Validation of Physical Activity Tracking Via Android Smartphones Compared to Actigraph Accelerometer: Laboratory-Based and Free-Living Validation Studies
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

A Middleware Framework for Application-Aware and User-Specific Energy Optimization in Smart Mobile Devices
Pervasive and Mobile Computing 20 (2015) 47–63 Contents lists available at ScienceDirect Pervasive and Mobile Computing journal homepage: www.elsevier.com/locate/pmc A middleware framework for application-aware and user-specific energy optimization in smart mobile devices Sudeep Pasricha a,∗, Brad K. Donohoo b, Chris Ohlsen c a Colorado State University, Fort Collins, CO 80523, USA b U.S. Department of the Air Force, Roy, UT 84067, UT 84067, USA c Woodward, Inc., Fort Collins, CO 80525, USA article info a b s t r a c t Article history: Mobile battery-operated devices are becoming an essential instrument for business, com- Received 5 August 2014 munication, and social interaction. In addition to the demand for an acceptable level of per- Received in revised form 22 December 2014 formance and a comprehensive set of features, users often desire extended battery lifetime. Accepted 7 January 2015 In fact, limited battery lifetime is one of the biggest obstacles facing the current utility and Available online 14 January 2015 future growth of increasingly sophisticated ``smart'' mobile devices. This paper proposes a novel application-aware and user-interaction aware energy optimization middleware Keywords: framework (AURA) for pervasive mobile devices. AURA optimizes CPU and screen back- Energy optimization Smart mobile systems light energy consumption while maintaining a minimum acceptable level of performance. Pervasive computing The proposed framework employs a novel Bayesian application classifier and management Machine learning strategies based on Markov Decision Processes and Q-Learning to achieve energy savings. Middleware Real-world user evaluation studies on Google Android based HTC Dream and Google Nexus One smartphones running the AURA framework demonstrate promising results, with up to 29% energy savings compared to the baseline device manager, and up to 5×savings over prior work on CPU and backlight energy co-optimization. -

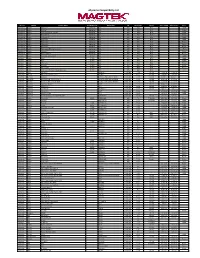
2014 BT Compatibility List 20141030
Item Brand Name Model 1 Acer Acer beTouch E210 2 Acer acer E400 3 Acer acer P400 4 Acer DX650 5 Acer E200 6 Acer Liquid E 7 Acer Liquid Mini (E310) 8 Acer M900 9 Acer S110 10 Acer Smart handheld 11 Acer Smart handheld 12 Acer Smart handheld E100 13 Acer Smart handheld E101 14 Adec & Partner AG AG vegas 15 Alcatel Alcatel OneTouch Fierce 2 16 Alcatel MISS SIXTY MSX10 17 Alcatel OT-800/ OT-800A 18 Alcatel OT-802/ OT-802A 19 Alcatel OT-806/ OT-806A/ OT-806D/ OT-807/ OT-807A/ OT-807D 20 Alcatel OT-808/ OT-808A 21 Alcatel OT-880/ OT-880A 22 Alcatel OT-980/ OT-980A 23 Altek Altek A14 24 Amazon Amazon Fire Phone 25 