Floods 1,955,140
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Preparing for the Possibility of a North Korean Collapse
CHILDREN AND FAMILIES The RAND Corporation is a nonprofit institution that EDUCATION AND THE ARTS helps improve policy and decisionmaking through ENERGY AND ENVIRONMENT research and analysis. HEALTH AND HEALTH CARE This electronic document was made available from INFRASTRUCTURE AND www.rand.org as a public service of the RAND TRANSPORTATION Corporation. INTERNATIONAL AFFAIRS LAW AND BUSINESS NATIONAL SECURITY Skip all front matter: Jump to Page 16 POPULATION AND AGING PUBLIC SAFETY SCIENCE AND TECHNOLOGY Support RAND Purchase this document TERRORISM AND HOMELAND SECURITY Browse Reports & Bookstore Make a charitable contribution For More Information Visit RAND at www.rand.org Explore the RAND National Security Research Division View document details Limited Electronic Distribution Rights This document and trademark(s) contained herein are protected by law as indicated in a notice appearing later in this work. This electronic representation of RAND intellectual property is provided for non-commercial use only. Unauthorized posting of RAND electronic documents to a non-RAND website is prohibited. RAND electronic documents are protected under copyright law. Permission is required from RAND to reproduce, or reuse in another form, any of our research documents for commercial use. For information on reprint and linking permissions, please see RAND Permissions. This report is part of the RAND Corporation research report series. RAND reports present research findings and objective analysis that address the challenges facing the public and private sectors. All RAND reports undergo rigorous peer review to ensure high standards for re- search quality and objectivity. Preparing for the Possibility of a North Korean Collapse Bruce W. Bennett C O R P O R A T I O N NATIONAL SECURITY RESEARCH DIVISION Preparing for the Possibility of a North Korean Collapse Bruce W. -

The Evening Gazette, Indiana, PA Korean War Weekly Front Pages
PMM BLOG ARCHIVE November 17, 2020 70 Years Later, the Korean War, The Evening Gazette, Indiana, PA Korean War Weekly Front Pages The First Week of November 1950 The Evening Gazette, Indiana, PA The Chinese Communists pause. General MacArthur formally notified the UN Security Council that Chinese Communist forces were fighting US troops in Korea. He said, “…the United Nations are presently in hostile contact with Chinese Communist military units deployed for action against the forces of the United command.” A high-ranking Eighth Army staff officer said the Chinese have probably 300,000 troops deployed along the Korean-Manchurian border.The situation in the critical Unsan-Kuna area, north of Pyongyang, appeared stabilized. In the northeast, two US Marine battalions were cut off north of Sudong, while other Marines, driving north toward the Changjin Reservoir, had met strong opposition. Near Majon, a third isolated battalion was reported dug in and in no danger. ROK Capital Division troops and Red Koreans were engaged in bitter street fighting in Kilchu in the northeast. As the week progressed, UN troops were pushing forward on all fronts amid an unexplained Communist withdrawal. A surprise news blackout had been clamped on developments between Communist battle lines and the Chinese border, but the Chinese appeared to be awaiting orders. Sixteen propeller-driven US F-51 Mustang fighters engaged ultramodern Russian-built jet fighters in the longest air battle of the Korean war. American F-80 Shooting Star jets, ordered to the battle over Sinuiju, near the border with China, arrived too late to engage. No American planes were damaged; three of the Mig-15 aircraft were reported hit, and all enemy planes fled across the border after the hour-and-a-half long dogfight. -
Pdf | 431.24 Kb
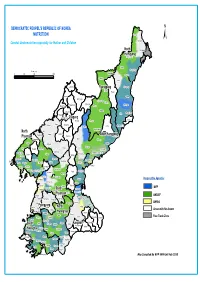
