Pakistan Child Survival Project Number 39-0496 Contract Number Project 391-04 96-C-00-0769-00
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

MBBS / BDS ADMISSIONS Government Medical Colleges of Azad Jammu & Kashmir (AJ&K) and Reserved Seats for AJ&K Nationals in Pakistan, Session 2019-2020
University of Health Sciences Lahore MBBS / BDS ADMISSIONS Government Medical Colleges of Azad Jammu & Kashmir (AJ&K) and Reserved Seats for AJ&K Nationals in Pakistan, Session 2019-2020 Online applications are invited from eligible (First Class State Subject) candidates for admissions in First Year MBBS and BDS against reserved seats for AJ&K Nationals, Refugees 1947and Refugees 1989 (conditions apply), in the following Public Sector Medical/Dental Colleges of Pakistan (Punjab, Khyber Pakhtunkhwa, Balochistan & Sindh) and Public Sector Medical Colleges of AJ&K. Admissions will be made strictly on merit basis as per PM&DC Admission Regulations and Admission Policy of AJ&K Government in vogue: Medical/Dental Institutions of Pakistan Punjab (MBBS) Khyber Pakhtunkhwa (MBBS) Allama Iqbal Medical University Lahore Ayub Medical College Abbottabad Fatima Jinnah Medical University Lahore Gomal Medical College D.I Khan King Edward Medical University Lahore Khyber Medical University Peshawar Nishtar Medical University Multan Saidu Sharif Medical College Swat Punjab Medical University Faisalabad Khyber Pakhtunkhwa (BDS) Quaid e Azam Medical College Bahawalpur Dental Unit Ayub Medical College Abbottabad Rawalpindi Medical University Rawalpindi Sindh (MBBS) Services Institute of Medical Sciences Lahore Chandka Medical College Larkana Sheikh Zayad Medical College Rahim Yar Khan Balochistan (MBBS) Punjab (BDS) Bolan Medical College Quetta de’Montmorency College of Dentistry Lahore Medical Institutions of AJ&K Azad Jammu Kashmir Medical College Muzaffarabad Mohtarma Be’Nazir Bhutto Shaheed Medical College Mirpur Poonch Medical College Rawalakot 1. ELIGIBILITY CRITERIA i) Qualifications: In accordance with “MBBS and BDS (Admissions, House Job and Internship) Regulations, 2018, as amended on 30th May, 2019” of Pakistan Medical and Dental Council, the required qualifications for admissions are as follows: The applicant has passed, obtaining minimum Seventy percent (770/1100) marks, in Higher Secondary School Certificate (HSSC) or F.Sc. -

Multilocus Enzyme Electrophoresis And
Am. J. Trop. Med. Hyg., 75(2), 2006, pp. 261–266 Copyright © 2006 by The American Society of Tropical Medicine and Hygiene MULTILOCUS ENZYME ELECTROPHORESIS AND CYTOCHROME B GENE SEQUENCING–BASED IDENTIFICATION OF LEISHMANIA ISOLATES FROM DIFFERENT FOCI OF CUTANEOUS LEISHMANIASIS IN PAKISTAN JORGE D. MARCO,* ABDUL M. BHUTTO, FAROOQ R. SOOMRO, JAVED H. BALOCH, PAOLA A. BARROSO, HIROTOMO KATO, HIROSHI UEZATO, KEN KATAKURA, MASATAKA KORENAGA, SHIGEO NONAKA, AND YOSHIHISA HASHIGUCHI Department of Parasitology, Kochi Medical School, Kochi University, Kochi, Japan; Instituto de Patología Experimental, Facultad de Ciencias de la Salud, Universidad Nacional de Salta/Consejo Nacional de Investigaciones Científicas y Técnicas, Salta, Argentina; Department of Dermatology and Incharge Leprosy Unit, Chandka Medical College/Hospital Larkana, Sindh, Pakistan; Department of Veterinary Hygiene, Faculty of Agriculture, Yamaguchi University, Yamaguchi, Japan; Department of Dermatology, Faculty of Medicine, University of the Ryukyus, Okinawa, Japan; Laboratory of Parasitology, Department of Disease Control, Graduate School of Veterinary Medicine, Hokkaido University, Sapporo, Japan Abstract. Seventeen Leishmania stocks isolated from cutaneous lesions of