Amgoo Telecom Co LTD AM83 26 Apple Apple iPhone 4S 27 Apple Apple iPhone 5 28 Apple Apple iPhone 6 29 Apple Apple iPhone 6 Plus 30 Apple iPhone 2G 31 Apple iPhone 3G 32 Apple iPhone 3Gs 33 Apple iPhone 4 34 Apple iPhone 5C 35 Apple iPHone 5S 36 Aramasmobile.com ZX021 37 Ascom Sweden AB 3749 38 Asustek 1000846 39 Asustek A10 40 Asustek G60 41 Asustek Galaxy3_L and Galaxy3_S 42 Asustek Garmin-ASUS M10E 43 Asustek P320 44 Asustek P565c 45 BlackBerry BlackBerry Passport 46 BlackBerry BlackBerry Q10 47 Broadcom Corporation BTL-A 48 Casio Hitachi C721 49 Cellnet 7 Inc. DG-805 Cellon Communications 50 C2052, Technology(Shenzhen) Co., Ltd. Cellon Communications 51 C2053, Technology(Shenzhen) Co., Ltd. Cellon Communications 52 C3031 Technology(Shenzhen) Co., Ltd. Cellon Communications 53 C5030, Technology(Shenzhen) Co., Ltd. -
Udynamo Compatibility List
uDynamo Compatibility List Reader Manuf. Device Name Alt. Model Info Model Info OS OS Version Carrier Date Added Date Tested Type iDynamo 5 Apple iPad Air 2 Lightning N/A iOS N/A N/A Tablet iDynamo 5 Apple iPad Air* Lightning N/A iOS N/A N/A Tablet iDynamo 5 Apple iPad with Retina Display* Lightning N/A iOS N/A N/A Tablet iDynamo 5 Apple iPad mini 3 Lightning N/A iOS N/A N/A Tablet iDynamo 5 Apple iPad mini 2 Lightning N/A iOS N/A N/A Tablet iDynamo 5 Apple iPad mini* Lightning N/A iOS N/A N/A Tablet iDynamo 5 Apple iPhone 5c* Lightning N/A iOS N/A N/A Phone iDynamo 5 Apple iPhone 5s* Lightning N/A iOS N/A N/A Phone iDynamo 5 Apple iPhone 5* Lightning N/A iOS N/A N/A Phone iDynamo 5 Apple iPod touch (5th* generation) Lightning N/A iOS N/A N/A iPod iDynamo 5 Apple iPhone 6* Lightning N/A iOS N/A N/A Phone iDynamo 5 Apple iPhone 6 Plus* Lightning N/A iOS N/A N/A Phone iDynamo Apple iPad (3rd generation) 30 PIN N/A iOS N/A N/A Tablet iDynamo Apple iPad 2 30 PIN N/A iOS N/A N/A Tablet iDynamo Apple iPad 30 PIN N/A iOS N/A N/A Tablet iDynamo Apple iPhone 4s 30 PIN N/A iOS N/A N/A Phone iDynamo Apple iPhone 4 30 PIN N/A iOS N/A N/A Phone iDynamo Apple iPhone 3GS 30 PIN N/A iOS N/A N/A Phone iDynamo Apple iPod touch (3rd and 4th generation) 30 PIN N/A iOS N/A N/A iPod uDynamo Acer liquid MT liquid MT Android 2.3.6 101.18 1/24/14 1/24/14 uDynamo Alcatel Alcatel OneTouch Fierce 7024W Android 4.2.2 101.18 3/6/14 3/6/14 uDynamo ALCATEL Megane ALCATEL ONE TOUCH 5020T Android 4.1.2 101.18 8/10/15 8/10/15 uDynamo ALCATEL ALCATEL ONE TOUCH IDOL X ALCATEL -

Android Software Platform Development at Fujitsu
Android Software Platform Development at Fujitsu Makoto Honda Makoto Kobayashi Masahiko Nagumo Yasuhiro Kawakatsu Smartphones using the Android platform first appeared on the market in October 2008. They have since overtaken Apple’s iPhone—the first entry in the smartphone market—in number of units shipped and have helped to bring about major changes in the way that mobile phones are used. Android was developed and is distributed as open source software that a device maker integrates into its own