Emotional Granularity: Definition, Measurement, and Relationship to Cardiovascular Physiological Activity
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Psychology 3131 Professor June Gruber Human Emotion
Human Emotion Psychology 3131 Professor June Gruber Human Emotion What is an Emotion? QUESTIONS? William James “To the psychologist alone can such questions occur as: Why do we smile, when pleased, and not scowl? Why are we unable to talk to a crowd as we talk to a single friend? Why does a particular maiden turn our wits upside-down?” James, W. (1982). Psychology - Briefer course. New York: Henry Holt. New edition, New York: Harper & Row, 1961. William James “The common man can only say: "Of course we smile, of course our heart palpitates at the sight of the crowd, of course we love the maiden. And so, probably, does each animal feel about the particular things it tends to do in the presence of certain objects...” James, W. (1982). Psychology - Briefer course. New York: Henry Holt. New edition, New York: Harper & Row, 1961. Roadmap Theories of emotion Components Classification Expert Interview Roadmap TheoriesTheories ofof emotionemotion Components Classification Expert Interview Theories of Emotion Timeline Theories ofEmotion Ancient Greek Enlightenment Darwin William James James-Lange Cannon-Bard Schachter-Singer Lazarus Theories of Emotion Timeline Hippocrates: 4 Humors Aristotle: Moderation principle Ancient Greek “Getting angry or sad is easy and anyone can do it; but doing it... in the right amount, at the right time, and in the right way is not easy, nor can everyone do it.” - ARISTOTLE, Nicomachean Ethics, 11.9, 1109a27 Theories of Emotion Timeline Descartes Spinoza Hume Enlightenment Theories of Emotion Timeline Evolutionary Approach Expression of Emotions in Man & Animals Emotions evolutionarily evolved, serve survival purpose Darwin Immediately a bestseller of it’s time (over 5,000 copies) 1st Scientific Treatment of Emotion Includes survey data Observations of healthy and mentally ill individuals Personal anecdotes (e.g., grief expressions in Darwin’s own family after death) Darwin’s Three Principles Darwin’s Three Principles I. -

Solving the Emotion Paradox: Categorization and the Experience of Emotion
Personality and Social Psychology Review Copyright © 2006 by 2006, Vol. 10, No. 1, 20–46 Lawrence Erlbaum Associates, Inc. Solving the Emotion Paradox: Categorization and the Experience of Emotion Lisa Feldman Barrett Department of Psychology Boston College In this article, I introduce an emotion paradox: People believe that they know an emo- tion when they see it, and as a consequence assume that emotions are discrete events that can be recognized with some degree of accuracy, but scientists have yet to pro- duce a set of clear and consistent criteria for indicating when an emotion is present and when it is not. I propose one solution to this paradox: People experience an emo- tion when they conceptualize an instance of affective feeling. In this view, the experi- ence of emotion is an act of categorization, guided by embodied knowledge about emotion. The result is a model of emotion experience that has much in common with the social psychological literature on person perception and with literature on em- bodied conceptual knowledge as it has recently been applied to social psychology. Humans experience emotion. For many, experience people feel fear when their fear mechanism has trig- serves as an emotion’s central and defining aspect. We gered, such that this feeling shapes perception and feel the heat of anger, the despair of sadness, the dread decision making and can have important conse- of fear. Most days, at least in North America, each of us quences for social relationships. asks and answers about our emotional state. We talk Although there is accumulating evidence that the about our experiences of emotion over coffee, or dur- experience of emotion can have great consequence for ing a telephone conversation, or in a therapist’s office. -

Download Preprint
From Electric Shocks to the Electoral College: How Boredom Steers Moral Behavior Meltem Yucel Department of Psychology, University of Virginia Erin C. Westgate Department of Psychology, University of Florida ***Preprint*** To appear in A. Elpidorou (Ed.), The Moral Psychology of Boredom. London: Rowman & Littlefield. From Electric Shocks to the Electoral College: How Boredom Steers Moral Behavior Among charming tales of quirky haircuts conjured up out of boredom, lurk more chilling stories. On June, 2017, motorists in Ireland were disturbed by an odd sight: a man on a bridge, aiming a gun. When police arrived, they found a teenager, perched above an Irish highway overpass, centering passing cars in the sights of his 6mm air rifle. When asked later in court, he explained simply: he was “bored” (Ferguson and McLean 2019). Although boredom has been associated with prosocial behavior (e.g., van Tilburg and Igou 2017), it has also been associated with a wide array of morally questionable and disturbing outcomes, including self-harm (Nederkoorn et al. 2016), reckless driving (Steinberger et al. 2017), and sadism (Pfattheicher et al. 2020). We all experience boredom, from being stuck in airport security lines to reading poorly written book chapters. But what is boredom, why do we experience it, and what happens when we do? We suggest a new take on this everyday emotion as an important and useful cue that we are not cognitively engaged in meaningful experiences. According to the Meaning and Attentional Components (MAC) model of boredom, people feel bored when they cannot successfully engage their attention in meaningful activities. Boredom can be painful, but it provides important feedback about our lives, by signaling a lack of meaningful attentional engagement. -