Pakistani patients were studied by multi- locus enzyme electrophoresis and by polymerase chain reaction amplification and sequencing of the cytochrome b (Cyt b) gene. Eleven stocks that expressed nine zymodemes were assigned to L. (Leishmania) major. All of them were isolated from patients in the lowlands of Larkana district and Sibi city in Sindh and Balochistan provinces, respectively. The remaining six, distributed in two zymodemes (five and one), isolated from the highland of Quetta city, Balochistan, were identified as L. (L.) tropica. The same result at species level was obtained by the Cyt b sequencing for all the stocks examined. -

OFFICE of the PRINCIPAL CHANDKA MEDICAL COLLEGE SHAHEED MOHTARMA BENAZIR BHUTO Clo Cl) E
OFFICE OF THE PRINCIPAL CHANDKA MEDICAL COLLEGE SHAHEED MOHTARMA BENAZIR BHUTO MEDICAL UNIVERSITY (SMBBMU) LARKANA, SINDH, PAKISTAN Phont No. (92)4174.9410715 & 9410724 Fax No, (92). 074-9410511 Digit.I're1ilwn. Exhan No.074-9410750 ExI: 311. 312 & 313 . ss-s' & ww'.s '.,t1,mu .du._pk E-ntail inioi iu.edu.14 & j1osmbbrnu.edu.pk - . - .1 . - . - a a - a a - a • - • • NO. CMC/ACCI'S/ c DATED: /2018 To, The Director Information (Advertisement) Public Relation Department. Government of Sindh, Block No.96. Karachi. Subject: NOTICE OF INVITATION TENDER. Five Copies for Invitation of Tender for SMBB Medical University. Larkana, are sent herewith, with the request that the said notice be published in widely circulated daily 'DAWN' Karachi, "JANG" Karachi, "KAWISH" Hyderabad and other newspapers in single insertion. NCIPAL CHANDKA MEDICAL COLLEGE LA RKA NA Copy for Information to: • The Registrar SMBB, Medical University Larkana. • Director Finance, SMBB, Medical University Larkana. • to Vice Chancellor, SMBB Medical University, Larkana. \f Director (A&F) Sindh Public Procurement Regularity Authoi'ity. Government of Sindh Karachi. for SPPRA website. • Incharge website SMBB Medical University, Larkana. • Office record. 6 z E—. cLO Cl) OFFICE OF THE PRINCIPAL CHANDKA MEDICAL COLLEGE SHAHEED MOHTARMA BENAZIR BHUTTO MEDICAL UNiVERSITY (SMBBMU) LARKANA, SINDH, PAKISTAN Phone No. (92).074-9410715 & 9410724 Fax No. (92)- 074-9.110511 Digital Telephone Exchange No.074-9410750 ExI: 311.312 & 313 Website : www.cmc.edu.pk & www.sinithmu.edu.pk E-mail : into nw.edu.pk & [email protected] • a -S • - JS • - NO.CMC/ACCrS/9 ft1 DATED: I'/2O18 NOTICE OF INVITATION TENDER Sealed tenders are invited from the manufactures or repair of Transport only registered with Sales Tax and Income Tax Departments having at least 05 years Experience in related field of Transport and supply of items (repair of Uino Bus) for the Financial Year 2017-20 18 in respect of Chandka Medical College Larkana. -

College Inspection Report
PAKISTAN MEDICAL COMMISSION LAST RECOGNIZED INSPECTION GRADES OF PRIVATE MEDICAL COLLEGES Sr. Date of Previous Name of Institute City Grade No. Inspection 1. Abbottabad International Medical College Abbottabad. 17-12-2019 A 2. Abwa Medical College Faisalabad 20-11-2018 B 3. Aga Khan University Medical College Karachi. 05-08-2019 A+ 4. Akhtar Saeed Medical & Dental College Lahore. 26-08-2019 A 5. Al Aleem Medical College Lahore 29-08-2019 B 6. Al-Nafees Medical College Islamabad. 30-12-2015 C 7. Al-Tibri Medical College Karachi. 08-11-2013 B 8. Amna Inayat Medical College Lahore. 28-09-2017 C 9. Avicenna Medical College Lahore. 28-08-2019 A 10. Aziz Fatimah Medical & Dental College Faisalabad. 21-03-2018 C 11. Azra Naheed Medical College Lahore. 30-04-2015 B 12. Bahria University Medical College Karachi. 07-08-2019 B 13. Bakhtawar Amin Medical & Dental College Multan 20-02-2016 A 14. Baqai Medical College Karachi. 