Coinfection and Tick-Bite Prevention
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Larval Tick Infestation: a Case Report and Review of Tick-Borne Disease
CONTINUING MEDICAL EDUCATION Larval Tick Infestation: A Case Report and Review of Tick-Borne Disease Emily A. Fibeger, DO; Quenby L. Erickson, DO; Benjamin D. Weintraub, MD; Dirk M. Elston, MD GOAL To understand larval tick infestation to better manage patients with the condition OBJECTIVES Upon completion of this activity, dermatologists and general practitioners should be able to: 1. Recognize the clinical presentation of larval tick infestation. 2. Manage and understand patients exposed to tick-borne disease. 3. Prevent tick-borne disease within the general population. CME Test on page 47. This article has been peer reviewed and approved Einstein College of Medicine is accredited by by Michael Fisher, MD, Professor of Medicine, the ACCME to provide continuing medical edu- Albert Einstein College of Medicine. Review date: cation for physicians. June 2008. Albert Einstein College of Medicine designates This activity has been planned and imple- this educational activity for a maximum of 1 AMA mented in accordance with the Essential Areas PRA Category 1 CreditTM. Physicians should only and Policies of the Accreditation Council for claim credit commensurate with the extent of their Continuing Medical Education through the participation in the activity. joint sponsorship of Albert Einstein College of This activity has been planned and produced in Medicine and Quadrant HealthCom, Inc. Albert accordance with ACCME Essentials. Drs. Fibeger, Erickson, Weintraub, and Elston report no conflict of interest. The authors report no discussion of off-label use. Dr. Fisher reports no conflict of interest. Tick-borne disease in the United States contin- disease, Rocky Mountain spotted fever (RMSF), ues to be a threat as people interact with their ehrlichiosis, babesiosis, tularemia, tick-borne natural surroundings. -

An Epidemiological Survey Regarding Ticks and Tick-Borne Diseases Among Livestock Owners in Punjab, Pakistan: a One Health Context
pathogens Article An Epidemiological Survey Regarding Ticks and Tick-Borne Diseases among Livestock Owners in Punjab, Pakistan: A One Health Context Sabir Hussain 1,* , Abrar Hussain 2 , Jeffery Ho 1, Jun Li 1,3, David George 4, Abdul Rehman 2 , Jehan Zeb 5 and Olivier Sparagano 1,* 1 Department of Infectious Diseases and Public Health, Jockey Club College of Veterinary Medicine and Life Sciences, City University of Hong Kong, Kowloon, Hong Kong, China; [email protected] (J.H.); [email protected] (J.L.) 2 Department of Epidemiology and Public Health, University of Veterinary and Animal Sciences, Lahore 54600, Pakistan; [email protected] (A.H.); [email protected] (A.R.) 3 School of Data Science, City University of Hong Kong, Kowloon, Hong Kong, China 4 School of Natural and Environmental Sciences, Agriculture Building, Newcastle University, Newcastle upon Tyne NE1 7RU, UK; [email protected] 5 Department of Zoology, Abdul Wali Khan University Mardan, Mardan 23200, Pakistan; [email protected] * Correspondence: [email protected] (S.H.); [email protected] (O.S.) Abstract: Recent global changes have led to an increase in the spread of ticks and tick-borne diseases (TBDs) affecting domestic ruminants and humans, with an annual loss of US $13.9–$18.7 billion. The Citation: Hussain, S.; Hussain, A.; current study determined the perception and practices of livestock farmers regarding tick infestation. Ho, J.; Li, J.; George, D.; Rehman, A.; A total of 112 livestock farms were surveyed in Punjab, Pakistan, among which animals from 42 Zeb, J.; Sparagano, O. -