hardware after adding original software technologies. The Android platform evolves in short cycles on the basis of software and hardware developments as the network infrastructure continues to expand in the form of WiMAX and LTE and as usage scenarios and services become increasingly diverse. Fujitsu has been developing Android smartphones with compelling functions and enhanced convenience since December 2010, when it released the REGZA Phone T-01C featuring a water-resistant enclosure, one-seg support, and FeliCa contactless IC card and infrared-communication functions. This paper describes Fujitsu’s approach to smartphone development, focusing on memory management and current-con- sumption management as important elements in the system design of the Android software platform, diverse manner modes for enhancing user convenience, high-picture-quality technol- ogy achieved by using the Mobile REGZA Engine, and audio-visual device-linking technology based on DLNA standards. 1. Introduction and Internet services, the smartphone market share of November 2007 marked the establishment of the Android devices continued to grow, and in fiscal 2011, Open Handset Alliance (OHA) centered about Google it came to exceed 50%. -

Small Spacecraft Technology State of the Art
NASA/TP–2015–216648/REV1 Small Spacecraft Technology State of the Art Mission Design Division Ames Research Center, Moffett Field, California December 2015 NASA STI Program . in Profile Since its founding, NASA has been dedicated • CONFERENCE PUBLICATION. to the advancement of aeronautics and space Collected papers from scientific and science. The NASA scientific and technical technical conferences, symposia, seminars, information (STI) program plays a key part or other meetings sponsored or in helping NASA maintain this important co-sponsored by NASA. role. • SPECIAL PUBLICATION. Scientific, The NASA STI Program operates under the technical, or historical information from auspices of the Agency Chief Information NASA programs, projects, and missions, Officer. It collects, organizes, provides for often concerned with subjects having archiving, and disseminates NASA’s STI. substantial public interest. The NASA STI Program provides access to the NASA Aeronautics and Space Database • TECHNICAL TRANSLATION. English- and its public interface, the NASA Technical language translations of foreign scientific Report Server, thus providing one of the and technical material pertinent to largest collection of aeronautical and space NASA’s mission. science STI in the world. Results are Specialized services also include creating published in both non-NASA channels and custom thesauri, building customized by NASA in the NASA STI Report Series, databases, and organizing and publishing which includes the following report types: research results. • TECHNICAL PUBLICATION. Reports of For more information about the NASA STI completed research or a major significant Program, see the following: phase of research that present the results of NASA programs and include extensive • Access the NASA STI program home page data or theoretical analysis. -