19-12-2018 F 15. Central Parks Medical College Lahore. 10-02-2015 C 16. CMH Institute of Medical Sciences Bahawalpur Bahawalpur 22-08-2019 C 17. CMH Kharian Medical College Kharian Cantt. 31-07-2019 B 18. CMH Lahore Medical College Lahore Cantt. 30-08-2019 A+ 19. CMH Multan Institute of Medical Sciences CIMS Multan Cantt 20-08-2019 A 20. Continental Medical College Lahore. 16-10-2018 C GRADING CRITERIA: 92.5% or above = A+, 85% or above = A, 77.5% or above = B, 70% or above = C, 69.9% or lower = F Sr. Date of Previous Name of Institute City Grade No. -

Abstract of ICEHSR
7th International Conference of Endorsing Health Science Research – ICEHSR-19 1 7th International Conference of Endorsing Health Science Research – ICEHSR-19 PREFACE International Conference for Endorsing Health Science Research has been a platform since 6 years for researchers from all over the world to exchange their thoughts on research and future developments in health sciences. ICEHSR with its previous impactful scientific history, has now become a brand enhancing the knowledge and information through numerous scientific activities throughout the session including keynote talks, workshops, panel sessions, scientific oral and poster presentations and publications. For the year 2019, team AEIRC is now back with its 7th International Conference for Endorsing Health Science Research (ICEHSR’19) in collaboration with World Health Organization (WHO) with the theme entitled: “Health for All; Everyone Everywhere” at Dow University of Health Sciences, Ojha Campus. AEIRC has been involved in arranging this mega event each year to encourage younger researchers in the field of health sciences by promoting the tradition of research through investigation, questioning and reaching out to appropriate answers. This year ICEHSR has been programmed to bring in the views from different health sectors. The main aim is to indulge the scientists and researchers from biomedical, environmental, psychological, pharmaceutical and all other health domains to identify the social issues and rather than just discussion the focus is break through the barriers and reach out to all possible solutions for it. This abstract book encloses an extracted form of all the sessions/talks delivered by our honorable speakers as well as 161 abstracts those were selected in the conference, presented by one of the author as poster and oral presentations. -

Viral Hepatitis in Pakistan: Past, Present, and Future 1Amna Subhan Butt, 1Fatima Sharif
EJOHG Amna Subhan Butt, Fatima Sharif 10.5005/jp-journals-10018-1172 MINI REVIEW Viral Hepatitis in Pakistan: Past, Present, and Future 1Amna Subhan Butt, 1Fatima Sharif ABSTRACT Viral hepatitis is a major cause of morbidity and mortality worldwide and a rising cause for concern in Asian countries. Weather it is blood borne or water/food borne hepatotropic virus, increasing burden is alarming for Asian countries. In this review we have evaluated the existing data to estimate the burden of viral hepatitis in populations of all age groups nationwide, along with an assessment of the risk factors and preventive and management strategies currently employed in Pakistan. The aim of our work is to consolidate and supplement the present knowledge regarding viral hepatitis in light of past and present trends and to provide future direction to the existing health policies. Keywords: Hepatitis A, Hepatitis B and C, Hepatitis E, Pakistan, Viral hepatitis. How to cite this article: Butt AS, Sharif F. Viral Hepatitis in Pakistan: Past, Present, and Future. Euroasian J Hepato-Gastroenterol 2016;6(1):70-81. Source