How Do You Identify the Patient with 'High Expectations' of Orthodontic
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Strategy 2014-19: Our Vision for the New King's
STRATEGY 2014-19 Our Vision for the new King’s King’s College Hospital, Princess Royal University Orpington Hospital Queen Mary’s Hospital, Beckenham Beacon Denmark Hill Hospital, Farnborough Sidcup Our vision is to become a fundamentally new kind of hospital built around We will be three types of hospitals in one: patient need, offering all our patients – local, national and international – the highest quality of care. • A leading national specialist hospital treating patients from across the country • A major regional emergency centre for London and the south east Working across our sites, and in the community, our care will be kind, innovative and • An extensive multi-site district general hospital for our resident population. It will efficient. Clinical care, research and education at King’s will work hand in hand to provide urgent hospital care joined up with GP services near where people live, and ensure the best services, latest treatments and compassionate care. well-run appointments and operations when people need them. Wherever we work we will be Team King’s, united by our caring culture and our values: Inspiring Making a Understanding Working Always aiming confidence in difference in you together higher our care our community Our background King’s College Hospital NHS Foundation The next five years will see further Trust provides hospital care to patients in change as we follow through our plans for Lambeth, Southwark, Lewisham, Bromley, these new hospitals to improve services and beyond to South East London and for patients in Bromley and Bexley. Kent. Our 11,000 staff see over one and We have a big task to meet increasing a half million patients each year – from needs and improve services with over- routine care for sick children and elderly stretched staff, beds and theatres. -
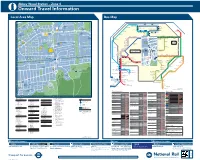
Abbey Wood Station – Zone 4 I Onward Travel Information Local Area Map Bus Map
Abbey Wood Station – Zone 4 i Onward Travel Information Local Area Map Bus Map 45 1 HARTSLOCK DRIVE TICKFORD CLOSE Y 1 GROVEBURY ROAD OAD 16 A ALK 25 River Thames 59 W AMPLEFORTH R AMPLEFORTH ROAD 16 Southmere Central Way S T. K A Crossway R 1 B I N S E Y W STANBROOK ROAD TAVY BRIDGE Linton Mead Primary School Hoveton Road O Village A B B E Y W 12 Footbridge T H E R I N E S N SEACOURT ROAD M E R E R O A D M I C H A E L’ S CLOSE A S T. AY ST. MARTINS CLOSE 1 127 SEWELL ROAD 1 15 Abbey 177 229 401 B11 MOUNTJOYCLOSE M Southmere Wood Park ROAD Steps Pumping GrGroroovoveburyryy RRoaadd Willow Bank Thamesmead Primary School Crossway Station W 1 Town Centre River Thames PANFIE 15 Central Way ANDW Nickelby Close 165 ST. HELENS ROAD CLO 113 O 99 18 Watersmeet Place 51 S ELL D R I V E Bentham Road E GODSTOW ROAD R S O U T H M E R E L D R O A 140 100 Crossway R Gallions Reach Health Centre 1 25 48 Emmanuel Baptist Manordene Road 79 STANBROOK ROAD 111 Abbey Wood A D Surgery 33 Church Bentham Road THAMESMEAD H Lakeside Crossway 165 1 Health Centre Footbridge Hawksmoor School 180 20 Lister Walk Abbey Y GODSTOW ROAD Footbridge N1 Belvedere BUR AY Central Way Wood Park OVE GROVEBURY ROAD Footbridge Y A R N T O N W Y GR ROAD A Industrial Area 242 Footbridge R Grasshaven Way Y A R N T O N W AY N 149 8 T Bentham Road Thamesmead 38 O EYNSHAM DRIVE Games N Southwood Road Bentham Road Crossway Crossway Court 109 W Poplar Place Curlew Close PANFIELD ROAD Limestone A Carlyle Road 73 Pet Aid Centre W O LV E R C O T E R O A D Y 78 7 21 Community 36 Bentham Road -
London Borough of Bexley Local Implementation Plan 2019/20 – 2021/22