Supported Android Devices AT&T KDDI Minor Carriers / Other
AT&T Appendix Acer Iconia Tab A501 (A501) A – HTC Aria (LIBERTY) Supported HTC Lele (HTCPH06130) Android HTC Nexus One (NEXUSONE) HTC One VX (HTCPM36100) Devices HTC One X (HTCONEX) HTC Status (HTCSTATUS) HTC Vivid (HTCPH39100) Huawei Impulse 4G (HUAWEIU8800-51) LG Eclipse (LG-E970) LG Escape 4G (LG-P870) LG Nitro HD (LG-P930) LG Phoenix (LG-P505) LG Thrill 3D (LG-P925) LG Thrive (LG-P506) Motorola Atrix 2 (MB865) Motorola Atrix 3 (MB886) Motorola Bravo MB520 (MB520) Motorola FlipSide (MB508) Pantech Crossover (PANTECHP8000) Samsung Captivate (SAMSUNG-SGH-I897) Samsung Captivate Glide (SAMSUNG-SGH-I927) Samsung Galaxy Express (SAMSUNG-SGH-I437) Samsung Galaxy Note (SAMSUNG-SGH-I717) Samsung Galaxy Note II (SGH-I317) Samsung Galaxy Rugby Pro (SAMSUNG-SGH-I547) Samsung Galaxy S II (SAMSUNG-SGH-I777) Samsung Galaxy S III (SAMSUNG-SGH-I747) Samsung Galaxy S4 (SAMSUNG-SGH-I337) Samsung Galaxy Tab 8.9 (SGH-I957) Samsung Galaxy Tab 8.9 (SAMSUNG-SGH-I957) Samsung Rugby (SAMSUNG-SGH-I847) Samsung SkyRocket (SAMSUNG-SGH-I727) Sony Xperia T (LT30AT) KDDI HTC EVO 3D (ISW12HT) Minor Carriers / Other* LG Nexus 4 (NEXUS4) LG Optimus One (LG-P500) Motorola RAZR i (XT890) Samsung Galaxy Ace (GT-S5830) Samsung Galaxy SII LTE (SGH-I727R) Samsung Galaxy S III (GT-I9300) * Other denotes a device that is not officially carried by a network and is usually purchased unlocked. 1 Version 15 Sprint HTC EVO 3D (PG86100) HTC EVO 4G (PC36100) HTC EVO 4G LTE (EVO) HTC EVO Shift 4G (PG06100) HTC EVO View 4G (PG41200) HTC Hero (HERO200) HTC One (HTCONE) Kyocera ECHO -

Replicant and Android Freedom
Replicant and Android freedom Why phone freedom matters? (I) ● Smartphones gather way too much data on you: ● Non democratic countries. ● If you want to organize a protest? ● In which hands should this power be? ● What happens to the data if a democratic country becomes non-democratic ● Commercial usage of the Data? ● Unintended consequences Why phone freedom matters? (II) ● smartphones are computers? ● Yes because they run user-installable applications ● => they have the same freedom issues ● It©s too hard to support a device with proprietary parts in the long run: Cyanogenmod dropped the Nexus one for that exact reason. ● It©s Hard to port GNU/Linux on it when there are blobs First part ● Introduction to the freedom issues ● Solutions What is a smartphone ModemModem CPU Average Joe user Problem Average Joe User Free Proprietary software Applications applications Android Linux Kernel Advanced User Supported devices ● A lot of devices(too much to be listed here) are supported but not all Problem I (AdvancedUser) Google Applications( Proprietary Free market, applications software applications youtube etc...) Cyanogenmod Problem II (Advanced user) Android GUI Proprietary hardware libraries Linux kernel Nexus S: Proprietary parts I ● /system/etc/gps.conf ● /system/lib/libpn544_fw.so ● /system/lib/libsecril-client.so ● /system/vendor/bin/gpsd ● /system/vendor/bin/pvrsrvinit ● /system/vendor/etc/gps.xml ● /system/vendor/firmware/bcm4329.hcd ● /system/vendor/firmware/cypress-touchkey.bin Nexus S: Proprietary parts II ● /system/vendor/firmware/nvram_net.txt -

