Session 4: Radiation Protection of Patients, Staff and the Public In
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Radiosynthesis and in Vivo Evaluation of a 18F-Labelled Styryl-Benzoxazole Derivative for Β-Amyloid Targeting
Author's Accepted Manuscript Radiosynthesis and in vivo Evaluation of a 18F- Labelled Styryl-Benzoxazole Derivative for β- Amyloid Targeting G.Ribeiro Morais, L. Gano, T. Kniess, R. Berg- mann, A. Abrunhosa, I. Santos, A. Paulo www.elsevier.com/locate/apradiso PII: S0969-8043(13)00292-3 DOI: http://dx.doi.org/10.1016/j.apradiso.2013.07.003 Reference: ARI6294 To appear in: Applied Radiation and Isotopes Received date: 9 January 2013 Revised date: 15 April 2013 Accepted date: 1 July 2013 Cite this article as: G.Ribeiro Morais, L. Gano, T. Kniess, R. Bergmann, A. Abrunhosa, I. Santos, A. Paulo, Radiosynthesis and in vivo Evaluation of a 18F- Labelled Styryl-Benzoxazole Derivative for β-Amyloid Targeting, Applied Radiation and Isotopes, http://dx.doi.org/10.1016/j.apradiso.2013.07.003 This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting galley proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain. Radiosynthesis and in vivo Evaluation of a 18F-Labelled Styryl-Benzoxazole Derivative for β-Amyloid Targeting G. Ribeiro Morais,1 L. Gano,1 T. Kniess,2 R. Bergmann,2 A. Abrunhosa,3 I. Santos,1 and A. Paulo1* 1Radiopharmaceutical Sciences Group, IST/ITN, Instituto Superior Técnico, Universidade Técnica de Lisboa, EN 10, 2686-953 Sacavem; 2Institute of Radiopharmacy, Helmholtz-Zentrum Dresden-Rossendorf e.V., POB 510119, D-01314 Dresden, Germany; 3Universidade Coimbra, ICNAS, Inst Nucl Sci Appl Saúde, P-3000 Coimbra, Portugal Corresponding e-mail: [email protected] Keywords: Alzheimer´s Disease/ β-Amyloid aggregation/ Molecular Imaging / Fluorine-18 Abstract The formation of β-amyloid deposits is considered a histopathological feature of Alzheimer´s disease (AD). -

Investigation Study Radiation Profile on a 20 Gbq Therasphere Dose Vial
Attachment 14 NUCLEAR MEDICINE M Nordion KANATA OPERATIONS INVESTIGATION STUDY PD99099003.08 Page No: I of 4 Investigation Study Radiation Profile on a 20 GBq TheraSphere Dose Vial I Signatures Prepared by: Date: ý - Al -; Approved by:. Date: 2•-O--c "Y (Richard Decaire CAHT) Document History Date Version''• •Comments Prepared by . Reviewed by Approved by PD99099003.08 Page Investigation No: 2 of 4 Study Radiation Profile on a 20 GBq TheraSphere Dose Vial 1. INTRODUCTION The United States Nuclear Regulatory Commission had requested information to support MDS Nordion application for the registration of TheraSphere. This request is contained in a letter dated November 23, 1999 from a Dr John P. Jankovich. This report contains data collected to address question 7 parts a, b, and c. The question poised is as follows: "Regarding external radiation levels, NRC needs information on the device itself, not on the radiation levels around the patient as addressed in the application. Therefore, please specify: a. External radiation levels around the lucite vial containing the maximum dose of 20 GBq (540 mCi). Provide the data, preferably, at the surface, and at 5, 30, and 100 cm. If there are no meaningful readings at these locations, please state so. b. Provide similar external radiation levels, if any, outside the lead pot with the lucite vial inside containing a maximum dose of microspheres. c. Please specify the instrument which you used to perform the radiation profile measurements by listing the instrument manufacturers, model numbers, calibration dates, sensitivity, etc." To address these questions, information was provided from previous development work. -