The Future of Psychology: Connecting Mind to Brain
PERSPECTIVES ON PSYCHOLOGICAL SCIENCE The Future of Psychology Connecting Mind to Brain Lisa Feldman Barrett Boston College, Massachusetts General Hospital, and Harvard Medical School ABSTRACT—Psychological states such as thoughts and feel- footbridge and more like a tightrope requiring lightness of foot and ings are real. Brain states are real. The problem is that the a really strong safety net. Mind–brain, and relatedly, behavior– two are not real in the same way, creating the mind–brain brain, correspondence continue to be central issues in psychology, correspondence problem. In this article, I present a possible and they remain the largest challenge in 21st-century psychology. solution to this problem that involves two suggestions. First, The difficulty in linking the human mind to behavior on the one complex psychological states such as emotion and cognition hand and to the brain on the other is rooted, ironically enough, in can be thought of as constructed events that can be causally the way the human brain itself works. Human brains categorize reduced to a set of more basic, psychologically primitive continuously, effortlessly, and relentlessly. Categorization plays a ingredients that are more clearly respected by the brain. fundamental role in every human activity, including science. Second, complex psychological categories like emotion and Categorizing functions like a chisel, dividing up the sensory world cognition are the phenomena that require explanation in into figure and ground, leading us to attend to certain features and psychology, and, therefore, they cannot be abandoned by to ignore others. Via the process of categorization, the brain science. Describing the content and structure of these cate- transforms only some sensory stimulation into information. -

Historical Pitfalls and New Directions in the Neuroscience of Emotion
G Model NSL-32985; No. of Pages 10 ARTICLE IN PRESS Neuroscience Letters xxx (2017) xxx–xxx Contents lists available at ScienceDirect Neuroscience Letters jo urnal homepage: www.elsevier.com/locate/neulet Review article Historical pitfalls and new directions in the neuroscience of emotion a,b,∗ c Lisa Feldman Barrett , Ajay B. Satpute a Department of Psychology, Northeastern University, Boston, MA, United States b Athinoula A. Martinos Center for Biomedical Imaging and Department of Psychiatry, Massachusetts General Hospital and Harvard Medical School, Charlestown, MA, United States c Departments of Psychology and Neuroscience, Pomona College, Claremont, CA, United States h i g h l i g h t s • A dynamic, systems-based neuroscience view of emotion is proposed. • An emotion word refers to a population of highly variable, situated instances. • Emotions are not reactions to the world, but are predictions corrected by sensory inputs. • Prediction signals are concepts that categorize and explain the causes of sensations. • Affect is a property of consciousness and is not synonymous with emotion. a r t i c l e i n f o a b s t r a c t Article history: In this article, we offer a brief history summarizing the last century of neuroscientific study of emotion, Received 2 April 2017 highlighting dominant themes that run through various schools of thought. We then summarize the Received in revised form 25 July 2017 current state of the field, followed by six key points for scientific progress that are inspired by a multi-level Accepted 25 July 2017 constructivist theory of emotion. Available online xxx © 2017 Elsevier B.V. -

CURRICULUM VITAE Lisa Feldman Barrett
CURRICULUM VITAE Lisa Feldman Barrett INFORMATION Northeastern University: Massachusetts General Hospital - East: Department of Psychology Martinos Center for Biomedical Imaging, and 253 Nightingale Hall Psychiatric Neuroimaging Research Program & Northeastern University Gerontology Research Unit Boston, MA 02115 Building 149, 13th Street, Rm. 10-018 617.373.2044 (voice) Charlestown, MA 02129 617.373-8714 (fax) 617.724.2324 (voice) Internet Correspondence: [email protected] http://www.affective-science.org h-index = 78 (Google Scholar) EDUCATION 2004 Fellow, National Science Foundation Advanced Training Institute in Immersive Virtual Environment Technology and Social Psychology, University of California, Santa Barbara 2000 Fellow, American Psychological Association's Advanced Training Institute in Functional Magnetic Resonance Imaging, Boston. 1995 Fellow, National Science Foundation Training Institute for Cardiovascular Approaches to Social Psychophysiology, State University of New York, Buffalo. 1992 Ph.D., Clinical Psychology, University of Waterloo 1992 Clinical Internship, University of Manitoba Medical School 1986 B.Sc., Psychology, with honors, University of Toronto ACADEMIC EMPLOYMENT 2013- University Distinguished Professor of Psychology, Northeastern University 2010-2013 Distinguished Professor of Psychology, Northeastern University 2003-2010 Professor of Psychology, Boston College 1999-2003 Associate Professor of Psychology, Boston College 1996-1999 Assistant Professor of Psychology, Boston College 1992-1996 Assistant Professor -