See List of Compatible Mobile Devices
Compatible Mobile Devices List Apple iOS Devices Azden i-Coustics products are fully compatible with the latest Apple iOS devices, including: iPhone 11 Pro*, 11*, Xr*, X* 8*, 8 Plus*, 7*, 7 Plus*, 6s, 6s Plus, SE, iPad Pro, iPad, iPad mini and iPod touch. *Use with iPhone models 7 and newer requires the use of Apple’s Lightning to headphone audio adapter Compatibility extends to earlier models as follows: iPhone 3G and newer (2008) iPad 2 and newer (2010) nd iPod Touch 2 Gen and newer (2008) Android Devices GOOGLE Motorola Samsung PIXEL 1, 2, 3* & 4* (all versions) Razr* All GALAXY NOTE MODELS NEXUS 4 Motorola One* Including Note10* & Note9 NEXUS 5 Moto G5, G6, G7 NEXUS 6 Moto E4, E5, E6 ALL GALAXY S MODELS* NEXUS 7 Moto Z2*, Z3*, Z4 Including S10 and S20 NEXUS 8 Moto X4 NEXUS 9 DROID RAZR M All GALAXY Tab Models NEXUS 10 DROID RAZR HD NEXUS ONE DROID RAZR MAXX HD Galaxy Z* NEXUS S PHOTON Q 4G LTE Galaxy A50 / A20 / A10e GALAXY NEXUS ATRIX HD Champ Neo DUOS DROID RAZR MAXX GALAXY Music HTC DROID RAZR GALAXY S Duos All HTC models including: ELECTRIFY 2 GALAXY Ace Plus DEFY XT GALAXY Beam HTC U12+* DROID 4 GALAXY Pocket HTC U11*/U11 Life* ATRIX 2 Black White HTC One models ADMIRAL Galaxy Mini 2 HTC Desire models ELECTRIFY GALAXY Y Duos Droid DNA PHOTON 4G GALAXY W HTC Evo 4G LTE i867 OMNIA W Droid Incredible 4G LTE TITANIUM GALAXY Xcover HTC One SV TRIUMPH GALAXY Nexus HTC 8XT ATRIX 4G GALAXY Ace GALAXY Gio LG GALAXY Fit GALAXY mini V50, V40, V35, V30, V30+ Nexus S G8X, G8, G7, G6, G5, G4 OMNIA 7 OPTIMUS G GALAXY 551 OPTIMUS L7, L5, L3, L2 GALAXY 580 Wave 723 * On Android devices, compatibility requires using the manufacturer’s USB-C adapter for headsets This list is not exhaustive and there may be some compatible devices not shown. -
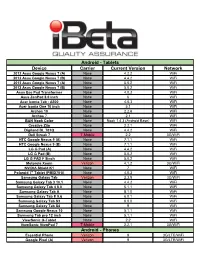
Device Carrier Current Version Network Android
Android - Tablets Device Carrier Current Version Network 2012 Asus Google Nexus 7 (A) None 4.2.2 WiFi 2012 Asus Google Nexus 7 (B) None 4.4.2 WiFi 2013 Asus Google Nexus 7 (A) None 5.0.2 WiFi 2013 Asus Google Nexus 7 (B) None 5.0.2 WiFi Asus Eee Pad Transformer None 4.0.3 WiFi Asus ZenPad 8.0 inch None 6 WiFi Acer Iconia Tab - A500 None 4.0.3 WiFi Acer Iconia One 10 inch None 5.1 WiFi Archos 10 None 2.2.6 WiFi Archos 7 None 2.1 WiFi B&N Nook Color None Nook 1.4.3 (Android Base) WiFi Creative Ziio None 2.2.1 WiFi Digiland DL 701Q None 4.4.2 WiFi Dell Streak 7 T-Mobile 2.2 3G/WiFi HTC Google Nexus 9 (A) None 7.1.1 WiFi HTC Google Nexus 9 (B) None 7.1.1 WiFi LG G