www.bexley.gov.uk London Borough of Bexley Local Implementation Plan 2019/20 – 2021/22 May 2019 LB Bexley LIP 2019/20 – 2021/22 Contents London Borough of Bexley Local Implementation Plan ............................................................................................. 2 Foreword ........................................................................................................................................................................... 6 1. Introduction and Preparation of the Draft Local Implementation Plan ..................................................... 7 1.1 Introduction ..................................................................................................................................................... 7 1.2 Local Approval Process ................................................................................................................................. 7 1.3 Statutory Consultation .................................................................................................................................. 8 1.4 Statutory duties ............................................................................................................................................... 9 1.5 LIP approval ..................................................................................................................................................... 9 2. Borough Transport Objectives .......................................................................................................................... -

Bexley Station – Zone 6 I Onward Travel Information Local Area Map Bus Map N
Bexley Station – Zone 6 i Onward Travel Information Local Area Map Bus Map N R D 686 22 1 144 Eighty Oak 200 Footbridge R O C H E S T E R D R I V E E A S O C H E S T E R W T R O E A S T R A Y C H E S T E 20 201 R BASING DRIVE GRAVEL HILL CLOSE GRAVEL HILL CLOSE Hall Place Thamesmead W A D Thamesmead Belvedere U Y 122 A Boiler House /RZHU5RDG P 8 Town Centre T O 12 Ri O N BAYNHAM CLOSE ver West Street 40 S R h ut R Thamesmead O tle 229 Abbey Wood A HARTLANDS CLOSE D Crossway E S B12 O 50 U N T WILLOW CLOSE Hall Place H 15 Erith Town Centre R 1 River Shuttle Gardens y THAMESMEAD U ra 25 C D O r 20 e Erith Health Centre iv 1 A Blackckk PrPPrincence B R FA R M VA L E O ERITH Beths R Interchchahangangenge Grammar 1 FINSBURY WAY 3 229 School D Avenue Road L Parsonage Northumberland O 67 H A R 2 T F Manorway Heath Erith & District Hospital O R 9 W D Holiday Inn R O O TFORD 6KLQJOHZHOO5RDG &DUOWRQ5RDG N E A H D L A D 1 C L O V E 1 33 L O SE T A E 1 1 198 O A Carlton Road +DLO 5LGH L O V E L A N E U R S 52 T section 1 O 13 30 31 E N R S Barnehurst 104 ELMINGTO O 1 E R Bedonwell Road CRAYFORD D S U C A N C L 14 O H O OSE L O Old Road Greenhithe 37 R H C B E L L A Bexleyheath O R N S RIVERDALE ROAD K N T 1 Perry Street Crayford Shepherd’s Lane Dartford Waterstone Park 1 F O O T R D T Old Dartfordians Bus Garage e G E tl ALBERT ROAD R t O N R 15 u A I Association h 14 D S M W Mayplace Road Crayford Chastilian Road Horns Cross D L er A D Riv E A 35 PARKHURST ROAD E A M R O Y East Bull L E L Town Hall T L 2 Pickford Lane T T H E C L O S E O U N BEXLEYHEATH H U K S P T O 1 14 N 132 R O DARTFORD 29 A 98 Mayplace Road West Bluewater Shopping Centre 65 D 20 North Greenwich 48 1 N21 S O Foresters Crescent U E for The O2 492 T H E R I D G E T A N continues to 2 H L Bexleyheath 1 K 132 S C H 267 A Bank , Bexleyheath U T B 132 T L Bexley FC y E M 38 ra Broadway +LJKODQG5RDG E A C St. -

Cray Hall 141 North Cray Road | Sidcup | DA14 5HE CRAY HALL
Cray Hall 141 North Cray Road | Sidcup | DA14 5HE CRAY HALL The Grade II listed Cray Hall is believed to of been built circa 1750 and still retains many of its original charm and features, the property is set in approximately 6 acres including formal gardens, lawn, orchard and paddock and has various outbuildings, including stables for 10 horses with attached paddock and garaging for several cars (circa 10,000sqft with potential for development subject to planning consent). The indoor pool complex offers a 15m x 5m swimming pool, jacuzzi with spiral staircase down to sauna, male and female changing rooms, whilst to the rear of the pool room is a bar area, snooker room and vaulted gymnasium (circa 10,000sq ft). The location could not be better, with Gatwick Airport (35 Mins) Heathrow (60 mins), Biggin Hill (20 mins) Ebbsfleet International (16 mins) and Central London (35 mins) all by car, making this ideal for applicants looking to be in a country