Rail Accident Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

'Gold Status' Lydney Town Council Achieves
branch line. branch country country typical a of pace relaxing the experience to can get off to explore the local area and get and area local the explore to off get can a chance chance a 5 stations so you you so stations 5 with Railway Heritage d an Steam ET 4 15 GL dney, y L Road, Forest tation, S chard or N days ected sel Open 845840 01594 and from railway building. railway from and later benefited from the growth of the ironworks into a tinplate factory factory tinplate a into ironworks the of growth the from benefited later trade of the Forest of Dean began to transform Lydney’s economy, which which economy, Lydney’s transform to began Dean of Forest the of trade 19th century the building of a tramroad and harbour to serve the coal coal the serve to harbour and tramroad a of building the century 19th Lydney’s harbour area was always strategically important and in the early early the in and important strategically always was area harbour Lydney’s of the 17th century and the reclamation of saltmarsh in the early 18th. early the in saltmarsh of reclamation the and century 17th the of establishment of ironworks at the start start the at ironworks of establishment Its owners also profited from the the from profited also owners Its deposits, and extensive woodland. woodland. extensive and deposits, resources, including fisheries, mineral mineral fisheries, including resources, free cafe, and local farm shop and deli. and shop farm local and cafe, free Picture framing and gift shop. -

World Heritage Site – Kalka Shimla Railway an Introduction
WORLD HERITAGE SITE – KALKA SHIMLA RAILWAY AN INTRODUCTION Ambala Division is the proud custodian of “WORLD HERITAGE SITE-KALKA SHIMLA RAILWAY”. The heritage status to KSR was awarded on 7th July, 2008 by UNESCO. Shimla (then spelt Simla) was settled by the British shortly after the first Anglo- Gurkha war and is located at 7,116 feet(2,169m) in the foothills of the Himalaya. By the 1830s, Shimla had already developed as a major base for the British. It became the summer capital of British India in 1864, and also the Headquarters of the British army in India. The Kalka- Shimla Railway was built to connect Shimla, the summer capital of India during the British Raj, with the Indian rail system. “The Guinness Book of Rail facts & feats” records Kalka Shimla Railways as the greatest narrow gauge engineering in India. It is indeed true, construction of 103 tunnels (102 Existing) aggregating five miles and over 800 bridge in three years, that too in rough and hostile terrain was not an easy task. The Historic, approximate 111 years old KLK-SML Railway line which was opened for public traffic on 9th Nov.1903, became UNESCO Declared world Heritage Railway line, when it was conferred Heritage status on 10th July 2008 & listed under “Mountain Railways of India”. The idea of a Railway line to Shimla dates back to the introduction of Railways in India. It is said that in The DELHI GAZETTE, a correspondent in November, 1847 sketched the route of railway to Shimla with the estimates of the traffic returns etc in appropriate style. -

Forest of Dean & Wye Valley Self Catering Holidays
FOREST OF DEAN & WYE VALLEY SELF CATERING HOLIDAYS Stank Farm, known to some locals as 'the stank', is situated in the picturesque village of Clearwell within walking distance of Clearwell Castle and Caves & Puzzle Wood. 'The stank' you will be relieved to hear is a very old word for pond or body of water and has nothing to do with the word stink! Ask the owners about the farm's history. The village also boasts 2 pubs, restaurants, cafe and a recreational ground. Nearby is Perrygrove steam railway and The Iron Age Experience. The old market town of Coleford only 2 miles away is a thriving community where all provisions can be bought 7 days a week. The Grade II listed farmhouse we believe dates back to 16th Century. The Lodge is a wooden log cabin that is set away from the house and sleeps 4/6 people. All of the self-catered accommodation has private access and outside space and all guests are welcome to enjoy the land and help on the farm if they would like to. The farm house and outbuildings are set within 17 acres with a stream running through and depending on the time of year there are sheep, cattle, pigs & chickens. The owners Andrew & Louise Salter and their 2 children William aged 14 and Lily aged 11. They offer a relaxing, comfortable and tranquil holiday within easy reach of the Royal Forest of Dean, Wye Valley and Vale of Leadon. The surrounding area offers walking, cycling, riding, climbing, canoeing, fishing, quad biking etc, Symonds Yat, Tintern, Monmouth, Clearwell castle, Welsh mountains, Newent, Ross- on-Wye and many other pretty villages and for younger children, Clearwell Caves, Dean Forest Railway, Model Village, Butterfly Zoo and plenty of nature trails etc. -