DEMOCRATIC PEOPEL'S REPUBLIC OF KOREA NUTRITION Onsong Kyongwon ± Combat Undernutrition especially for Mother and Children North Kyonghung Hamgyong Hoiryong City Musan Chongjin City Kilometers Taehongdan 050 100 200 Puryong Samjiyon Yonsa Junggang Ryanggang Kyongsong Pochon Paekam Jasong Orang Kimhyongjik Hyesan City Unhung Hwaphyong Kimjongsuk Myonggan Manpo City Samsu Kapsan Janggang Kilju Myongchon Sijung Kanggye City Chagang Rangrim Pungso Hwadae Chosan Wiwon Songgang Pujon Hochon Kimchaek City Kimhyonggwon North Usi Kopung Jonchon South Hamgyong Phyongan Pyokdong Ryongrim Tanchon City Changsong Jangjin Toksong Sakju Songwon Riwon Sinhung Uiju Tongsin Taegwan Tongchang Pukchong Huichon City Sinuiju City Hongwon Sinpho City Chonma Unsan Yonggwang Phihyon Taehung Ryongchon Hyangsan Kusong City Hamhung City Sindo Nyongwon Yomju Tongrim Thaechon Kujang Hamju Sonchon Rakwon Cholsan Nyongbyon Pakchon Tokchon City Kwaksan Jongju City Unjon Jongphyong Kaechon City Yodok Maengsan Anju City Pukchang Mundok Kumya Responsible Agencies Sunchon City Kowon Sukchon Sinyang Sudong WFP Pyongsong City South Chonnae Pyongwon Songchon PhyonganYangdok Munchon City Jungsan UNICEF Wonsan City Taedong Pyongyang City Kangdong Hoichang Anbyon Kangso Sinpyong Popdong UNFPA PyongyangKangnam Thongchon Onchon Junghwa YonsanNorth Kosan Taean Sangwon Areas with No Access Nampo City Hwangju HwanghaeKoksan Hoiyang Suan Pangyo Sepho Free Trade Zone Unchon Yontan Kumgang Kosong Unryul Sariwon City Singye Changdo South Anak Pongsan Sohung Ichon Kangwon Phyonggang Kwail Kimhwa Jaeryong HwanghaeSonghwa Samchon Unpha Phyongsan Sinchon Cholwon Jangyon Rinsan Tosan Ryongyon Sinwon Kumchon Taetan Pongchon Pyoksong Jangphung Haeju City Kaesong City Chongdan Ongjin Paechon Yonan Kaepung Kangryong Map Compiled By WFP VAM Unit Feb 2010. -

UN Consolidated Relief Appeal 2004
In Tribute In 2003 many United Nations, International Organisation, and Non-Governmental Organisation staff members died while helping people in several countries struck by crisis. Scores more were attacked and injured. Aid agency staff members were abducted. Some continue to be held against their will. In recognition of our colleagues’ commitment to humanitarian action and pledging to continue the work we began together We dedicate this year’s appeals to them. FOR ADDITIONAL COPIES, PLEASE CONTACT: UN OFFICE FOR THE COORDINATION OF HUMANITARIAN AFFAIRS PALAIS DES NATIONS 8-14 AVENUE DE LA PAIX CH - 1211 GENEVA, SWITZERLAND TEL.: (41 22) 917.1972 FAX: (41 22) 917.0368 E-MAIL: [email protected] THIS DOCUMENT CAN ALSO BE FOUND ON HTTP://WWW.RELIEFWEB.INT/ UNITED NATIONS New York and Geneva, November 2003 TABLE OF CONTENTS 1. EXECUTIVE SUMMARY ..........................................................................................................................11 Table I. Summary of Requirements – By Appealing Organisation ........................................................12 2. YEAR IN REVIEW ....................................................................................................................................13 2.1 CHANGES IN THE HUMANITARIAN SITUATION ...........................................................................................13 2.2 FINANCIAL OVERVIEW...........................................................................................................................14 2.3 MONITORING REPORT AND -
Searchable PDF Format
- Yangdok Hot Spring Resort - Popular Ceramics Exhibition House - World of Prodigies Silver Ornament A gift presented to President Kim Il Sung by Kaleda Zia, Prime Minister of the People’s Republic of Bangladesh in April 1992 Monthly Journal (766) C O N T E N T S 3 Yangdok Hot Spring Resort 10 Korean Nation’s History of Using Hot Spring 11 Architecture for the People 12 Fruit of Enthusiasm 13 Offensive for Frontal Breakthrough and Increased Production and Economy 14 Old Home at Mangyongdae 17 The Secret Camp on Mt. Paektu 21 Understanding of the People Monthly journal Korea Today is posted on the Internet site www.korean-books.com.kp in English, Russian and Chinese. 1 22 Seventy-fi ve Years of WPK (4) Revolutionary Martyrs Cemetery Tells 23 Relying on Domestic Resources 24 Consumer Changes to Producer 26 Popular Ceramics Exhibition House 28 Nano Cloth Developers Front Cover: Yangdok 29 Target of Developers Hot Spring Resort in the morning 30 World of Prodigies Photo by Kim Kum Sok 32 Record-breaking Achievement in 2019 36 True story I’ll Remain a Winner (7) 38 Promising Sheep Breeding Base 40 Pioneer of Complex Hand-foot Refl ex Therapy 41 Disabled Table Tennis Player 42 National Dog under Good Care 43 Story of Headmaster 44 Glimpse of Japan’s Plunder of Korean Cultural Heritage Back Cover: Moran Hill in spring 46 National Intangible Cultural Heritage (41) Photo by Kim Ji Ye Sijungho Mud Therapy 47 Poetess Ho Ran Sol Hon 13502 ㄱ – 208057 48 Mt Kuwol (3) Edited by Kim Myong Hak Address: Sochon-dong, Sosong District, Pyongyang, DPRK E-mail: fl [email protected] © The Foreign Language Magazines 2020 2 YYangdokangdok HHotot SSpringpring RResortesort No. -