Ixodes Ricinus Salivary Serpin Iripin-8 Inhibits the Intrinsic Pathway of Coagulation and Complement
International Journal of Molecular Sciences Article Ixodes ricinus Salivary Serpin Iripin-8 Inhibits the Intrinsic Pathway of Coagulation and Complement Jan Kotál 1,2 , Stéphanie G. I. Polderdijk 3 , Helena Langhansová 1, Monika Ederová 1, Larissa A. Martins 2 , Zuzana Beránková 1, Adéla Chlastáková 1 , OndˇrejHajdušek 4, Michail Kotsyfakis 1,2 , James A. Huntington 3 and JindˇrichChmelaˇr 1,* 1 Department of Medical Biology, Faculty of Science, University of South Bohemia in Ceskˇ é Budˇejovice, Branišovská 1760c, 37005 Ceskˇ é Budˇejovice,Czech Republic; [email protected] (J.K.); [email protected] (H.L.); [email protected] (M.E.); [email protected] (Z.B.); [email protected] (A.C.); [email protected] (M.K.) 2 Laboratory of Genomics and Proteomics of Disease Vectors, Institute of Parasitology, Biology Center CAS, Branišovská 1160/31, 37005 Ceskˇ é Budˇejovice,Czech Republic; [email protected] 3 Cambridge Institute for Medical Research, Department of Haematology, University of Cambridge, The Keith Peters Building, Hills Road, Cambridge CB2 0XY, UK; [email protected] (S.G.I.P.); [email protected] (J.A.H.) 4 Laboratory of Vector Immunology, Institute of Parasitology, Biology Center CAS, Branišovská 1160/31, 37005 Ceskˇ é Budˇejovice,Czech Republic; [email protected] * Correspondence: [email protected] Abstract: Tick saliva is a rich source of antihemostatic, anti-inflammatory, and immunomodulatory molecules that actively help the tick to finish its blood meal. Moreover, these molecules facilitate the Citation: Kotál, J.; Polderdijk, S.G.I.; transmission of tick-borne pathogens. Here we present the functional and structural characterization Langhansová, H.; Ederová, M.; of Iripin-8, a salivary serpin from the tick Ixodes ricinus, a European vector of tick-borne encephalitis Martins, L.A.; Beránková, Z.; and Lyme disease. -

Severe Babesiosis Caused by Babesia Divergens in a Host with Intact Spleen, Russia, 2018 T ⁎ Irina V
Ticks and Tick-borne Diseases 10 (2019) 101262 Contents lists available at ScienceDirect Ticks and Tick-borne Diseases journal homepage: www.elsevier.com/locate/ttbdis Severe babesiosis caused by Babesia divergens in a host with intact spleen, Russia, 2018 T ⁎ Irina V. Kukinaa, Olga P. Zelyaa, , Tatiana M. Guzeevaa, Ludmila S. Karanb, Irina A. Perkovskayac, Nina I. Tymoshenkod, Marina V. Guzeevad a Sechenov First Moscow State Medical University (Sechenov University), Moscow, Russian Federation b Central Research Institute of Epidemiology, Moscow, Russian Federation c Infectious Clinical Hospital №2 of the Moscow Department of Health, Moscow, Russian Federation d Centre for Hygiene and Epidemiology in Moscow, Moscow, Russian Federation ARTICLE INFO ABSTRACT Keywords: We report a case of severe babesiosis caused by the bovine pathogen Babesia divergens with the development of Protozoan parasites multisystem failure in a splenic host. Immunosuppression other than splenectomy can also predispose people to Babesia divergens B. divergens. There was heavy multiple invasion of up to 14 parasites inside the erythrocyte, which had not been Ixodes ricinus previously observed even in asplenic hosts. The piroplasm 18S rRNA sequence from our patient was identical B. Tick-borne disease divergens EU lineage with identity 99.5–100%. Human babesiosis 1. Introduction Leucocyte left shift with immature neutrophils, signs of dysery- thropoiesis, anisocytosis, and poikilocytosis were seen on the peripheral Babesia divergens, a protozoan blood parasite (Apicomplexa: smear. Numerous intra-erythrocytic parasites were found, which were Babesiidae) is primarily specific to bovines. This parasite is widespread initially falsely identified as Plasmodium falciparum. The patient was throughout Europe within the vector Ixodes ricinus. -