Hope Mansell, Lea Bailey, and Wigpool the White House with Its Distinctive Tower Distance, and Cross a Footbridge and Stile
Walking Through Dean History Walk Eleven Walk 11 7½ or 5 miles (12 or 8 km) Hope Mansell, Lea Bailey, and Wigpool The white house with its distinctive tower distance, and cross a footbridge and stile. is Euroclydon (1). Continue to the far end Pass to the left of a house (Bailey Brook of the field, where there is a gap and a stile. Cottage) onto a lane and follow this uphill A lovely secluded valley, a gold mine, Wigpool iron mine (including a WW2 Follow the narrow path beyond down to to a junction. Turn right here to follow a ‘cinema’), and extensive views. A hilly walk on field paths, woodland tracks, a tarmac road. Turn left and then right in gravel track just on the edge of a conifer and lanes; can be muddy; the section around Wigpool Common requires front of the first house (‘Greystones’). The plantation (Lea Bailey Inclosure), keeping careful navigation; 9 stiles. path heads uphill, initially between stone left past a driveway. Bear right at a junction walls, to a gate. Keeping the hedge on to go behind two houses (Newtown!), and START at one of the parking areas on either side of the unclassified road your left, continue uphill through another keep left at another to go up a small valley between Drybrook and Mitcheldean, on the sharp bend a little under a gate. Beyond this there is a good view to to a junction of several tracks. Take the mile from Drybrook and just over half a mile from Mitcheldean (the top of the left of Drybrook and Ruardean Hill, one that goes half right past a barrier to a Stenders Hill): GR SO 656180. -

Statement of Consultation
Gloucestershire Waste Core Strategy (WCS) Regulation 30(d) Statement of Consultation Prepared in accordance with Regulation 30(d) of the Town & Country Planning (Local Development) (England) (Amendment) Regulations 2008 September 2011 1 Contents 1. Introduction 2. Who was consulted? 3. How were they consulted? 4. How many responses were received? 5. What were the main issues raised and how have these been taken into account? APPENDICES Appendix 1 – Schedule of Key Issues Appendix 2 – List of consultees Appendix 3 – Waste forum attendees (March 2006) Appendix 4 – Waste forum attendees (October 2007) 2 1. Introduction 1.1 This ‘statement of consultation’ has been produced in support of the publication Gloucestershire Waste Core Strategy (WCS) December 2010 and fulfils the requirements of Regulation 27 and 30(d) of the Town and Country Planning (Local Development) (England) (Amendment) Regulations 2008. 1.2 The purpose of the statement is to set out the following: . Which bodies and persons were invited to make representations during the preparation of the WCS (the stage known as ‘Regulation 25’) . How those bodies and persons were invited to make those representations . A summary of the main issues raised; and . How those issues have been addressed in the WCS. 1.3 Preparation of the WCS has taken place in three main stages; issues and options (2006) preferred options (2008) and site options (2009). A certain amount of ongoing consultation has also been carried out in between each stage. 1.4 Below we outline who was consulted at each stage, how they were consulted, the main issues raised and how these have been taken into account in the publication WCS. -