setting with the Five Arches across the road and Joydens Wood at the rear while being close to European and Worldwide transport links and of course the Capital. Finally there are outstanding state and private schools in the vicinity – St Olaves, Newstead, Eltham College, Bromley High, Chislehurst and Sidcup Grammar, BETHS Grammar and many others. All in all the perfect location. Back in its heyday the original village of North Cray became almost a private estate for the wealthy. By the beginning of the 18th century large houses with magnificent ornate gardens lined the banks of the River Cray and the surrounding area. -

Cray Riverway Village
How to get there... 9 Turn left down Edgington Lane for 100 metres to a footbridge, cross and turn right to head back to the BUSES: roundabout and turn left into Maidstone Road. Walk on R6 Orpington to St Mary Cray 400 metres to Foots Cray High Street. Cross the road to Wa l k s R4 St Paul’s Cray to Locksbottom the Seven Stars public house c.1753 on the right. In 1814 51 Woolwich to Orpington a red lantern was hung outside this pub to guide travellers around the Borough 61 Chislehusrt to Bromley through the ford and it was once an important staging post for coaches from Maidstone to London. 273 Lewisham to Petts Wood R1 St Pauls Cray to Green Street Green R11 Sidcup to Green Street Green 10 Continue past the Tudor Cottages on the left to the end B14 Bexleyheath to Orpington of the High Street. Turn right into Rectory Lane, the listed R2 Petts Wood to Biggin Hill Georgian Terrace on the left c. 1737 bears the original R3 Locksbottom to Chelsfield road plaques. Continue on to Harenc School c.1815, a clock tower was added to commemorate Queen Victoria’s TRAIN: Jubilee. Nearest station: Orpington CAR: Image © David Griffiths 11 Walk on 300 metres. Ahead is the parish church of All Turn into the High Street, Orpington at the junction with Saints Foots Cray. Originally a wood and thatch building Station Road (A232). Continue north along the High c.900 AD, it was rebuilt in 1330. Take the signposted Street and turn into Church Hill. -
Bexley Growth Strategy
www.bexley.gov.uk Bexley Growth Strategy December 2017 Bexley Growth Strategy December 2017 Leader’s Foreword Following two years of detailed technical work and consultation, I am delighted to present the Bexley Growth Strategy that sets out how we plan to ensure our borough thrives and grows in a sustainable way. For centuries, Bexley riverside has been a place of enterprise and endeavour, from iron working and ship fitting to silk printing, quarrying and heavy engineering. People have come to live and work in the borough for generations, taking advantage of its riverside locations, bustling town and village centres and pleasant neighbourhoods as well as good links to London and Kent, major airports, the Channel rail tunnel and ports. Today Bexley remains a popular place to put down roots and for businesses to start and grow. We have a wealth of quality housing and employment land where large and small businesses alike are investing for the future. We also have a variety of historic buildings, neighbourhoods and open spaces that provide an important link to our proud heritage and are a rich resource. We have great schools and two world-class performing arts colleges plus exciting plans for a new Place and Making Institute in Thamesmead that will transform the skills training for everyone involved in literally building our future. History tells us that change is inevitable and we are ready to respond and adapt to meet new opportunities. London is facing unprecedented growth and Bexley needs to play its part in helping the capital continue to thrive. But we can only do that if we plan carefully and ensure we attract the right kind of quality investment supported by the funding of key infrastructure by central government, the Mayor of London and other public bodies. -
Locally Listed Buildings and Structures in the London Borough of Bexley, of Architectural Or Historic Interest
