye, she would laterally wipe the resulting excess Dodrops away from the eyes with her hands and then wash her hands. She denied a change in eye color from their natural brown but did report using blue color contact lenses. She denied an increase in hair growth elsewhere including the upper lip, chin, upper chest, forearms, and hands. She denied deepening of her voice, CUTIS acne, or hair thinning. WHAT’S THE DIAGNOSIS? a. acetazolamide-induced hypertrichosis b. betamethasone-induced hypertrichosis c. bimatoprost-induced hypertrichosis d. cyclosporine-induced hypertrichosis e. timolol-induced hypertrichosis PLEASE TURN TO PAGE E21 FOR THE DIAGNOSIS From the Department of Dermatology, Medical University of South Carolina, Charleston. The authors report no conflict of interest. Correspondence: Justin P. Bandino, MD, 171 Ashley Ave, MSC 908, Charleston, SC 29425 ([email protected]). -

Guideline for Preoperative Medication Management
Guideline: Preoperative Medication Management Guideline for Preoperative Medication Management Purpose of Guideline: To provide guidance to physicians, advanced practice providers (APPs), pharmacists, and nurses regarding medication management in the preoperative setting. Background: Appropriate perioperative medication management is essential to ensure positive surgical outcomes and prevent medication misadventures.1 Results from a prospective analysis of 1,025 patients admitted to a general surgical unit concluded that patients on at least one medication for a chronic disease are 2.7 times more likely to experience surgical complications compared with those not taking any medications. As the aging population requires more medication use and the availability of various nonprescription medications continues to increase, so does the risk of polypharmacy and the need for perioperative medication guidance.2 There are no well-designed trials to support evidence-based recommendations for perioperative medication management; however, general principles and best practice approaches are available. General considerations for perioperative medication management include a thorough medication history, understanding of the medication pharmacokinetics and potential for withdrawal symptoms, understanding the risks associated with the surgical procedure and the risks of medication discontinuation based on the intended indication. Clinical judgement must be exercised, especially if medication pharmacokinetics are not predictable or there are significant risks associated with inappropriate medication withdrawal (eg, tolerance) or continuation (eg, postsurgical infection).2 Clinical Assessment: Prior to instructing the patient on preoperative medication management, completion of a thorough medication history is recommended – including all information on prescription medications, over-the-counter medications, “as needed” medications, vitamins, supplements, and herbal medications. Allergies should also be verified and documented. -

March Newsletter 2020C Layout 1
March 2020 INSIDER TIPS FOR A HAPPY, HEALTHY AND GLAMOROUS LIFE Natural Good Looks and Healthy Legs: Our Specialty! From The to Key West at the end of March to help my Desk of friend Richard open his practice there. He had Who We Are. What We Do. some setbacks with his father’s hip fracture and Where To Find Us. Dr. D his girlfriend’s father’s demise. I am very interested in his success as I may want to take New York Skin and Vein Center over his practice in KW in my old age. LOL. Next was founded in 2001 by Dr. trip after that is Staunton VA for Dohner, who is the area’s only American Shakespeare Theater for board-certified varicose vein a long weekend beginning of April. specialist (ABVLM). Originally Whoever said Tennis is not a contact called Oneonta Laser Derm, sport is WRONG. I’ve had two ‘incidents’ the practice expanded and changed the recently that were more than a name to New York Skin and Vein Center. So glad that spring is coming! Winter was way sprain! The first was from a fall trying to avoid a We now have 4 locations with 3 dermat- too long even if it was milder than usual. I’m lightning fastball heading towards my face ology PA’s/NP’s, 5 laser nurses and technicians, feeling it more and more as time goes on, thus resulting in a fall on my elbow and it hurt! The with two private surgical facilities for your the trips away in the winter. -

