Bulletproof Radio, a State of High Performance. Dave Asprey
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Whose Art Is It? - the New Yorker 2/8/16, 11:06 AM
Whose Art Is It? - The New Yorker 2/8/16, 11:06 AM Save paper and follow @newyorker on Twitter In the South Bronx DECEMBER 21, 1992 ISSUE Whose Art Is It? BY JANE KRAMER t could be argued that the South Bronx John Ahearn PHOTOGRAPH BY DUANE bronzes fit right into the neighborhood MICHALS —that whatever a couple of people said about bad role models and negative Iimages and political incorrectness, there was something seemly and humane, and even, in a rueful, complicated way, “correct,” about casting Raymond and his pit bull, Daleesha and her roller skates, and Corey and his boom box and basketball in the metal of Ghiberti, Donatello, and Rodin and putting them up on pedestals, like patron saints of Jerome Avenue. John Ahearn, who made the statues, says that he thought of them more as guardians than as saints, because their job was ambiguous, standing, as they did for a couple of days last year, between the http://www.newyorker.com/magazine/1992/12/21/whose-art-is-it Page 1 of 47 Whose Art Is It? - The New Yorker 2/8/16, 11:06 AM drab new station house of the city’s 44th Police Precinct and what is arguably one of its poorest, saddest, shabbiest, most drug-infested, AIDS-infected, violent neighborhoods. John himself is ambiguous about “ambiguous.” He says that when the city asked him to “decorate” the precinct he thought of the Paseo de la Reforma, in Mexico City, with its bronze heroes—a mile of heroes. He thought that maybe it would be interesting—or at least accurate to life on a calamitous South Bronx street, a street of survivors—to commemorate a few of the people he knew who were having trouble surviving the street, even if they were trouble themselves. -

TSCA Section 402(C)
ENVIRONMENTAL PROTECTION AGENCY Round Table Discussion of: TSCA Section 402(c) Lead Exposure Reduction Proposed Renovation and Remodeling Rule March 8, 1999 DoubleTree Hotel Crystal City Arlington Virginia Reported By: CASET Associates 10201 Lee Highway, Suite 160 Fairfax, Virginia 22030 (703) 352-0091 TABLE OF CONTENTS Page Welcome, Introductions, and Review-to-Date 1 Work Practice Standards (set-up, dust control, 10 clean-up, clearance, restricted practices) Certification and Accreditation 149 Final Questions, Summary and Next Steps 238 PARTICIPANTS VICKI AINSLIE, Georgia Tech Research Institute, Atlanta, GA RICHARD BAKER, Baker Environmental Consulting, Inc, Lenexa, KS ROB BEEKMAN MEGAN BOOTH, National Association of Realtors, Washington, DC DEAN BULLIS, MD Department of the Environment, Baltimore, MD KENNETH CARLINO, New York City Department of Health, NY, NY PATRICK CONNOR, CONNOR, Baltimore, Maryland GENE DANIELS, UBC H&S Fund, Cincinnati, Ohio STEPHEN DIETRICH, POCA, Lancaster, Pennsylvania PIERRE ERVILLE, Consultant, Silver Spring, Maryland NICK FARR, National Center for Lead-Safe Housing, Columbia, MD NEIL FINE, Applied Systems, Inc., Holland, Pennsylvania MARC FREEDMAN, Painting & Decorating Contractors of America, Fairfax, Virginia GREGG GOLDSTEIN, National Multihousing Council, Washington, DC DAVID HARRINGTON, California Department of Health Services Occupational Lead Poisoning Prevention Program, Oakland, CA MARK HENSHALL, US EPA, Washington, DC EILEEN LEE, National Multihousing Council, Washington, DC DAVID LEVITT, HUD, -

UC Riverside UC Riverside Electronic Theses and Dissertations