Walk Westward Now Along This High Ridge and from This Vantage Point, You Can Often Gaze Down Upon Kestrels Who in Turn Are Scouring the Grass for Prey
This e-book has been laid out so that each walk starts on a left hand-page, to make print- ing the individual walks easier. When viewing on-screen, clicking on a walk below will take you to that walk in the book (pity it can’t take you straight to the start point of the walk itself!) As always, I’d be pleased to hear of any errors in the text or changes to the walks themselves. Happy walking! Walk Page Walks of up to 6 miles 1 East Bristol – Pucklechurch 3 2 North Bristol – The Tortworth Chestnut 5 3 North Bristol – Wetmoor Wood 7 4 West Bristol – Prior’s Wood 9 5 West Bristol – Abbots Leigh 11 6 The Mendips – Charterhouse 13 7 East Bristol – Willsbridge & The Dramway 16 8 Vale of Berkeley – Ham & Stone 19 Walks of 6–8 miles 9 South Bristol – Pensford & Stanton Drew 22 10 Vale of Gloucester – Deerhurst & The Severn Way 25 11 Glamorgan – Castell Coch 28 12 Clevedon – Tickenham Moor 31 13 The Mendips – Ebbor Gorge 33 14 Herefordshire – The Cat’s Back 36 15 The Wye Valley – St. Briavels 38 Walks of 8–10 miles 16 North Somerset – Kewstoke & Woodspring Priory 41 17 Chippenham – Maud Heath’s Causeway 44 18 The Cotswolds – Ozleworth Bottom 47 19 East Mendips – East Somerset Railway 50 20 Forest of Dean – The Essence of the Forest 54 21 The Cotswolds – Chedworth 57 22 The Cotswolds – Westonbirt & The Arboretum 60 23 Bath – The Kennet & Avon Canal 63 24 The Cotswolds – The Thames & Severn Canal 66 25 East Mendips – Mells & Nunney 69 26 Limpley Stoke Valley – Bath to Bradford-on-Avon 73 Middle Hope (walk 16) Walks of over 10 miles 27 Avebury – -

May 2015 1 Reason #33 DESTINATION for a LIFETIME Main-Level Living at Its Best
RIDE Magazine | May 2015 1 Reason #33 DESTINATION for a LIFETIME Main-level living at its best. There’s a lot to love about our well-appointed Tidewater homes—now welcoming families to Potomac Shores. Choose from fi ve new neighborhoods by two national builders. Traditional and main-level living with indoor/outdoor fl oorplans. Over a dozen home designs with two to seven bedrooms. And golf or forest views. It’s resort-style living only 30 miles from DC. Where every home comes with an exquisite community. VRE Station on track. Award-winning homes from the mid $400s CALL OR VISIT THE GREETING HOUSE: 855-808-6051 2175 Potomac River Blvd., Potomac Shores, VA 22026 PotomacShores.com GPS address: Harbor Station Parkway, Dumfries, VA 22026 Features and products vary by community. Price, offers, fi nancing and availability are subject to change without notice. RIDE Magazine | May 2015 1 CONTENTS RIDE MAGAZINE | MAY 2015 FROM THE CEO 02 | FRENCH TALL SHIP L’HERMIONE TO MEET VRE MANAGEMENT VISIT ALEXANDRIA very spring, VRE launches our 03 | VRE PARTICIPATES IN NTSB AND Meet the Management events AMTRAK SAFETY AND SECURITY at our five busiest destination EVENTS E stations. Meet the Management enables me and our VRE team the DOUG ALLEN 04 | JOIN VRE FOR MEET THE MANAGEMENT opportunity to personally meet you, Chief Executive Officer our passengers, and listen to your suggestions and ideas to improve VRE. 05 | IMPROVING RAIL SERVICE FROM In April, we hosted our first Meet the Management event at Washington’s WASHINGTON TO RICHMOND Union Station. We will be at the following stations for evening trains in the upcoming weeks: 06 | THE VIRGINIA ASSOCIATION OF RAILWAY PATRONS WORKS FOR YOU Wednesday, May 13 - L’Enfant Wednesday, May 20 - Crystal City 07 | SPOTLIGHT ON KEOLIS MEET RANDY ANDES Wednesday, May 27 - Alexandria Wednesday, June 3 - Franconia/Springfield We will be serving refreshments, giving away promotional items and hosting hands-on demos showcasing VRE Mobile, our new mobile ticketing Get Noticed with app, launching later this month. -