Pad (A) None 4.4.2 WiFi LG G Pad (B) None 5.0.2 WiFi LG G PAD F 8inch None 5.0.2 WiFi Motorola Xoom Verizon 4.1.2 3G/WiFi NVIDIA Shield K1 None 7 WiFi Polaroid 7" Tablet (PMID701i) None 4.0.3 WiFi Samsung Galaxy Tab Verizon 2.3.5 3G/WiFi Samsung Galaxy Tab 3 10.1 None 4.4.2 WiFi Samsung Galaxy Tab 4 8.0 None 5.1.1 WiFi Samsung Galaxy Tab A None 8.1.0 WiFi Samsung Galaxy Tab E 9.6 None 6.0.1 WiFi Samsung Galaxy Tab S3 None 8.0.0 WiFi Samsung Galaxy Tab S4 None 9 WiFi Samsung Google Nexus 10 None 5.1.1 WiFi Samsung Tab pro 12 inch None 5.1.1 WiFi ViewSonic G-Tablet None 2.2 WiFi ViewSonic ViewPad 7 T-Mobile 2.2.1 3G/WiFi Android - Phones Essential Phone Verizon 9 3G/LTE/WiFi Google Pixel (A) Verizon 9 3G/LTE/WiFi Android - Phones (continued) Google Pixel (B) Verizon 8.1 3G/LTE/WiFi Google Pixel 2 Verizon 8.1 3G/LTE/WiFi Google Pixel 3 XL None 9 3G/LTE/WiFi HTC Desire (International) -

Amazon Amazon Fire Apple Iphone 5, Ipad 4, Ipad Mini, Iphone 5C
Amazon Amazon Fire Apple iPhone 5, iPad 4, iPad Mini, iPhone 5c, iPhone 5s, iPad Air, iPad Mini 2/3, iPad Air 2, iPhone 6 Plus, iPhone 6, iPhone 6s, iPhone 6s Plus, iPhone SE, iPhone 7, iPhone 7 Plus, iPhone 8, iPhone 8 Plus, iPhone X BlackBerry Storm II / 9550, Flip 8220/8230, 8900, Curve 8520 / 8530, Curve 9360, Curve 9380, Bold 9790, Curve 9370, Curve 9310, Z10, Q10, Z30, Tour 9630, Classic Google Pixel 4, Pixel 4 XL HTC Nexus One, Trophy, Droid Incredible 2, Inspire 4G, Merge, myTouch 4G, Sensation 4G, Wildfire, Wildfire S, Titan, Rhyme, Sensation XE, Vivid, Rezound, One S, Windows Phone 8X, One X, Evo 4G LTE, Droid DNA, One SV, One VX, One, One Mini, EVO 4G, EVO Shift 4G, HD2, Desire, EVO 3D, HD7, One (E8), One Remix/One Mini 2, One M8 LG Lotus, Revolution, Thrive, Optimus M MS690, Optimus S LS670, Optimus T P509, Optimus U US670, Optimus V VM670, Select MN180, UX-300, Vortex VS660, Revere, Thrill/ Optimus 3D, Optimus Hub, Marquee, Ignite, Nitro HD, Optimus 2, Optimus LTE, Optimus Slider, Optimus Sol, Optimus One, Spectrum, Connect 4G, Venice, Intuition, Nexus 4, Lucid, Lucid 2, Optimus F7, Optimus Zone, Enact, G2, Nexus 5, LG G3, LG G4, LG G5 Motorola Defy MB525, Droid 2 Global, DROID BIONIC XT865, Droid Pro A957, Droid RAZR, DROID RAZR MAXX, DROID 4, Motoluxe, Photon Q, Droid RAZR HD, Droid RAZR MAXX HD, Droid RAZR M, Droid Mini, Droid Ultra, Droid Maxx, Moto X, Electrify M, Electrify 2, Moto G, Devour A555, ATRIX 4G MB860, Backflip, Moto E, Droid Turbo, Google Nexus 6 Nokia E71, E72, N78, N81, N85, N86 8MP, N900, E63, 800, 710, -

A List of Compatible Devices