UC Riverside UC Riverside Electronic Theses and Dissertations Title The Smell of Rain Permalink https://escholarship.org/uc/item/4gx7s18h Author Gibbs, Nicole Ann Publication Date 2015 Peer reviewed|Thesis/dissertation eScholarship.org Powered by the California Digital Library University of California UNIVERSITY OF CALIFORNIA RIVERSIDE The Smell of Rain A Thesis submitted in partial satisfaction of the requirements for the degree of Master of Fine Arts in Creative Writing and Writing for the Performing Arts by Nicole Ann Gibbs December 2015 Thesis Committee: Professor Andrew Winer, Co-Chairperson Professor Rob Roberge, Co-Chairperson Professor Mary Otis Copyright by Nicole Ann Gibbs 2015 The Thesis of Nicole Ann Gibbs is approved: Committee Co-Chairperson Committee Co-Chairperson University of California, Riverside Acknowledgements Very special thanks to Rob Roberge, Mary Otis, Gina Frangello, Elizabeth Crane, Anthony McCann, Emily Rapp, Deanne Stillman, for teaching me everything I know about writing. To Michelle Camacho, Rebecca Gibbs, Gia Burton-Blasingame, Taylor Rubinstein, Jordan Rubinstein, Emily Rubinstein, Carol Gibbs, Greg Rush, Bill Gibbs, Linda Fox, Molly Rubinstein, Cheryl Fort, Sara Gibbs, Aaron Gibbs, Jaysin Graves, Hailey Gibbs, Persephone Gibbs, for giving me the time, space, motivation and encouragement, support and coffee needed to do this. To Stephanie Anne and Jason Metz for sharing your experience. To my chosen family, who loves me and supports me no matter what and to Tod Goldberg and Agam Patel for giving me a chance and for putting up with my craziness. iv This work is dedicated to my father, Bill Gibbs, who always encouraged me to use my imagination and follow my dreams. -

Question & Answers # 10
Question & Answers # 10 Hebrews 11: Bro. Lee Vayle - March 8, 1998 Heavenly Father, it’s so wonderful to hear the songs of Zion and know that we are singing them unto you, that we have a part of You, Yourself, and a part in Your great predestinated plan; so one day it’s going to be God, All in all, when the Son hands over everything to the Father, Who now we know you, Great Jehovah-Elohim, standing here somewhere amongst the Bride, somewhere adjudicating, somewhere blessing, somewhere helping. You are here, Lord, to bring us this Word as You want it to be to a people worshipping you in Spirit and in Truth to bring forth a Resurrection and a Rapture. We know that to be true. What a golden hour in which we live! What a wonderful time. We are rejoicing this morning and have our doubts settled and any fear we might have put aside, because you have not given us a spirit of fear but of love. And You, Yourself, Love, are here giving us courage and a sound mind. May each one realize that, not only have we passed from death unto life, but into that life for which there is a true sanity, which is the mind of God; even as Paul said, “Let this mind be in you which was in Christ.” We know, Father, that is true. We know this is a mind age; we know it is your age. We know we’re a part of it. May we never forget it. -
For Additional Information Contact the Archives Center at 202.633.3270 Or
Funding for the Smithsonian Jazz Oral History Program NEA Jazz Master interview was provided by the National Endowment for the Arts. HANK JONES NEA Jazz Master (1989) Interviewee: Hank Jones (July 31, 1918 – May 16, 2010) Interviewer: Bill Brower Date: November 26-27, 2004 Repository: Archives Center, National Museum of American History Description: Transcript, pp. 134 Hank Jones: I was over there for about two and a half weeks doing a promotional tour. I had done a couple of CDs; one was with my brother Elvin and Richard Davis, the bass player. They made – – I think they made two releases from that date. And I did another date with Jack DeJohnette and John Patitucci. But, these two albums were the objects of the promotion. I mean, they promote very, very heavily everyday. I must have had 40 interviews and about 30 record signings at the record shops, plus all of the recording. We did seven concerts and people inevitably want the records, CDs of the concert for us to sign. I have a trio over there, with Jimmy Cobb and John Fink. It was called, “The Great Jazz Trio.” It was not my name, but the Japanese have special names for everything, you know? That's only one in a series of tree others which he called the great jazz trio. The first one was Ron Carter, Tony Williams and myself. But, there had been a succession of different changes in personnel. It changed about six times. The current one was Jimmy Cobb and Dave Fink--Oh, the cookies have arrived and not a minute too soon. -