www.bexley.gov.uk Locally Listed Buildings Locally listed buildings and structures in the London Borough of Bexley, of architectural or historic interest These are shown in street order for ease of reference Locally listed buildings and structures in street order Year of Address Locality Name or descriptive detail entry A 1-12 (cons) Acacia Way Sidcup Former Hollies Children’s Home Boys 2011 Houses: ‘Limes’ and ‘Oaks’ 32 & 33 Acacia Way Sidcup Former Hollies Children’s Home Infant 2011 Boys Home: ‘Willow’ 34 Acacia Way Sidcup Sports Club building 2011 35 & 36 Acacia Way Sidcup Former ‘Hollies’ admin. building. Other 1983 The Manor House flats addressed to Rowanwood Avenue. 38, 39 & 40 Acacia Way Sidcup Stable block of “The Hollies” 2006 53 Acacia Way Sidcup Former Hollies Children’s Home building 2011 - Ash’ 54-73 (cons) Acacia Way Sidcup Former Hollies Children’s Home Boys 2011 Homes: ‘Beeches’ and Firs’ 63 Albert Road Bexley “The Black Horse” 1983 1 & 2 Belvoir Cottages Alma Road Sidcup 2006 10 Alma Road Sidcup “The Alma” 1983 2 Avenue Road Bexleyheath “Turret House” 2006 6 Avenue Road Bexleyheath “Torre” 2006 27 Avenue Road Bexleyheath “Ravensbourne” 2006 109 Avenue Road Erith Lodge 2008 B Chapel Banks Lane Bexleyheath Cemetery Chapel 2006 War memorial Banks Lane Bexleyheath War memorial in cemetery 2006 Maufe memorial Banks Lane Bexleyheath Memorial in cemetery 2011 The Red Barn Barnehurst Road Bexleyheath The Red Barn Public House 2008 3, 5 & 7 Bedford Road Sidcup “Burley Villas” 2006 6 Bedwell Road Belvedere Kearsbrook Lodge 2008 -

Waring Park, Sidcup, Kent
CARNEGIE NPFA PLAYING FIELD: WARING PARK, SIDCUP, KENT Site details The total cost of levelling, fencing and lay-out of the playing field was £1,100. In March 1931 a grant Site Name: Waring Park of £200.00 was made covering 18% of the cost; Size originally: 13 acres £160.00 from the Carnegie UK Trust and £40.00 from Size currently: tbc the National Playing Fields Association. The works Street: Birchwood Avenue were completed in May 1930. The formal opening (Lansdown Road) of Waring Park took place on Saturday 2nd May Town: Sidcup 1931 with a ceremony performed by The Marquis of Postcode: DA14 4EF Camden, president of Kent CPFA, supported by the Landowner: London Borough of Bexley donors of the park, Lord and Lady Waring. Category: Principal Local Authority County: Kent (Metropolitan) Title information Local Authority: Bexley Council The land was gifted by The Right Honourable OS Grid ref: TQ467724 Samuel James Baron Waring in November 1929 Title Number: SGL701319 and vested in the Local Authority under the Public Health Act, to be laid-out as a public park and Sidcup is an urban district in the London Borough recreation ground. Waring Park was scheduled of Bexley, approximately 12 miles south east of as a public open space under the Council’s Town Central London. There is a mixture of large Victorian Planning Scheme. We understand there is a binding and Edwardian properties alongside typical 1930s restriction in the Deed of Gift and Conveyance suburbia, primarily owner-occupied semi-detached which guarantees the land will be held in perpetuity and detached housing. -

Manor House the Green, Sidcup, Da14 6Bw
LONG LEASEHOLD OPPORTUNITY - GRADE II LISTED MANOR HOUSE THE GREEN, SIDCUP, DA14 6BW VARIETY OF REGENERATIVE USES CONSIDERED INCLUDING A BOUTIQUE HOTEL, SPA, GASTRO PUB, RESTAURANT, OFFICE AND RESIDENTIAL OPPORTUNITY Manor House The Green, Sidcup, DA14 6BW 2 y e e l Damo ther BACKGROUND LOCATION d Plac Langfor a Clarence Road H for d Place g The Manor House, Sidcup is situated on the Nash Cottages Lan pledor Sandhurst Road ck Road Savills are delighted to offer Ap e Cr e north side of The Green close toescent its junction e Road oad Birkb Lydd R with ChislehurstC Road. Sidcup is a sought after l ch this landmark Grade II Listed ose ent suburban district of south east London in the esc tchur Stanle s y Road ence Cr late 18th Century Manor House ar London Borough of Bexley. Cl Chri Langfor d Place d a ld Road e located in the heart of Sidcup fi k e r The Property is approximately 0.1 milesLa south of Shel s Road er Ro b n d Victoria Road ury Close Al t Joh the High Street while Sidcup Railway Station lies S town Centre on The Green. A211 S approximately 