Ambetter 90-Day-Maintenance Drug List- 2020
Ambetter 90-Day-Maintenance Drug List Guide to this list: What is Ambetter 90‐Day‐Maintenance Drug List? Ambetter 90‐Day‐Supply Maintenance Drug List is a list of maintenance medications that are available for 90 day supply through mail order or through our Extended Day Supply Network. How do I find a pharmacy that is participating in Extended Day Supply Network? To find a retail pharmacy that is participating in our Extended Day Supply Network please consult information available under Pharmacy Resources tab on our webpage. Alternatively, you can utilize our mail order pharmacy. Information on mail order pharmacy is available in Pharmacy Resources tab on our webpage. Are all formulary drugs covered for 90 day supply? No, certain specialty and non‐specialty drugs are excluded from 90 day supply. Please consult 90‐Day‐ Supply Maintenance Drug List for information if your drug is included. A Amitriptyline HCl Acamprosate Calcium Amlodipine Besylate Acarbose Amlodipine Besylate-Atorvastatin Calcium Acebutolol HCl Amlodipine Besylate-Benazepril HCl Acetazolamide Amlodipine Besylate-Olmesartan Medoxomil Albuterol Sulfate Amlodipine Besylate-Valsartan Alendronate Sodium Amlodipine-Valsartan-Hydrochlorothiazide Alendronate Sodium-Cholecalciferol Amoxapine Alfuzosin HCl Amphetamine-Dextroamphetamine Aliskiren Fumarate Anagrelide HCl Allopurinol Anastrozole Alogliptin Benzoate Apixaban Alosetron HCl Arformoterol Tartrate Amantadine HCl Aripiprazole Amiloride & Hydrochlorothiazide Armodafinil Amiloride HCl Asenapine Maleate Amiodarone HCl Aspirin-Dipyridamole -
INSIDE THIS ISSUE What’S New a New Tip on Thermage Picturing Your Complexion the Versatile Aurora Big on Botox Calendar of Upcoming Events Summer Specials WHAT’S NEW
THETHE SKINNYSKINNYSUMMER 2004 INSIDE THIS ISSUE What’s New A New Tip On Thermage Picturing Your Complexion The Versatile Aurora Big On Botox Calendar Of Upcoming Events Summer Specials WHAT’S NEW Summer is in full swing, and it’s been a busy first six months at Suzanne for hair removal, especially for those with blond, red, and even white Bruce and Associates. There have been some exciting developments hair. Aurora is also used for our popular FotoFacial™ procedure, and since our winter issue, and I finally have been able to slow down long with its acne head can be an effective light treatment for acne. enough to give you the “skinny” on what’s new in skin rejuvenation. Our Thermage® facial rejuvenation procedure has proven very pop- First, we are pleased to introduce Megan York, our new patient- ular since it was introduced a little over a year ago. The technology and care coordinator. Megan is a licensed aesthetician and has been in the procedure protocol continue to advance. Both are aimed at producing skin-care field for five years. She joined us in March and has been work- ever better results while improving patient comfort during treatment. We ing closely with me, other Suzanne Bruce and Associates professionals, just introduced our new larger surface area fast tip. Learn more about and our product representatives to provide information to our patients this skin tightening treatment below. and assist them in setting up a personal skin-care regimen. Megan is Our new filler, Restylane®, has also been very popular since its also the primary operator of our new VISIA™ Complexion Analysis introduction in January. -

Study Protocol 7
Title: Role of Neurogenic Inflammation and Topical 6% Gabapentin Therapy in Symptomatic Scarring Alopecia Protocol Number: 1308M40801 Study Drug: Gabapentin 6% Solution Principal Investigator: Maria Hordinsky, MD 612-625-8625 Study Team: Rehana Ahmed-Saucedo, MD, PhD Margareth Pierre-Louis, MD Elisabeth Hurliman, MD, PhD Trial Site: University of Minnesota, Department of Dermatology MMC 98 Minneapolis, MN 55455 Laboratory: University of Minnesota, Fairview Laboratory 516 Delaware St. Minneapolis, MN 55455 Masonic Clinical Research Unit MMC 405, 420 Delaware St. Minneapolis, MN 55455 Version Date: January 12, 2016 CONFIDENTIAL This is a University of Minnesota clinical research trial document that contains confidential information. It is intended solely for the recipient clinical investigator(s) and must not be disclosed to any other party. The material may be used only for evaluating or conducting clinical investigations; any other proposed use requires written consent from the University of Minnesota Department of Dermatology. Scarring Alopecia-Gabapentin Study Version 5 | Approved 01.28.2016 Page ii Table of Contents STUDY SUMMARY ................................................................................................................................. 1 1 INTRODUCTION ............................................................................................................................... 2 1.1 BACKGROUND ............................................................................................................................. -

Valproate-Induced Hair Loss: What to Tell Patients
P earls Valproate-induced hair loss: What to tell patients Shailesh Jain, MD, MPH, ABDA, and Beth Beste, MS Teach patients s. B, age 29, has bipolar disorder may lead to low serum and liver tissue bio- that certain that is stabilized by valproate, 1,250 tinidase enzyme4; a major clinical manifes- supplements and Mmg/d. After 1 month of treatment, tation of biotin deficiency is alopecia. she shows scalp hair loss. She takes no other lifestyle changes medications and is distressed because she had 2 Tell patients to avoid taking valproate may reduce this never experienced such copious hair loss. Ms. during meals to prevent its chelating effect on usually temporary B’s blood valproate level is at a therapeutic food. The chelating effect of valproate makes side effect level. She wants to know if the hair loss will metals that facilitate hair growth, such as zinc be permanent and what she can do to stop it. and selenium, unavailable for absorption.5 Up to 28% of patients who take valproate suffer temporary alopecia.1,2 In most cases, 3 Recommend zinc and selenium supple- hair loss is associated with long-term valpro- ments, which can help stop further hair loss ate pharmacotherapy. Hair loss appears to and regenerate hair.5 be dose-related2 and may be more common in women than in men. Usually patients will 4 Suggest practical advice for hair care, in- report gradual but steady hair loss, com- cluding using soft brushes and mild sham- monly beginning 2 to 6 months after initiat- poos and avoiding dyes, heated curlers, and ing treatment.3 Complete hair loss is rare and hair dryers.