of support: Nil Conflict of interest: None Copyright and License information: Copyright © 2016; Jaypee Brothers Medical Publishers (P) Ltd. This work is licensed under a Creative Commons Attribution 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by/3.0/ FOOD BORNE PATHOGENS: of acute hepatitis A are much lower than the actual rate HEPATITIS A AND E existing in the population.11 Hepatitis E in Pakistan has been witnessed to occur as Developing countries are at a high risk of infection with outbreaks and sporadic cases in circumstances involving orofecal pathogens. -
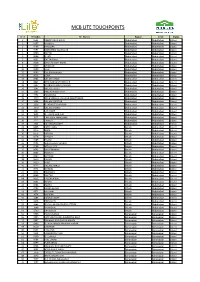
Mcb Lite Touchpoints
MCB LITE TOUCHPOINTS Sr. # Br Codes Br. Names Region Circle Status 1 0585 ABBOTTABAD MAIN Abbottabad Abbottabad Litized 2 0587 HARIPUR Abbottabad Abbottabad Litized 3 0588 HAVELIAN Abbottabad Abbottabad Litized 4 0591 MANSEHRA Star Branch Abbottabad Abbottabad Litized 5 0600 BATTAL Abbottabad Abbottabad Litized 6 0606 GHAZI Abbottabad Abbottabad Litized 7 0622 BATTAGRAM Abbottabad Abbottabad Litized 8 0628 SARAI NIAMAT KHAN Abbottabad Abbottabad Litized 9 0639 SHINKIARI Abbottabad Abbottabad Litized 10 0640 OGHI Abbottabad Abbottabad Litized 11 0643 QALANDARABAD Abbottabad Abbottabad Litized 12 0651 LORA Abbottabad Abbottabad Litized 13 0761 VILLAGE KHAKI Abbottabad Abbottabad Litized 14 0824 NEW DARBAN TOWNSHIP Abbottabad Abbottabad Litized 15 1197 DARBAND ADDA HARIPUR Abbottabad Abbottabad Litized 16 1267 VILLAGE ALLULI Abbottabad Abbottabad Litized 17 1303 PIND KARGOO KHAN Abbottabad Abbottabad Litized 18 1304 KANGRORA Abbottabad Abbottabad Litized 19 1320 AYUB MEDICAL COLLEGE ABBOTTABAD Abbottabad Abbottabad Litized 20 1324 VILLAGE QAZIPUR Abbottabad Abbottabad Litized 21 1358 GHAZIKOT TOWNSHIP Abbottabad Abbottabad Litized 22 1370 VILLAGE JHANGI Abbottabad Abbottabad Litized 23 1387 LAB MORE Abbottabad Abbottabad Litized 24 1655 G.T.ROAD HARIPUR Abbottabad Abbottabad Litized 25 1671 LARI ADDA MANSEHRA Abbottabad Abbottabad Litized 26 1713 THAKOT Abbottabad Abbottabad Litized 27 1724 KALABAGH CANTT Abbottabad Abbottabad Litized 28 0455 FATEH JANG Attock Abbottabad Litized 29 0475 NARA Attock Abbottabad Litized 30 0575 MITHIAL Attock -
MBBS-Session-2017-18.Pdf
Declaration of Geneva (Code of Ethics) At the time of being admitted as member of the medical profession • I solemnly pledge myself to consecrate my life to the service of humanity. • I will give to my teachers the respect and gratitude which is their due. • I will practice my profession with conscience and dignity • The health of my patient will be my first consideration • I will respect secrets, which are confided in me. • I will maintain by all means in my power the honor and noble traditions of the medical profession. • I will not permit considerations of religion, nationality, race, party politics or social standing to intervene between my duty and my patients. • I will maintain the utmost respect for human life from the time of conception and even under threat I will not use my medical knowledge to the laws humanity. • I make these promises solemnly, freely and upon my honour. HEALTH DEPARTMENT, GOVT. OF SINDH Content 05 DUHS 10 INTRODUCTION MESSAGES 06 * H.E. Governor Sindh & Chancellor JSMU 22 * H.E. Chief Minister Sindh & Pro-Chancellor LUMHS 32 * H.E. Health Minister Sindh DOW UNIVERSITY OF HEALTH SCIENCES PUMHSW 44 (DUHS), KARACHI 10 * Vice Chancellor Message * Introduction to DUHS SMBBMU 54 * Distribution of Seats SMBBMC 64 JINNAH SINDH MEDICAL UNIVERSITY (JSMU), KARACHI 22 * Vice Chancellor Message * Introduction to JSMU * Distribution of Seats LIAQUAT UNIVERSITY OF MEDICAL & Dow University of Health HEALTH SCIENCES (LUMHS), JAMSHORO 32 Sciences (DUHS), Karachi * Vice Chancellor Message www.duhs.edu.pk * Introduction to LUMHS -