PREVENTION of TICK-BORNE DISEASE Contrary to Popular Belief, Ticks Do Not Jump, Fly Or Fall out of Trees. They Wait on Low Growi
PREVENTION OF TICK-BORNE DISEASE LYME DISEASE Symptoms and Treatment Contrary to popular belief, ticks do not jump, fly or fall out Lyme disease is caused Symptoms of Lyme disease may appear between three days of trees. They wait on low growing plants for a host to pass by bacteria called Borrelia to a few weeks after a tick bite. Most, but not all infected by. When a person or animal brushes against the vegetation, burgdorferi. In Ohio, the bacteria people develop a circular, ring-like rash called erythema the tick will cling to fur or clothing and crawl upward, are transmitted to humans by migrans. Other early symptoms include fever, fatigue, looking for a place to attach and begin feeding. The risk of the deer tick, Ixodes scapularis. headache and joint pain. Some symptoms of Lyme disease exposure to ticks and disease can be reduced by following Not all ticks are infected and an may not appear until weeks, months or years after a tick these precautions: infected tick is usually attached bite, affecting joints, nervous system and heart. Diagnosis to the host for 36 to 48 hours of Lyme disease is based on history of tick exposure, signs Humans before it transmits disease. This and symptoms and is aided by the use of blood tests. Lyme Avoid tick-infested areas such as tall grass and dense disease is usually transmitted disease responds to appropriate antibiotic therapy. Early • Ixodes scapularis, female vegetation. Dermacentor variabilis female (left) and male (right) in the spring and summer by detection and treatment will reduce the risk of arthritis and juvenile ticks, which are about the size of a pinhead, and in other complications. -

Infection of Dogs with Babesia Canis in Gwagwalada Metropolis of Federal Capital Territory, Abuja, Nigeria OC Jegede*, SS Obeta & B Faisal
Sokoto Journal of Veterinary Sciences, Volume 12 (Number 3). December, 2014 RESEARCH ARTICLE Sokoto Journal of Veterinary Sciences (P-ISSN 1595-093X/ E-ISSN 2315-6201) Jegede et al/Sokoto Journal of Veterinary Sciences (2014) 12(3): 37-41 http://dx.doi.org/10.4314/sokjvs.v12i3.7 Infection of dogs with Babesia canis in Gwagwalada metropolis of Federal Capital Territory, Abuja, Nigeria OC Jegede*, SS Obeta & B Faisal Department of Parasitology and Entomology, Faculty of Veterinary Medicine, University of Abuja *Correspondence: Tel.: +2348037023920, E-mail: [email protected] Abstract Epidemiological investigation was carried out to determine the prevalence of infection with Babesia canis in dogs in Gwagwalada metropolis of the Federal Capital Territory, Abuja Nigeria, from November 2013 to January 2014. Blood samples were collected from 101 dogs and examined for the parasite. Data obtained were analyzed to determine the prevalence of Babesia canis and the correlation of infection with age, sex, breed, types of management and presence or absence of tick infestation on the animal. Dogs screened were those from randomly selected house holds within the area. Overall results show an infection rate of 9/101 (8.9%). The prevalence was higher (P <0.05) among adults than puppies and also higher (P<0.05) among dogs with tick infestation than those without. Keywords: Babesia, Canine, Epidemiology, Gwagwalada, Prevalence Received: 17-04-2014 Accepted: 30-10-2014 Introduction Babesiosis, a tick-borne protozoan disease of America and North and East Africa (Taboada, 1998). animals caused by the parasite of the genus Babesia The common brown dog tick, R. -

Client Handout: 7 Myths About Lyme Disease
Client handout: 7 myths about Lyme disease Consider this list of common myths about Lyme disease and learn the facts to protect your pet: Myth 1: I don’t live in a ease. While you may diligent about wooded area, so my pet checking for and removing ticks, it can’t get ticks. still only takes one tick bite for a pet thaws during winter may release these Even if you think your pets don’t to contract Lyme disease. When you frozen ticks for another blood meal. visit areas where ticks are com- find ticks on your pet, there’s a good For the best protection, continuously monly found, such as wooded areas chance the pet has had other ticks apply preventives throughout the and places with high grass or brush, you’ve missed. And even if you only year, including the colder months. remember that ticks are actually find one tick, your veterinary team able to live out their entire life cycle wants to protect the pet’s well-being Myth 6: My pet was within your home. Woodpiles near by testing for tick-borne diseases in treated for Lyme disease, or inside a home provide the perfect the months following the bite. so now she’s cured. environment for ticks to survive. Once a pet is diagnosed with Lyme And when your pets are inside, this Myth 4: I apply a flea and disease, the doctor usually prescribes improves the environment for a tick’s tick preventive to my pet an antibiotic. Once the antibiotic survival because ticks need readily monthly, so I don’t need course is finished, this doesn’t guar- available hosts. -