POL 373H1F: the Emotions and Political Theory
POL 373Y: The Emotions and Political Theory Lectures: Wednesdays 12 to 2 Instructor: Rebecca Kingston, Associate Professor of Political Science Office Hours: Wednesdays 3 to 5, Sid Smith 3117 Contact info: (416) 946- 0187 or [email protected] Course Description: Despite some renderings of the art of proper political thinking as the search for the supremacy of reason over passion, recent scholarship across the humanities and social sciences has revealed the multiple ways in which emotion can be recognised as a key component of morality and good politics. Revisionist approaches to the history of political thought have come to recognise that many political theorists writing prior to the twentieth century were more receptive to emotion as a positive political force than previously acknowledged. Through deeper exploration of the history of political thought, theorists have found more appealing and sophisticated accounts of the place that emotions play in political life and in normative theories of morals and politics. In this context, this course has two objectives. The first objective is to explore the work of some important thinkers in the history of political thought with a focus on their conception of emotion and of emotion’s place in political life. While thinkers are chosen selectively, a reading of their ideas will provide us with a map of competing ways in which an appreciation of emotion can be understood and integrated into a theory of politics. The first half of the course will allow students to see some of the historical development of competing models of the place of emotion in politics. -

The New Science of Emotions with Lisa Feldman Barrett Full Episode
The New Science of Emotions with Lisa Feldman Barrett Full Episode Transcript With Your Host The Brainfluence Podcast with Roger Dooley The New Science of Emotions with Lisa Feldman Barrett Welcome to the Brainfluence Podcast with Roger Dooley, author, speaker and educator on neuromarketing and the psychology of persuasion. Every week, we talk with thought leaders that will help you improve your influence with factual evidence and concrete research. Introducing your host, Roger Dooley. Roger Dooley: Welcome to the Brainfluence Podcast. I'm Roger Dooley. As marketers, as leaders, and team members, and in many other roles, we all know how important emotions are. The driving force behind neuro- marketing is the understanding that humans are not logical robots making rational decisions. Our guest this week is a true expert in emotions. She's conducting original research that some say is changing our understanding of the science of emotion in the same way that relativity revolutionized physics and natural selection changed biology. She is a university distinguished professor of psychology at Northeastern University and directs the Affective Science Lab there and that's Affective with an A, by the way, although they are probably effected with an E there as well. Her new book is How Emotions Are Made. The Secret Life of the Brain. Welcome to the show, Lisa Feldman Barrett. Lisa Barrett: Thanks so much for inviting me on your show, Roger. Roger Dooley: Great. Let me start by saying, Lisa, that scientists like you are making life really difficult for people like me, who try to turn academic research into practical business advice. -