Pdf | 400.65 Kb
InterAction Member Activity Report North Korea A Guide to Humanitarian and Development Efforts of InterAction Member Agencies in North Korea September 2002 Photo by Tom Garofalo, courtesy of Catholic Relief Services Produced by Emily Fugate With the Disaster Response Unit of 1717 Massachusetts Ave., NW, Suite 701, Washington DC 20036 Phone (202) 667-8227 Fax (202) 667-8236 Website: http://www.interaction.org Table of Contents Map of North Korea 2 Background Summary 3 Report Summary 5 Organizations by Sector Activity 6 Glossary of Acronyms 7 InterAction Member Activity Report American Friends Service Committee 8 AmeriCares Foundation 10 Baptist World Aid 12 Catholic Relief Services 13 Christian Reformed World Relief Committee 15 Church World Service 17 Concern Worldwide 19 Heifer International 21 Holt International Children’s Services 22 International Aid 23 Korean American Sharing Movement 24 Lutheran World Relief 26 Mercy Corps 28 US Fund for UNICEF 30 World Vision 32 InterAction Member Activity Report for North Korea 1 September 2002 Map of North Korea Map courtesy of Central Intelligence Agency / World Fact Book InterAction Member Activity Report for North Korea 2 September 2002 Background Summary Over the past decade, the Democratic People’s Republic of Korea (DPRK) has endured a string of natural disasters that have contributed to a prolonged famine that has already claimed an estimated two million lives. Severe flooding and drought have damaged much of the limited agricultural land, leaving only 14 percent arable and the country’s 22 million inhabitants heavily dependent on international food aid. An economic decline since the end of the Cold War, largely the result of misguided policy but coupled with the collapse of assistance from former East-Bloc nations and the former Soviet Union, has further exacerbated the food insecurity in the DPRK. -

WATER SUPPLY and HABITAT PROJECTS in the DPRK ICRC Mission in the Democratic People’S Republic of Korea
PROJECT BRIEF WATER SUPPLY AND HABITAT PROJECTS IN THE DPRK ICRC Mission in the Democratic People’s Republic of Korea PROGRAMME OVERVIEW Since 2013, the International Committee of the Red Cross (ICRC) has been working on water supply in peri-urban areas. Launched in different years, the four ongo- ing projects mainly involve construction with locally available materials and are in different phases of completion. Once finished, they will benefit about 123,750 inhabitants, ensuring they have sustainable access to clean water. Renovations at two local hospitals and two Physical Rehabilitation Centres will enable the public facilities to run more effectively and provide people with up-to-standard infra- structure and services. The Ministry of Urban Management PARTNERS The Democratic People’s Republic of Korea (DPRK) Red Cross Society The International Committee of the Red Cross Water supply to peri-urban communities Jongpyong Eup Town water-supply system Kaechon City water-supply system Location Jongpyong, South Hamgyong Province Location Kaechon, South Pyongan Province Population targeted 43,000 Population targeted 59,200 Starting year 2018 Starting year 2019 Completion May 2020 Completion May 2020 Constructed in the 1970s, the existing water-supply system is Kaechon relies on a pumped water-supply system set up in unable to cover the current needs due to an increase in popu- the 1970s. Over the years, the quality of source well has wors- lation and reduction and deterioration of the water source. ened with the pumps too old to function fully, electricity for Households receive water in shifts and residents without piped pumping has been limited and distribution pipes are broken water in their houses draw it from hand-dug wells, which are and have developed leaks. -

25 Interagency Map Pmedequipment.Mxd