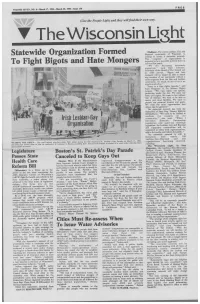
View Full Issue As
VOLUME SEVEN, NO. 6—March 17, 1994—March 30, 1994—Issue 150 FREE Give the People Light and they will find their own way. IV The Wisconsin Light Statewide Organization Formed [Madison]- The entire Lesbian, Gay and Bisexual community of Wisconsin is uniting to create a statewide network. This "congress" of organizations is To Fight Bigots and Hate Mongers expected to be a powerful political force in the next few years. "We are becoming extremely organized," said Dale Johnson, President of the Board of The United and an AIDS activist. "Bigots and hate mongers will no longer be able to attack any member of our community without a swift response from the Gay and Lesbian community. An attack on one of us is an attack on all of us." There is a Gay rights agenda," said Karl Hoagland of the Human Rights League. "We want equal, not special, protection under the law. We want our basic civil rights. We want to live without fear of violence. We want to be able to marry and raise families. We want to pursue our personal dreams and goals. We want the same opportunities that others take for granted." The statewide network has been the brainchild of State Rep. Tammy Baldwin (D-Madison). "We need to be unified to confront the assaults on our community," she said. "When I introduce Domestic Partnership legislation and same-sex marriage legislation, the Lesbian, Gay and Bisexual and supportive communities will be organized to lobby their representatives, talk to the media, and inform the public." The statewide network is still in formation with nearly 100 Lesbian/Gay/Bisexual and ally WEARING THE GREEN— marchers Gay and Lesbian make their debut during the San Francisco St. -

ROUGHLY EDITED TRANSCRIPT BUREAU of LAND MANAGEMENT WILD HORSE and BURRO ADVISORY BOARD OCTOBER 18, 2017 8:00 A.M. Capt
ROUGHLY EDITED TRANSCRIPT BUREAU OF LAND MANAGEMENT WILD HORSE AND BURRO ADVISORY BOARD OCTOBER 18, 2017 8:00 A.M. Captioning Provided by: Closed Caption Productions, LLC www.CaptionFamily.com Phone: (800) 335-0911 * * * REALTIME CAPTIONING AND/OR CART (COMMUNICATIONS ACCESS REALTIME TRANSLATION) ARE PROVIDED IN ORDER TO FACILITATE COMMUNICATION ACCESSIBILITY AND MAY NOT BE A TOTALLY VERBATIM RECORD OF THE PROCEEDINGS. * * * >> KATHIE LIBBY: So let's all get settled. Folks let's get settled. Okay, folks. >> DR. SUE McDONNELL: Kathie? >> KATHIE LIBBY: It was a long day yesterday and we have a really, really good day today. Really a bunch of issues were really looking forward to, and I will go over that in a minute. Let me just say very briefly about that very long rules of room thing. This is the tape that says, the public is here and the board is here because this basically is a board meeting and the public comment section is over. So typically the speakers are speaking to the board and the board is questioning and getting additional information from the speakers and we are all listening in, taking notes. Again, the presentations will be posted so you don't have to take down every single word you hear. Those will be available to you next week. So this morning, everything over to Dr. Julie. We are going to hear -- and this is something we talk about all the time, kind of no matter where we sit, is that we need to be more collaborative. We will talk about some really important Colorado collaborative partnerships. -

CALIFORNIA STATE UNIVERSITY, NORTHRIDGE 16 BARS a Thesis