1 a New Age of Steam?
A new age of steam? The Tua Valley Line, Portugal - Experience and Examples from the Technological Heritage Operations and Preserved Railways of Britain. Dr Dominic Fontana Department of Geography, University of Portsmouth, United Kingdom [email protected] The railways of Portugal are well known to a global community of steam enthusiasts, many of whom used to visit the country specifically to experience and photograph the last days of steam traction until as late as the 1980s. The narrow gauge lines north of the Douro River, and the Tua Valley line in particular, were considered as very special railways. Their outstanding combination of narrow gauge steam traction, relatively long runs of track and extraordinarily beautiful landscapes, made for a magical railway experience. In the 1980s steam was replaced with diesel traction and although there are now regular but infrequent steam hauled tourist trains on the Douro Valley line, there are currently very limited opportunities for people to recapture this experience. Portugal has several railway museums including the excellent National Railway Museum in Entroncamento, but these present static displays rather than “live” steam and many railway enthusiasts consider this to be a poor substitute for the “real” thing where steam locomotives are operating in steam, within a fully-fledged railway environment. 0189 2-8-4T Henschel 1925 Mallet locomotive at Regua. 1 Portugal possesses over 100 redundant steam locomotives (Bailey, 2013) dispersed in yards around its national railway network, some of them remain potentially usable and many are certainly restorable to full operating condition. Portugal also possesses track and routes, which have been recently closed to passenger and freight traffic. -

SOUTH WEST ENGLAND Frequently Asked Questions
SOUTH WEST ENGLAND Frequently Asked Questions Product Information & Key Contacts 2016 Frequently Asked Questions Bath Bath Visitor Information Centre Abbey Chambers Abbey Churchyard Bath BA1 1LY Key contact: Katie Sandercock Telephone: 01225 322 448 Email: [email protected] Website: www.visitbath.co.uk Lead product Nourished by natural hot springs, Bath is a UNESCO World Heritage city with stunning architecture, great shopping and iconic attractions. Rich in Roman and Georgian heritage, the city has been attracting visitors with its obvious charms for well over 2000 years and is now the leading Spa destination of the UK. Some of the highlights of the city include: The Roman Baths - constructed around 70 AD as a grand bathing and socialising complex. It is now one of the best preserved Roman remains in the world. Thermae Bath Spa – bathe in Bath’s natural thermal waters. Highlights include the indoor Minerva Bath, steam rooms, and an open-air rooftop pool with amazing views over the city. A fantastic range of treatments including massage, facials and water treatments can be booked in advance. Gainsborough Bath Spa Hotel – Britain’s first natural thermal spa hotel. Opened in July 2015. A five-star luxury hotel located in the centre of Bath. Facilities include 99 bedrooms (some with access to Bath’s spring water in their own bathrooms), The Spa Village Bath and Johan Lafer’s ‘Dining Without Borders’ restaurant. Bath Abbey - Magnificent stained glass windows, columns of honey-gold stone and some of the finest fan vaulting in the world, create an extraordinary experience of light and space. -
Inquiry Into the Priorities for the Future of Welsh Rail Infrastructure
Cynulliad Cenedlaethol Cymru National Assembly for Wales Y Pwyllgor Menter a Busnes Enterprise and Business Committee Ymchwiliad i’r Blaenoriaethau ar gyfer Inquiry into the Priorities for the future dyfodol Seilwaith y Rheilffyrdd yng of Welsh Rail Infrastructure Nghymru WRI 11 WRI 11 Cyngor Sir Swydd Gaerloyw Gloucestershire County Council Strategic Planning Shire Hall Gloucester GL1 2TH [email protected] Dear Sir/Madam National Assembly for Wales - Inquiry into the Priorities for the future of Welsh Rail Infrastructure I have been made aware of the above Inquiry. On behalf of Gloucestershire County Council (GCC) I have the following officer comments to make. GCC’s main interest is the Maesteg/Cardiff to Gloucester/Cheltenham service operated by Arriva Trains Wales (ATW) and Lydney station also operated by ATW. Lydney is the only main line railway station within the Forest of Dean and as such is an important component of the area’s infrastructure providing sustainable transport options for residents and visitors alike. Lydney has an allocation of approximately 1900 houses along with additional employment land up to 2026 in their Adopted Core Strategy. Consequently, investment in local rail infrastructure is essential to enable sustainable growth and provide connectivity to the wider area. I have confined my comments to the questions below and they reflect the County’s position as a neighbouring ‘border’ authority. High level priorities for the development of rail infrastructure to provide the capacity and connectivity necessary to support the social and economic well-being of Wales; Response Electrification of the valley lines around Cardiff will improve capacity and connectivity across the city and wider area as well as improving links to other areas of Wales and England including Gloucestershire. -