Actually Embodied Emotions
University of Pennsylvania ScholarlyCommons Publicly Accessible Penn Dissertations 2018 Actually Embodied Emotions Jordan Christopher Victor Taylor University of Pennsylvania, [email protected] Follow this and additional works at: https://repository.upenn.edu/edissertations Part of the Philosophy of Science Commons, and the Psychology Commons Recommended Citation Taylor, Jordan Christopher Victor, "Actually Embodied Emotions" (2018). Publicly Accessible Penn Dissertations. 3192. https://repository.upenn.edu/edissertations/3192 This paper is posted at ScholarlyCommons. https://repository.upenn.edu/edissertations/3192 For more information, please contact [email protected]. Actually Embodied Emotions Abstract This dissertation offers a theory of emotion called the primitivist theory. Emotions are defined as bodily caused affective states. It derives key principles from William James’s feeling theory of emotion, which states that emotions are felt experiences of bodily changes triggered by sensory stimuli (James, 1884; James, 1890). However, James’s theory is commonly misinterpreted, leading to its dismissal by contemporary philosophers and psychologists. Chapter 1 therefore analyzes James’s theory and compares it against contemporary treatments. It demonstrates that a rehabilitated Jamesian theory promises to benefit contemporary emotion research. Chapter 2 investigates James’s legacy, as numerous alterations of his theory have influenced the field of emotion research over the past fifty years, including so-called neo-Jamesian theories. This chapter argues that all these variations of the Jamesian theory assume that emotions require mental causes, whether in the form of evaluative judgments or perceptual contents. But this demand is not present in James’s theory. Nor, as Chapter 3 demonstrates, is this assumption necessary or even preferable for a fecund theory that explains human and non-human emotions. -
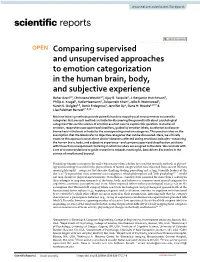
Comparing Supervised and Unsupervised Approaches to Emotion Categorization in the Human Brain, Body, and Subjective Experience
www.nature.com/scientificreports OPEN Comparing supervised and unsupervised approaches to emotion categorization in the human brain, body, and subjective experience Bahar Azari1,9, Christiana Westlin2,9, Ajay B. Satpute2, J. Benjamin Hutchinson3, Philip A. Kragel4, Katie Hoemann2, Zulqarnain Khan1, Jolie B. Wormwood5, Karen S. Quigley2,6, Deniz Erdogmus1, Jennifer Dy1, Dana H. Brooks1,10* & Lisa Feldman Barrett2,7,8,10* Machine learning methods provide powerful tools to map physical measurements to scientifc categories. But are such methods suitable for discovering the ground truth about psychological categories? We use the science of emotion as a test case to explore this question. In studies of emotion, researchers use supervised classifers, guided by emotion labels, to attempt to discover biomarkers in the brain or body for the corresponding emotion categories. This practice relies on the assumption that the labels refer to objective categories that can be discovered. Here, we critically examine this approach across three distinct datasets collected during emotional episodes—measuring the human brain, body, and subjective experience—and compare supervised classifcation solutions with those from unsupervised clustering in which no labels are assigned to the data. We conclude with a set of recommendations to guide researchers towards meaningful, data-driven discoveries in the science of emotion and beyond. Psychology became a science in the mid-19th century when scholars frst used the research methods of physiol- ogy and neurology to search for the physical basis of mental categories that were inherited from ancient Western mental philosophy—categories that describe thinking, feeling, perceiving and acting. Scientifc leaders of the day (e.g.1,2) warned that these common-sense categories, which philosophers call “folk psychology”3–7, would not map cleanly to physical measurements. -

Viewpoints: Approaches to Defining and Investigating Fear
SUPPLEMENTARY INFORMATION q&a In the format provided by the authors and unedited. Viewpoints: Approaches to defining and investigating fear Interviewed by Dean Mobbs 1, Ralph Adolphs 1, Michael S. Fanselow 2, Lisa Feldman Barrett3,4, Joseph E. LeDoux5,6,7, Kerry Ressler8,9 and Kay M. Tye10 NatURE NEUROSCIENCE | www.nature.com/natureneuroscience Supplementary Note 1 Fear: The Awareness that You Are in Harm’s Way Joseph LeDoux A Snapshot of My view of Fear Fear is a conscious experience in which you come to believe that you are about to be harmed (LeDoux, 2015, 2017, 2019; LeDoux and Pine, 2016; LeDoux and Brown, 2017; LeDoux and Hofmann, 2018; LeDoux et al, 2018). Such a subjective state of inner awareness, of phenomenological consciousness (LeDoux, 2019; Brown et al, 2019), can result from the presence of an innate or learned threat, but also by misattributing danger to a benign stimulus or situation, or also by imagining the possibility of harm in the near or distal future, even when such a possibility is improbable or even physically impossible. All that is necessary is your expectation or prediction that this is the case, which occurs when a mental model of fear is pattern-completed using your ‘fear schema’--the unique collection of memories about threat, fear, danger, that you have accumulated throughout life. But if you don’t apprehend that it is you that is to be harmed by the threat, you cannot experience fear—no self, no fear. Your ‘self schema,’ your repository of ‘you,’ must therefore also be involved in the mental model for the experience of fear to result. -
Thesis Entitled: Subjective Wellbeing As an Affective Construct
Subjective Wellbeing As An Affective Construct By Melanie Therese Davern BSc (Hons) Submitted in fulfilment of the requirements for the award of Doctor of Philosophy Deakin University November 2004 1 DEAKIN UNIVERSITY CANDIDATE DECLARATION I certify that the thesis entitled: Subjective Wellbeing as an Affective Construct Submitted for the degree of: Doctor of Philosophy Is the result of my own research, except where otherwise acknowledged, and that this thesis in whole or in part has not been submitted for an award, including a higher degree, to any other university or institution. Full Name.................................................…………………………………. (Please Print) Signed ..................................................................................………………. Date......................................................................................………………. 2 Acknowledgements I am indebted to Professor Robert Cummins for his supportive, challenging and stimulating supervision of this thesis. It was a privilege to work with such a passionate and committed academic and I am extremely grateful for his endless hours of editing and intellectual discussions. I would also like to thank my devoted husband Stephen for engaging in countless hours of discussion and all of my extended family for providing endless support during my study. Finally, I would like to thank my kind mother Regina for her numerous hours of final proofreading. 3 TABLE OF CONTENTS EXECUTIVE SUMMARY ............................................................................................