Compatible Mobile Devices List HTC HTC EndeavorU ATRIX HD HTC Droid DNA HTC Evita DROID RAZR MAXX HTC HTC One X+ HTC Ville DROID RAZR HTC One S HTC Primo ELECTRIFY 2 HTC EVO 4G LTE HTC Jewel DEFY XT HTC Desire SV HTC Valentewx DROID 4 HTC Desire C HTC Golf ATRIX 2 HTC one X HTC Fireball ADMIRAL HTC Butterfly HTC Proto ELECTRIFY HTC Desire X HTC DLXJ PHOTON 4G HTC Dream i867 HTC Magic, Samsung TITANIUM HTC Hero Champ Neo DUOS TRIUMPH HTC Click GALAXY Note II ATRIX 4G HTC Bravo GALAXY Music HTC Desire[3] GALAXY S Duos GOOGLE HTC Incredible GALAXY Ace Plus NEXUS 4 HTC Legend GALAXY S III 4G NEXUS 10 HTC Buzz GALAXY S4 NEXUS ONE HTC Espresso GALAXY S4 Mini NEXUS S HTC Liberty[7] GALAXY Beam GALAXY NEXUS HTC Supersonic GALAXY Pocket HTC Ace Black White LG HTC Vision Galaxy Mini 2 OPTIMUS G HTC Glacier GALAXY S III OPTIMUS L7 HTC Gratia GALAXY Y Duos OPTIMUS L5 HTC Stallion GALAXY W OPTIMUS L3 HTC Mecha GALAXY S II 4G OPTIMUS L2 HTC Speedy OMNIA W HTC Vivo GALAXY Xcover Apple HTC Marvel GALAXY Nexus iPhone 3G (all models) HTC Saga GALAXY S II iPhone 3Gs (all models) HTC VivoW GALAXY Ace iPhone 4 (all models) HTC Lexikon GALAXY Gio iPhone 4s (all models) HTC Pyramid GALAXY Fit iPhone 5 (all models) HTC Status GALAXY mini HTC Icon Nexus S iPod touch 2nd Generation HTC Shooter GALAXY S iPod touch 3rd Generation HTC Doubleshot GALAXY 5 iPod touch 4th Generation HTC Rider OMNIA 7 iPod touch 5th Generation HTC ShooterU GALAXY 551 HTC Holiday GALAXY 580 iPad 3rd Generation & newer HTC Bliss Wave 723 HTC Kingdom GALAXY Tab 3 HTC Ruby GALAXY Tab Pro HTC Pico Motorola HTC Pyramid LE DROID RAZR M HTC Runnymede DROID RAZR HD DROID RAZR MAXX HD HTC Vigor PHOTON Q 4G LTE *There may be some compatible devices not shown on this list. -
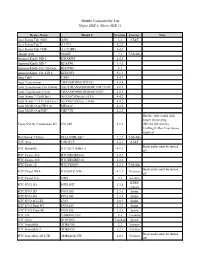
Shuttle Compatibility List Major SDK 5, Minor SDK 13
Shuttle Compatibility List Major SDK 5, Minor SDK 13 Device Name Model # Version Carrier Note Acer Iconia Tab A501 A501 3.2 AT&T Acer Iconia Tab 7 A1-713 4.2.2 Acer Iconia Tab 7 HD A1-713HD 4.4.2 Alcatel A30 9024W 7.1 T-Mobile Amazon Kindle HD 6 KWARWI 4.4.3 Amazon Kindle HD 7 KFASWI 4.4.3 Amazon Kindle Fire 5th Gen. KFFOWI 5.1 Amazon Kindle Fire HD 8 KFDOWI 5.1.1 Alps Tab9 TAB9 4.4.2 Asus Transformer TRANSFORMERTF101 4.0.4 Asus Transformer Pad Infinity ASUSTRANSFORMERPADTF700T 4.0.3 Asus Transformer Prime TRANSFORMERPRIMETF201 4.0.3 Asus Nexus 7 (2nd Gen.) NEXUS7 (Device: FLO) 4.4.2 Asus Nexus 7 LTE (2nd Gen.) NEXUS7 (Device: DEB) 4.4.2 Asus MeMO Pad FHD 10 ME302C 4.2.2 Asus MeMO Pad HD7 ME173X 4.2.2 Shuttle: only works with longer phone plug: Casio G'zOne Commando 4G C8114G 4.1.2 (ID-80110010-028) UniMag II: Rev G or above required Dell Streak 7 Tablet DELLSTREAK7 2.2.2 T-Mobile HTC Aria LIBERTY 2.2.1 AT&T Beats audio must be turned HTC Butterfly HTCBUTTERFLY 4.1.1 off HTC Desire 816 HTCDESIRE816 4.4.2 HTC Desire 310 HTCDESIRE310 4.2.2 HTC Desire Z HTCVISION 2.2.1 T-Mobile Beats audio must be turned HTC Droid DNA HTC6435LVW 4.1.1 Verizon off HTC Droid Eris ERIS 2.1 Verizon KDDI HTC EVO 3D ISW12HT 2.3.4 (Japan) HTC EVO 3D PG86100 2.3.3 Sprint HTC EVO 4G PC36100 2.3.3 Sprint HTC EVO 4G LTE EVO 4.0.3 Sprint HTC EVO Shift 4G PG06100 2.3.3 Sprint HTC EVO View 4G PG41200 2.3.3 Sprint HTC G2 T-MOBILEG2 2.2 T-mobile HTC Hero HERO200 2.1-update1 Sprint HTC Incredible ADR6300 2.2 Verizon HTC Incredible 2 ADR6350 2.2.1 Verizon Beats audio must