CALIFORNIA STATE UNIVERSITY, NORTHRIDGE 16 BARS A thesis submitted in partial fulfillment of the requirements For the degree of Master of Arts in Screenwriting by John Reyes Cadiente May 2013 The thesis of John Reyes Cadiente is approved: Rappaport, Jared H, MFA Date Krasilovsky, Alexis R, MFA Date Sturgeon, Scott, MFA, Chair Date California State University, Northridge ii DEDICATION This thesis is dedicated to: My family. With their unconditional love and support, anything is possible. iii TABLE OF CONTENTS Signature Page…………………………………………………………………………… ii Dedication ……………………………………………………………………………….iii List of Tables …………………………………………………………………………….iv Abstract …………………………………………………………………………………v 16 BARS ………………………………………………………………………………….1 iv ABSTRACT 16 BARS by John Reyes Cadiente Master of Arts in Screenwriting When Jake, a witty high school student with a knack for hip-hop music, gets kicked out of his home and sent to a continuation school, he must now find his way back by surviving the school and ultimately becoming his own man. v OVER BLACK CHEERS of hundreds of rowdy teenagers uproar with excitement. HEAVY BREATHING of a boy who awaits to be brought on stage. EMINEM'S "TILL I COLLAPSE" plays. FADE IN. DREAM SEQUENCE INT. AUDITORIUM - NIGHT It's dark backstage. JAKE, 17 and short, breathes heavily and jitters behind the curtains. He wears a hoodie over his head similar to a boxer whose about to enter a ring. The song kicks it up a notch when a low rumbling of GUITARS and DRUM thumps build up. A hear thumping rhythm develops. The crowd outside sings along with the backing vocals. YO LEFT... YO LEFT... YO LEFT, RIGHT, LEFT! Jake looks down at his SCUFFED UP NIKE'S to catch light underneath the curtains hitting it. -
Jack Stauber
Issue 51 December 2018 Issue 51 ONLINE www.thecutmagazine.com FACEBOOK www.facebook.com/TheCutMagazine ADDRESS The Cut Magazine 5000 Forbes Avenue UC Box 122 Pittsburgh, PA 15238 COVER PHOTO Cassandra Scheirer December 2018 Editor-in-Chief Brooke Ley Assistant Editor Trevor Lazar Photo Editor Matthew McGehee PR Editors Dalia Laredo Issue 51 CJ Rosado Letter Design Editor Jackie Chou Copy Editor Wilson Ekern From Writing Staff Amanda Vallon Clara Enders Clare Lai The Claudia Osorio Emma Blank Izzy Sio Jamie McArthur Editor Julianne Tippett Julie Heming Leila Berger Winter has come in best soundtracks. Finally, if you holiday cheer. Lexie Rodriguez Pittsburgh, despite what the you’re looking to leave your I’m also particularly fond Megan Naji recent 60° day might make significant other before you of this issues mixtape, an Mei Leng you think. With the changing have to bring them home for imagining of a new Shrek Michelle Ng of seasons comes the joy of the holidays, check out Clare movie through its potential Omasan Richardson finals and the push towards Lai’s write up on breakup soundtrack. I had the Shrek Shambhavi Mishra the end of the semester. What songs. If you’re the one who soundtrack on CD growing better way to cheer yourself up has been broken-up with, up, so this one hit particularly and relax than with Carnegie check out Jamie McArthur’s close to home. "My Beloved Design Staff Arpita Nag Mellon’s very own music guide to Joji who can help you Monster" by the Eels still goes Jenna Kim magazine. -
Zine Iss2.Pdf
3 Notes from a deranged mind... Contents Well, here we are once again, a fresh issue to have and to hold. A lot Witchery....................................................................................................................4 has happened since issue one, but I’ll be damned if I can remember what Criminal.....................................................................................................................6 those things were. Well, for one thing, the kind people at various record Grip Inc......................................................................................................................8 companies have kept me in the light with regards to the happenings in the Vader....................................................................................................................... 11 biz, good friends have kept me occupied, and work hasn’t killed me yet. Crucible.................................................................................................................. 14 7KLVLVVXHLVTXLWHDELWODUJHUWKDQWKH¿UVWRQH ZLWKDGHFUHDVHLQWH[W Arch Enemy .......................................................................................................... 17 size, so get your reading glasses!), so hopefully you’ll have more to read Amon Amarth...................................................................................................... 18 XQWLOWKHQH[WLVV$QGVSHDNLQJRIWKHQH[WLVVXH,¶YHDOUHDG\JRWDERXW March Metal Meltdown................................................................................... -