Age-Related Tick Infestation Patterns in Springtime Migratory Passerines
The University of Southern Mississippi The Aquila Digital Community Honors Theses Honors College Spring 5-2019 Age-Related Tick Infestation Patterns in Springtime Migratory Passerines Matthew Dunning University of Southern Mississippi Follow this and additional works at: https://aquila.usm.edu/honors_theses Part of the Ecology and Evolutionary Biology Commons Recommended Citation Dunning, Matthew, "Age-Related Tick Infestation Patterns in Springtime Migratory Passerines" (2019). Honors Theses. 657. https://aquila.usm.edu/honors_theses/657 This Honors College Thesis is brought to you for free and open access by the Honors College at The Aquila Digital Community. It has been accepted for inclusion in Honors Theses by an authorized administrator of The Aquila Digital Community. For more information, please contact [email protected]. The University of Southern Mississippi Age-Related Tick Infestation Patterns in Springtime Migratory Passerines by Matthew Dunning A Thesis Submitted to the Honors College of The University of Southern Mississippi in Partial Fulfillment of Honors Requirements May 2019 ii Approved by: ________________________________ Michael Sellers, Thesis Adviser Instructor of Biological Sciences ________________________________ Frank R. Moore, Ph.D., Thesis Adviser Professor Emeritus of Biological Sciences _______________________________ Jake Schaefer, Ph.D., Director School of Biological, Environmental, and Earth Sciences _______________________________ Ellen Weinauer, Ph.D., Dean Honors College iii Abstract To test the hypothesis that younger migrants are more prone to arrive at stopover sites on the northern coast of the Gulf of Mexico with ticks than adult migrants, 2177 migratory passerines were screened for ticks at Gulf Coast sites in Texas and Louisiana. Fifty eight (2.7%) were infested with ticks with 28 (1.3%) being young birds and 30 (1.4%) being adult birds. -

Tularemia in the Wildlife of Arkansas Leo J
Journal of the Arkansas Academy of Science Volume 21 Article 11 1967 Tularemia in the Wildlife of Arkansas Leo J. Paulissen University of Arkansas, Fayetteville E. Reece Corey University of Arkansas, Fayetteville Delbert Swartz University of Arkansas, Fayetteville Follow this and additional works at: http://scholarworks.uark.edu/jaas Part of the Animal Diseases Commons Recommended Citation Paulissen, Leo J.; Corey, E. Reece; and Swartz, Delbert (1967) "Tularemia in the Wildlife of Arkansas," Journal of the Arkansas Academy of Science: Vol. 21 , Article 11. Available at: http://scholarworks.uark.edu/jaas/vol21/iss1/11 This article is available for use under the Creative Commons license: Attribution-NoDerivatives 4.0 International (CC BY-ND 4.0). Users are able to read, download, copy, print, distribute, search, link to the full texts of these articles, or use them for any other lawful purpose, without asking prior permission from the publisher or the author. This Article is brought to you for free and open access by ScholarWorks@UARK. It has been accepted for inclusion in Journal of the Arkansas Academy of Science by an authorized editor of ScholarWorks@UARK. For more information, please contact [email protected], [email protected]. Journal of the Arkansas Academy of Science, Vol. 21 [1967], Art. 11 39 Arkansas Academy of Science Proceedings, Vol.21, 1967 TULAREMIA IN THE WILDLIFE OF ARKANSAS Leo J. Paulissen, R. Reece Corey* and Delbert Swartz** University of Arkansas, Fayetteville INTRODUCTION Tularemia is generally considered to be a disease of rabbits and hares from which, through handling, humans contract the infection. This consideration has been fostered by reports, such as by Francis (11), and by particular statistics, such as for Illinois (17), which implicate rabbits • in well over 90% of human infections. -