PNJR-4Th-Annual-Report.Pdf
PNJR Report 2017-18 Theme PNJR 4th year of Success: From Infancy to a leader in National Health Registries. Pakistan: A cradle of oldest civilizations in the world Dedicated to the memory of legendary forefather of eastern medicine Hakim Mohammed Said Pakistan Arthroplasty Society (PAS) Pakistan National Joint Registry (PNJR) www.arthroplasty.org.pk www.pasnjr.org 01 Hakim Mohammed Said (1920 – 1998) Hakim Mohammed Said was a medical researcher, scholar, philanthropist, and a Governor of Sindh Province, Pakistan from 1993 until 1996. Said was one of Pakistan's most prominent medical researchers in the eld of Eastern medicines. He established the Hamdard Foundation in 1948. Herbal medical products of the Hamdard Foundation became household names in Pakistan. Hakim Mohammed Said authored and compiled about 200 books in medicine, philosophy, science, health, religion, natural medicine, literary, social, and travelogues. In 1981, Said became one of the founding member of the World Cultural Council. Contents Foreword 05 List of Authors 07 PNJR Steering Committee 09 Part 1: PNJR from infancy to a leader in National Health Registries I. Leadership in National Health Registries 11 II. Upgrades in the Data Collection Model 15 III. PNJR Clinical Coordinator Network 25 IV. PNJR Partnership with HRAB (Health Research Advisory Board) 29 V. PNJR Stake Holders Network 33 VI. Promising Future and Broadening Horizons 41 Part 2: Data Analysis and Reporting I. Primary Total Knee Arthroplasty 45 II. Revision Total Knee Arthroplasty 59 III. Primary Total Hip Arthroplasty 65 IV. Revision Total Hip Arthroplasty 79 PAS Current National Board 84 International Fellows 85 National Fellows 86 Partners of Pakistan Arthroplasty Society (PAS) Spanish Knee Society Foreword It is with great pleasure that I write this foreword to the fourth edition of the Pakistan National Joint Registry. -

Reflections on a Visit to Karachi: a Small World, After All Paul A
Georgia State University College of Law Reading Room Faculty Publications By Year Faculty Publications 12-1-2009 Reflections on a Visit to Karachi: A Small World, After All Paul A. Lombardo Georgia State University College of Law, [email protected] Follow this and additional works at: https://readingroom.law.gsu.edu/faculty_pub Part of the Comparative and Foreign Law Commons Recommended Citation Paul A. Lombardo, Reflections on a Visit to Karachi: A Small World, After All, Bioethics Links, Dec. 2009, at 1. This Article is brought to you for free and open access by the Faculty Publications at Reading Room. It has been accepted for inclusion in Faculty Publications By Year by an authorized administrator of Reading Room. For more information, please contact [email protected]. Volume 5 Issue 2 December 2009 cbecSIUT Pakistan Centre of Biomedical Ethics and Culture Bioethics Links Each year we invite national and international students and faculty to participate in different activities in CBEC. In this issue of Bioethics Links some of our guests, including a visiting faculty member from America, write about their impressions of their visit to CBEC and Karachi. Editor Reflections on a Visit to Karachi: A Small World, after All Paul A. Lombardo, Ph.D., J.D.* It was well past midnight when my plane of the old city doctors at SIUT face landed at the Jinnah International Airport in daunting challenges in identifying Karachi and after almost a full day in appropriate donors and navigating the transit, fatigue had dulled my perceptions. medical complexities of transplant surgery But by the time I made the trip through the for those in need of replacement organs. -