Onsong Kyongwon North Kyonghung Hamgyong Hoiryong City Provision of Medical Equipment Musan Chongjin City Taehongdan Puryong Samjiyon Yonsa Junggang Ryanggang Kyongsong Pochon Paekam Jasong Orang Kimhyongjik Hyesan City Unhung Hwaphyong Kimjongsuk Myonggan Manpo City Samsu Kapsan Janggang Kilju Myongchon Sijung Chagang Kanggye City Rangrim Pungso Hwadae Chosan Wiwon Songgang Pujon Hochon Kimchaek City Kimhyonggwon North Usi Responsible Agency Kopung Jonchon South Hamgyong Phyongan Pyokdong Ryongrim Tanchon City Changsong Jangjin Toksong Sakju Songwon Riwon WHO Sinhung Uiju Tongsin Taegwan Tongchang Pukchong Huichon City Sinuiju City Hongwon Sinpho City UNFPA Chonma Unsan Yonggwang Phihyon Taehung Ryongchon Hyangsan Kusong City Hamhung City Sindo Nyongwon UNICEF Yomju Tongrim Thaechon Kujang Hamju Sonchon Rakwon Cholsan Nyongbyon IFRC Pakchon Tokchon City Kwaksan Jongju City Unjon Jongphyong Kaechon City Yodok Maengsan EUPS 1 Anju City Pukchang Mundok Kumya Sunchon City Kowon EUPS 3 Sukchon SouthSinyang Sudong Pyongsong City Chonnae Pyongwon Songchon EUPS 7 PhyonganYangdok Munchon City Jungsan Wonsan City Taedong Pyongyang City Kangdong Hoichang Anbyon Free Trade Zone Kangso Sinpyong Popdong PyongyangKangnam North Thongchon Onchon Junghwa Yonsan Kosan Taean Sangwon No Access Allowed Nampo City Hwanghae Hwangju Koksan Hoiyang Suan Pangyo Sepho Unchon Yontan Kumgang Kosong Unryul Sariwon City South Singye Kangwon Changdo Anak Pongsan Sohung Ichon Phyonggang Kwail Kimhwa Hwanghae Jaeryong Songhwa Samchon Unpha Phyongsan Sinchon Cholwon Jangyon Rinsan Tosan Ryongyon Sinwon Kumchon Taetan Pongchon Pyoksong Jangphung Haeju City Kaesong City Chongdan Ongjin Paechon Yonan Kaepung Map compliled by VAM Unit Kangryong WFP DPRK Feb 2010. -

Dpr Korea 2019 Needs and Priorities
DPR KOREA 2019 NEEDS AND PRIORITIES MARCH 2019 Credit: OCHA/Anthony Burke Democratic People’s Republic of Korea targeted beneficiaries by sector () Food Security Agriculture Health Nutrition WASH 327,000 97,000 CHINA Chongjin 120,000 North ! Hamgyong ! Hyeson 379,000 Ryanggang ! Kanggye 344,000 Jagang South Hamgyong ! Sinuiju 492,000 North Pyongan Hamhung ! South Pyongan 431,000 ! PYONGYANG Wonsan ! Nampo Nampo ! Kangwon North Hwanghae 123,000 274,000 South Hwanghae ! Haeju 559,000 REPUBLIC OF 548,000 KOREA PART I: TOTAL POPULATION PEOPLE IN NEED PEOPLE TARGETED 25M 10.9M 3.8M REQUIREMENTS (US$) # HUMANITARIAN PARTNERS 120M 12 Democratic People’s Republic of Korea targeted beneficiaries by sector () Food Security Agriculture Health Nutrition WASH 327,000 97,000 CHINA Chongjin 120,000 North ! Hamgyong ! Hyeson 379,000 Ryanggang ! Kanggye 344,000 Jagang South Hamgyong ! Sinuiju 492,000 North Pyongan Hamhung ! South Pyongan 431,000 ! PYONGYANG Wonsan ! Nampo Nampo ! Kangwon North Hwanghae 123,000 274,000 South Hwanghae ! Haeju 559,000 REPUBLIC OF 548,000 KOREA 1 PART I: TABLE OF CONTENTS PART I: COUNTRY STRATEGY Foreword by the UN Resident Coordinator 03 Needs and priorities at a glance 04 Overview of the situation 05 2018 key achievements 12 Strategic objectives 14 Response strategy 15 Operational capacity 18 Humanitarian access and monitoring 20 Summary of needs, targets and requirements 23 PART II: NEEDS AND PRIORITIES BY SECTOR Food Security & Agriculture 25 Nutrition 26 Water, Sanitation and Hygiene (WASH) 27 Health 28 Guide to giving 29 PART III: ANNEXES Participating organizations & funding requirements 31 Activities by sector 32 People targeted by province 35 People targeted by sector 36 2 PART I: FOREWORD BY THE UN RESIDENT COORDINATOR FOREWORD BY THE UN RESIDENT COORDINATOR In the almost four years that I have been in DPR Korea Despite these challenges, I have also seen progress being made. -

DPRK) So Far This Year
DEMOCRATIC PEOPLE’S 16 April 2004 REPUBLIC OF KOREA Appeal No. 01.68/2004 Appeal Target: CHF 14, 278, 310 Programme Update No. 01 Period covered: January – March 2004 The Federation’s mission is to improve the lives of vulnerable people by mobilising the power of humanity. It is the world’s largest humanitarian organisation and its millions of volunteers are active in over 180 countries. For more information: www.ifrc.org In Brief Appeal coverage: 36.3 %; See attached Contributions List for details. Outstanding needs: CHF 9,089,504 Related Emergency or Annual Appeals: 01.67/2003 Programme Summary: No major natural disasters have affected the People’s Democratic Republic of Korea (DPRK) so far this year. Food security is a major concern, especially in areas remote from the capital. The Red Cross Society of the Democratic People’s Republic of Korea (DPRK RC) has been granted permission from the government to expand the Federation supported health and care programme to another province, increasing the number of potential beneficiaries covered by the essential medicines programme to 8.8 