Sokoto Journal of Veterinary Sciences Prevalence of Ticks on Indigenous
Sokoto Journal of Veterinary Sciences, Volume 16 (Number 3). September, 2018 RESEARCH ARTICLE Sokoto Journal of Veterinary Sciences (P-ISSN 1595-093X: E-ISSN 2315-6201) http://dx.doi.org/10.4314/sokjvs.v16i3.10 Akande et al./Sokoto Journal of Veterinary Sciences, 16(3): 66-71. Prevalence of ticks on indigenous breed of hunting dogs in Ogun State, Nigeria FA Akande1*, AF Adebowale1, OA Idowu1 & OO Sofela2 1. Department of Veterinary Microbiology and Parasitology, College of Veterinary Medicine, Federal University of Agriculture, PMB 224, Abeokuta, Ogun State, Nigeria 2. Department of Veterinary Medicine, Faculty of Veterinary Medicine, University of Ibadan, Oyo State, Nigeria *Correspondence: Tel.: +2348035008607; E-mail: [email protected] Copyright: © 2018 Abstract Akande et al. This is an Ticks are haematophagous arthropods that are important vectors of diseases of open-access article animals and humans, many of which are zoonotic, thus predisposing humans, published under the including hunters to risk. The present study was conducted to assess the prevalence terms of the Creative of tick infestation among hunting dogs with the aim of determining the danger which Commons Attribution the presence of ticks portends, bearing in mind that hunting dogs are kept by the duo License which permits of rural and urban dwellers. A total of one hundred and nine (109) hunting dogs were unrestricted use, sampled from nineteen (19) different locations in the State. The age, weight and sex distribution, and of the dogs were noted and recorded as variables. The dogs were thoroughly reproduction in any examined for ticks and other ectoparasites which were collected into properly medium, provided the labelled plastic containers and were transported to the laboratory for identification. -

Ticks and Lyme Disease
Ticks and Lyme Disease USDA Forest Service Hoosier National Forest 7/2012 We don't have lions or tigers or bears on on small mammals and are not a problem for the Hoosier National Forest, but we do have humans. ticks. Over the past 20-30 years the number There are over 800 species of ticks. Dif- of ticks on the Hoosier National Forest, espe- ferent species carry different diseases. Rocky cially in the area south of Interstate 64 has Mountain Spotted Fever and Lyme Disease increased dramatically. Along with the in- are two of the better known diseases spread crease in the numbers of ticks, is a growing by ticks. Some diseases, such as Lyme Dis- problem with human diseases which are as- ease may effect pets and livestock as well as sociated with ticks. people. For many people, finding a tick latched onto their leg is enough to put a damper on a Avoiding Ticks trip to the woods. It's like finding a mouse in Ticks are going to congregate where they the cupboard or a roach in your bed sheets, have a high chance of finding a host or where and leaves you feeling unaccountably para- they hatched out as larvae. Any high traffic noid. With recent publicity given to the threat area should be avoided, including cow paths of Lyme disease, people's fears have intensi- in pastures and deer paths in the woods. Also fied and some are actually afraid to visit the avoid tall grass and thick brush. If your pets forest. roam into areas where they are likely to pick up ticks, routinely check them for ticks and Tick Demographics use baths, dips, and flea and tick collars to Weather conditions seem to have the reduce the chances of your pets bringing ticks greatest effect on the density of ticks. -
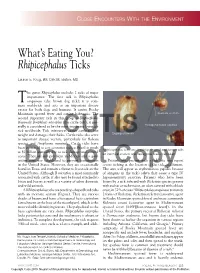
Rhipicephalus Ticks
Close enCounters With the environment What’s Eating You? Rhipicephalus Ticks Lauren E. Krug, BS; Dirk M. Elston, MD he genus Rhipicephalus includes 2 ticks of major importance. The first tick is Rhipicephalus T sanguineus (the brown dog tick); it is com- mon worldwide and acts as an important disease vector for both dogs and humans. It carries Rocky Mountain spotted fever and canine babesiosis. The Inornate scutum second important tick in this group is Rhipicephalus (formerly Boophilus) microplus (the cattle tick); it gen- erally is considered to be the most important livestock Hexagonal basis capitula tick worldwide. Tick infestation causes cattle to lose weight and damages their hides.CUTIS Cattle ticks also serve Engorged female as important disease vectors, particularly for Babesia species and Anaplasma marginale. Cattle ticks have been estimated to cost countries such as Brazil as much Rhipicephalus ticks are teardrop shaped and brown with as $2 billion annually due to tick damage and control an inornate scutum and hexagonal basis capitulum. costs.1 They are still prevalent in Mexico and a quar- antine zone was established to prevent transmission Patients who present with a tick bite may report in theDo United States. However, Not they are occasionally severe itchingCopy at the location of the tick attachment. found in Texas and remain a threat to livestock in the The area will appear as erythematous papules because United States. Although R microplus is most commonly of antigens in the tick’s saliva that cause a type IV associated with cattle, it also may be found attached to hypersensitivity reaction.