1 mile to the north and providesLyminge Close ta aylors Clos t T io n The Property benefits from the d Ne direct links to Central London via Londona Cannon Ro ville Clos a le Ro d potential for conversion of the Street and London Charing Cross. It is 5a minutes Upd ws from the A20 and less than 15 minutesM from the e Stanhope Road ain R A222 Granville Road existing main house with some ad A2, M20 and M25 and is within approximatelyo ille Me ad v d Road an Gr S anville Roa ar d t h oneaffor hour of mostc major London airports and the Gr d limited new development on the Or Channeld Road Tunnel and ferry ports. -

Buses from St Pauls Cray (Sevenoaks Way)
Buses from St. Paul’s Cray (Sevenoaks Way) N199 Route finder Trafalgar Square Plumstead Common Ship Crook Log for Charing Cross 51 B14 Woolwich Blendon Bexleyheath Bus route Towards Bus stops Penhill Road Aldwych Town Centre for Shopping Centre Woolwich Arsenal Edison Road WELLING 51 Orpington ○M ○N ○P ○Q ○R for Covent Garden Albany Park BEXLEYHEATH Woolwich +A○A ○B ○C ○D Ludgate Circus Maylands Drive B14 Bexleyheath M ○D for City Thameslink WOOLWICH Welling Royal Road M ○E ○M Orpington Bexley Lane St. Pauls Cathedral Hail section& Ride ○S Blackfen Cleve Park School R6 Orpington ○E ○M The Drive R11 Green Street Green Bank Sidcup ○D Sidcup Glanville Road Sidcup Hill Sidcup Hill Hail & Ride section Knoll Road Cray Road Monument SIDCUP River Thames Sidcup High Street Sidcup Hill Night buses Church Road Middleton Avenue Chislehurst Road Elm Road Cray Road London Bridge s The Green The Green Suffolk Road Bus route Towards Bus stops for Guy’s Hospital ○S N199 Trafalgar Square City Hall Sidcup Crittall’s Corner Queen Mary’s Hospital R11 Rotherhithe Queen Mary’s Hospital Queen Mary’s Hospital Jamaica Road A&E B Block Key Bermondsey 51 Day buses in black Midfield Way VALLEY ROAD Chipperfield Road N199 Night buses in blue Canada Water MIDFIELD WAY —O Connections with London Underground Midfield Way St. Paul’s Wood Hill D o Connections with London Overground Breakspears Drive Croxley Green GRAYS FARM R Surrey Quays R Connections with National Rail D Connections with Docklands Light Railway M B Connections with river boats Plough Way A I WALSINGHAM RD N Tube station with 24-hour service Friday and R —O O Saturday nights when Night Tube services operate A Grove Street Mickleham Road D M Mondays to Saturdays and Sunday shopping hours only Beddington Road ©P1ndar Deptford ST. -

North Cray Place Part of Foots Cray Meadows
North Cray Place Part of Foots Cray Meadows Kent Gardens Trust 1 North Cray Place (part of Foots Cray Meadows) TABLE OF CONTENTS INTRODUCTION STATEMENT OF SIGNIFICANCE SITE DESCRIPTION LIST OF FIGURES FIGURE 1: Boundary and key features map. FIGURE 2: J. Andrews, A. Dury and W. Herbert, A Topographical Map of the County of Kent in Twenty Five Sheets (1769). FIGURE 3: OS Surveyors drawing 1799 (British Library OSD 129 FIGURE 4: Tithe map North Cray Parish (1838). Kent History and Library Centre FIGURE 5: Ordnance Survey 1st edition 6” map (1862-1875) FIGURE 6: Ordnance Survey 2nd edition 6” map (1898) FIGURE 7: Ordnance Survey 3rd edition 6” map (1910) FIGURE 8: Ordnance Survey 4th edition 6” map (1939 1940) FIGURE 9: Illustration of North Cray Place by J Bayly c1779 . Kent History and Library Centre FIGURE 10: North Cray Place (part of Foots Cray Meadows) 2015 FIGURE 11: Five Arch Bridge 2015 2 INTRODUCTION This site dossier and description has been prepared as part of the review of the five sites in the Kent area where Lancelot Capability Brown was engaged to carry out redesign of the landscape for the owners of those estates in the latter half of C18. This review has been developed into one of the chapters of a book entitled Capability Brown in Kent produced by the Kent Gardens Trust. The research was carried out by volunteers of the Kent Gardens Trust with support and editing by consultant Virginia Hinze. The extent of the area identified represents the remains of the designed landscape and does not necessarily cover all remaining elements or the historical extent of landscape changes and takes no account of current ownership.