million from July 2004. Due to delayed funding, the first quarter of 2004 has been used to finalise most of the programme activities from the 2003 appeal. Bilateral support from the Republic of Korea, the Netherlands and the Norwegian Red Cross Societies is supplementing Federation support. Partner national societies renewed their commitment to continue supporting DPRK RC. DPRK RC is regarded as an important organisation in DPRK by the government, donor country embassies, UN agencies and NGOs. Operational developments Harvests last year in DPRK were above average, however, the UN Food and Agriculture Organisation (FAO) and the World Food Programme (WFP) state that, despite the good harvests, the situation remains “especially precarious” for young children, pregnant and nursing women and many elderly people. -

North Korean Political Prison Camps Starts with the So-Called “August Faction Incident” in 1956
North Korean Prison Camps Radio Free Asia Radio Free Asia Copyright: 2016 by Radio Free Asia . Table Of Contents Chapter 1 Prison Camps from Hell ..................................................................................................................... 2 1) What are Political Prison Camps? ........................................................................................................... 2 2) Testimonies of Former Prisoners ............................................................................................................. 2 3) North Korea Keeps its Political Prison Camps Secret ............................................................................ 3 4) Names Used by North Korea to Disguise the Camps ............................................................................ 4 5) The Intensity of Labor and the Guilt-By-Association System .............................................................. 4 Chapter 2 What is My Crime? ............................................................................................................................ 6 1) Total Control Zones and Revolutionizing Zones .................................................................................. 6 2) Nine Years of Imprisonment as No.1 Criminal ..................................................................................... 6 3) Christians All Go to Prison Camps ......................................................................................................... 8 4) Preposterous Espionage Charges and Passed-Down -
Korea-Today-2021-0306.Pdf
Monthly Journal (777) C O N T E N T S 2 Second Plenary Meeting of Eighth Central Committee of WPK Held 12 Kim Jong Un Sees Lunar New Year’s Day Performance with Party Central Leadership Body Members 14 Appeal to All Working People Across the Country 15 By Dint of Scientifi c Self-reliance 16 Harnessing of Renewable Energy Propelled 17 Electric Power Management Gets Upgraded 18 By Tapping Local Materials 19 Secret of Increasing Production 20 Ideals for New Victory 21 Guidance for the People’s Well-being Monthly journal Korea Today is available on the Internet site www.korean-books.com.kp in English, Russian and Chinese. 22 Education Highlighted in DPRK 23 Immortal Juche Idea (10) Self-reliance in National Defence 24 Pride of Medical Scientist 24 Authority on Burns Treatment 26 With Sincerity and Devotion 28 True story Front Cover: On March Life and Promise 8 International Women’s Day 30 Vinalon Inventor and His Descendants Photo by courtesy 32 E-commerce Gets Expansive of the KCNA 33 Efforts for Correct and Prompt Weather Forecast 34 How Mun Has Overcome Disability 35 Liquefi ed Rare Earth Draws Attention 36 Small Institute in Woods 37 People Who Strive to Increase Forest Land 38 Songchon County Changes 40 Pacesetter of Costume Culture 41 For Conservation of Water Resources 42 Kimchi, Distinctive Dish of Korea (1) Kimchi and Folklore of Korea 44 Mt Chilbo ( 2 ) Back Cover: Rhododen- 46 National Intangible Cultural Heritage (51) dron blossoms in the snow Ssolmaethagi Photo by Song Tae Hyok 47 Ho Jun and Tonguibogam 48 History Denounces 13502 Edited by An Su Yong Address: Sochon-dong, Sosong District, Pyongyang, DPRK E-mail: fl [email protected] © The Foreign Language Magazines 2021 1 ► amine the plans for this year in detail and fi x and work for implementing the decisions made at the issue them as the decisions of the Party Central Party congress starts and what kind of change is Committee.