Appendix-II Pakistani Scheduled Banks Branches
Appendix-II Pakistani Scheduled Banks Branches Al Baraka Bank (Pakistan) Sukkur Kasur Swabi Ltd. (120) Khanewal Talagang Abbottabad Khanpur (R.Y Khan) Timergara Arifwala Kotri Vehari Attock Zhob Badin Lahore (17) Bahawalnagar -Anarkali Allied Bank Ltd. (998) Bahawalpur -Bank Square Market Abbaspur Burewala -Barkat Market, Garden Town Chichawatni -Cavalry Ground Abbottabad (6) Chistian -Circular Road -Supply Bazar Daska -DHA-Phase-II -The Mall Depalpur -DHA-Phase-VI -Bara Towers, Jinnahabad Dera Ghazi Khan -DHA-S-Block -Murree Road Dera Ismail Khan -Faisal Town -Mansehrah Road Dina -Gulshan Block, Allama Iqbal Town -Pine View Road Ellahabad -Hali Road, Gulberg II -M.M. Alam Road, Gulberg-III Adda Farid Nagar Faisalabad (2) -Maclod Road Adda Johal -Civil Line -Shadman Adda Nandi Pur -Chiniot Bazar -Shadman Colony Adda Zakhera -Shaukat Khanum Road Ahmed Pur East Fateh Jhang -Urdu Bazar Akalgarh (AK) Akhora Khatak Gujranwala (2) Larkana Akwal (Talagang) -Anwar Industrial Complex Mailsi Ali Pur -Main G.T. Road Mansehra Alipur Chatha Mardan Arifwala Gilgit Mian Channu Attock Gojra Minawali Bagh (AK) Gujrat Mingora Hafizabad Mirpur (AK) Bahawalnagar (3) Haripur Mirpurkhas -Jail Road, -Main Raod Hyderabad (2) Multan (3) -Minchin Abad Road -Saddar -Abdali Road -Market Area, -Kaswar Gardezi Road Bahawalpur (8) -Mushahid Trade Centre -Model Town B Haroonabad -New Grain Market Muzzaffarabad -Satellite Town Islamabad (4) Okara -Dubai Chowk, Ahmedpur Road -Blue Area, -One Unit Chowk -F-10 Markaz, Peshawar (3) -Circular Road -Jinnah Avenue -Hayatabad -

Precipitating Risk Factors, Clinical Presentation, and Outcome of Diabetic Ketoacidosis in Patients with Type 1 Diabetes
Open Access Original Article DOI: 10.7759/cureus.4789 Precipitating Risk Factors, Clinical Presentation, and Outcome of Diabetic Ketoacidosis in Patients with Type 1 Diabetes Warsha Ahuja 1 , Navin Kumar 2 , Sumeet Kumar 2 , Amber Rizwan 3 1. Internal Medicine, Jinnah Sindh Medical University, Karachi, PAK 2. Internal Medicine, Chandka Medical College Hospital Larkana, Larkana, PAK 3. Family Medicine, Dr. Ruth Pfau Hospital, Karachi, PAK Corresponding author: Amber Rizwan, [email protected] Abstract Introduction Over the past few years, there have been drastic advancements in the management of type 1 and 2 diabetes mellitus (DM). Prevention of complications is a prime concern of all physicians dealing with DM. However, whether or not these interventions have helped in reducing the incidence of diabetic ketoacidosis (DKA) in patients with type 1 DM, is still an unanswered question. The aim of this study is to assess the clinical pattern of DKA, evaluate its outcomes, and study the predictors of outcome. Methods The study was conducted as a prospective, observational one in the department of medicine of a tertiary care hospital from July-December 2018. Patients of type 1 DM presenting in the emergency department with DKA were evaluated for their predisposing factors, clinical presentation, biochemical parameters, rate of mortality, and predictors of mortality. Data was processed through and analyzed using IBM SPSS Statistics for Windows, version 22.0 (IBM Corp., Armonk, NY). Results The common clinical presentations include severe vomiting (32.2%), abdominal pain (27.9%), and depressed mental state (DMS) (26.8%). Infections (36.5%) and inadequate insulin dose (22.5%) were frequently seen as the predisposing factors.