Light Rail and Tram Statistics, England: 2019/20
Statistical Release 25 June 2020 Light Rail and Tram Statistics, England: 2019/20 About this release Light rail and tram use in England has seen the biggest This statistical release decrease in almost 30 years, down 4.2% in 2019/20. The presents the latest annual information on light rail and number of passenger journeys has fallen below 2016/17 tram systems in England levels. during the 2019/20 fnancial year. The release covers 263.4m light rail and tram use, passenger journeys infrastructure, revenue and passenger experience. Þ 4.2% This publication covers since 2018/19 eight urban systems that are predominantly surface- running (see table 1 for a list There were 263.4 million passengers journeys made on the eight of systems covered). Smaller light rail and tram systems in England, a 4.2% decrease (11.4 million systems, e.g. heritage railway and airport transit systems, passenger journeys) compared with the previous year. Outside are not included. London and London passenger journeys decreased by 4.0% to 119.4 million and Glasgow undergrounds and in London by 4.3% to 144.0 million in the year ending March 2020. Edinburgh Trams are also excluded but statistics for Chart 1: Light rail and tram passenger journeys (millions): these systems are included in England, annually 1983/84 to 2019/20 (table LRT0101) the tables. In this publication 263.4 million Summary fgures 3 Safety 3 Infrastructure 3 Passenger journeys 5 Concessionary journeys 5 Vehicle mileage 6 Revenue 6 Passengers 7 Comment on Coronavirus (COVID-19) impact The period covered by this release includes the frst few weeks of nationwide Passenger satisfaction 8 movement restrictions in March 2020. -
Geomap Leaflet
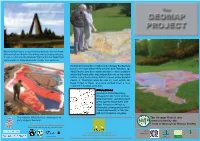
Opposite Geomap is a memorial sculpture to honour those who worked and died in the mining and quarrying industry. It was constructed by Graham Tyler and John Wakefield and consists of three elements: stone, iron and coal. Freeminer Norman Ennis (right) and colleague Ron Baldwin point to the mine where they worked. Over 700 years ago King Edward I gave Dean miners the right to mine anywhere within the Forest after they helped him win an important battle, using their mining skills to tunnel under Berwick Castle. A Freeminer must be over 21, born within the Royal Forest of Dean, and have worked down a local coalmine for a year and a day. Directions Geomap is at the New Fancy Viewpoint in the Forest of Dean, Gloucestershire, two miles south of the Speech House Hotel (see map). Follow the A40 out of Gloucester, picking up the A4136 towards Monmouth, or take the A48 from Chepstow to Lydney The sculptor, David Yeates, working on an The Geomap Project was early stage of Geomap. commissioned by the Forest of Dean Local History Society. This leaflet is funded by the organisations below Our Supported through Defra’s Partners Aggregates Levy Sustainability Fund Geological column What is Geomap? Geomap celebrates both the geological and the The rocks found in the Forest of Dean industrial history of the Forest of Dean. The complex that make up Geomap are shown as a geology of the region, formed over millions of years, geological column, giving their produced the coal and iron deposits that miners have formation and local names, as well as been extracting for at least two thousand years.