Baptist University Scholarly Commons @ Ouachita
Ouachita Baptist University Scholarly Commons @ Ouachita Arkansas Baptist Newsmagazine, 1960-1964 Arkansas Baptist Newsmagazine 10-17-1963 October 17, 1963 Arkansas Baptist State Convention Follow this and additional works at: https://scholarlycommons.obu.edu/arbaptnews Part of the Christianity Commons, and the Mass Communication Commons Recommended Citation Arkansas Baptist State Convention, "October 17, 1963" (1963). Arkansas Baptist Newsmagazine, 1960-1964. 222. https://scholarlycommons.obu.edu/arbaptnews/222 This Book is brought to you for free and open access by the Arkansas Baptist Newsmagazine at Scholarly Commons @ Ouachita. It has been accepted for inclusion in Arkansas Baptist Newsmagazine, 1960-1964 by an authorized administrator of Scholarly Commons @ Ouachita. For more information, please contact [email protected]. Arlansa~ Baptist OCTOBER 17, 1963 'today in your home, your church, your community, as compared with f~ve year~ ago! Well, go on from here. We're out of space and personally speaking the ball ~as dQne stopped bouncing l ~~~~A~ 7~e dtJet~eet,l,9 dall 1\ /fY fellow church member :aob Crafton, of Cen lV.ltral Chur.ch, North Little Rock, tells about a IN THIS ISSUE:- young surgeon who undertook to operate on a man for the removal of a ping-pong ball the man had ) . swallowed. Inste~d of one incision, the surgeon UTSIDE forces which would use the church for made half a dozen, at widely scattered points over 0 their own ends come under scrutiny in a series the patient's chest and abdomen. of articles by the Christian Life Commission. The Soon after the operation(s), an old, experi first of these provocative discussions is on page 8. -

Indie Rock Subculture: Hamilton As Microcosm Indie Rock Subculture: Hamilton As Microcosm
INDIE ROCK SUBCULTURE: HAMILTON AS MICROCOSM INDIE ROCK SUBCULTURE: HAMILTON AS MICROCOSM By KATHLEEN DAVIES, B.A. A Thesis Submitted to the School of Graduate Studies In Partial Fulfilment of the Requirements for the Degree Master of Arts McMaster University © Copyright by Kathleen Davies, April 2006 MASTER OF ARTS (2006) McMaster University (Music Criticism) Hamilton, Ontario TITLE: Indie Rock Subculture: Hamilton as Microcosm AUTHOR: Kathleen Davies, B.A. (McMaster University) NUMBER OF PAGES: v, 123 11 ABSTRACT In recent years, interest in the indie rock subculture has exploded, both in the popular press and among popular music scholars and culture theorists. This is an ethnographic study of the indie rock scene in Hamilton, Ontario. Hamilton represents a microcosm of what is happening in other local indie scenes. The geographical, historical and cultural locality of Hamilton creates a sense of shared identity among individuals connected by the common interest in indie rock. This study focuses on how independent rock's network of social practices and economic institutions works to locate subjects within Hamilton's local network while connecting them to the larger framework of interlocal scenes. Aspects of the local and interlocal are explored through narratives of indie aesthetics, style, fashion, institutions, cultural practices, authenticity and investment. Cultural practices, including the production and consumption of indie rock are examined through the lens of Bourdieu' s concept of cultural capital, which exposes constructions and configurations of class, generation, ethnicity, and gender. 111 ACKNOWLEDGEMENTS Thank you to: Dr. Susan Fast for her encouragement to pursue my Masters degree. Dr. Christina Baade. As my supervisor of research, her guidance and encouragement helped ensure this project came to fruition.