Myocardial Perfusion Imaging in Coronary Artery Disease
Cor et Vasa Available online at www.sciencedirect.com journal homepage: www.elsevier.com/locate/crvasa Přehledový článek | Review article Myocardial perfusion imaging in coronary artery disease Magdalena Kostkiewicza,b a Department of Cardiovascular Diseases, Jagiellonian University, Collegium Medicum, Hospital John Paul II, Krakow, Poland b Department of Nuclear Medicine, Hospital John Paul II, Jagiellonian University, Collegium Medicum, Krakow, Poland ARTICLE INFO SOUHRN Article history: Radionuklidové zobrazování perfuze myokardu (myocardial perfusion imaging, MPI) lze použít k prokázání Received: 22. 8. 2015 přítomnosti ischemické choroby srdeční (ICHS), stratifi kaci rizika i k vedení léčby pacientů s již potvrzeným Received in revised form: 26. 9. 2015 onemocněním. Uvedená metoda je schopna lokalizovat hemodynamicky významné stenózy koronárních Accepted: 28. 9. 2015 tepen i zhodnotit rozsah a závažnost jejich obstrukce podle přítomnosti a rozsahu defektů perfuze. Nor- Available online: 31. 10. 2015 mální výsledek MPI znamená nepřítomnost koronární obstrukce, a tedy i klinicky významného onemocnění. Předností vyšetření srdce metodou PET je oproti SPECT její vyšší prostorové a časové rozlišení i nižší radiační zátěž pacienta. Zdá se, že hybridní vyšetření srdce kombinací SPECT nebo PET s údaji z CT nabízí přesnější Klíčová slova: a spolehlivější diagnostické a prognostické informace o pacientech se středně vysokým rizikem rozvoje ICHS. Ischemická choroba srdeční V poslední době byl zaznamenán významný pokrok ve smyslu přesnější kvantifi kace průtoku krve myokar- PET dem a koronární průtokové rezervy. Několik studií rovněž prokázalo, že kombinace zobrazení apoptózy Radionuklidové zobrazování perfuze a tvorby matrixových metaloproteináz může být prospěšná při zobrazování nestabilních plátů a vyhledání myokardu skupin asymptomatických pacientů s vysokým rizikem, pro něž znamená vyšetření zobrazovací metodou SPECT největší přínos. -

PART I GENERAL PROVISIONS R12 64E-5.101 Definitions
64E-5 Florida Administrative Code Index PART I GENERAL PROVISIONS R12 64E-5.101 Definitions ................................................................................................. I-1 64E-5.102 Exemptions ............................................................................................. I-23 64E-5.103 Records ................................................................................................... I-24 64E-5.104 Tests ... ................................................................................................... I-24 64E-5.105 Prohibited Use ........................................................................................ I-24 64E-5.106 Units of Exposure and Dose ................................................................... I-25 64E-5 Florida Administrative Code Index 64E-5 Florida Administrative Code Index PART II LICENSING OF RADIOACTIVE MATERIALS R2 64E-5.201 ...... Licensing of Radioactive Material .............................................................. II-1 64E-5.202 ...... Source Material - Exemptions .................................................................... II-2 R12 64E-5.203 ...... Radioactive Material Other than Source Material - Exemptions ................. II-4 SUBPART A LICENSE TYPES AND FEES R12 64E-5.204 ..... Types of Licenses ..................................................................................... II-13 SUBPART B GENERAL LICENSES 64E-5.205 ..... General Licenses - Source Material ......................................................... -

3Rd Quarter 2001 Bulletin
In This Issue... Promoting Colorectal Cancer Screening Important Information and Documentaion on Promoting the Prevention of Colorectal Cancer ....................................................................................................... 9 Intestinal and Multi-Visceral Transplantation Coverage Guidelines and Requirements for Approval of Transplantation Facilities12 Expanded Coverage of Positron Emission Tomography Scans New HCPCS Codes and Coverage Guidelines Effective July 1, 2001 ..................... 14 Skilled Nursing Facility Consolidated Billing Clarification on HCPCS Coding Update and Part B Fee Schedule Services .......... 22 Final Medical Review Policies 29540, 33282, 67221, 70450, 76090, 76092, 82947, 86353, 93922, C1300, C1305, J0207, and J9293 ......................................................................................... 31 Outpatient Prospective Payment System Bulletin Devices Eligible for Transitional Pass-Through Payments, New Categories and Crosswalk C-codes to Be Used in Coding Devices Eligible for Transitional Pass-Through Payments ............................................................................................ 68 Features From the Medical Director 3 he Medicare A Bulletin Administrative 4 Tshould be shared with all General Information 5 health care practitioners and managerial members of the General Coverage 12 provider/supplier staff. Hospital Services 17 Publications issued after End Stage Renal Disease 19 October 1, 1997, are available at no-cost from our provider Skilled Nursing Facility -

Nrc Regulatory Issue Summary 2005-23 Clarification of the Physical Presence Requirement During Gamma Stereotactic Radiosurgery Treatments
UNITED STATES NUCLEAR REGULATORY COMMISSION OFFICE OF NUCLEAR MATERIAL SAFETY AND SAFEGUARDS WASHINGTON, D.C. 20555 October 7, 2005 NRC REGULATORY ISSUE SUMMARY 2005-23 CLARIFICATION OF THE PHYSICAL PRESENCE REQUIREMENT DURING GAMMA STEREOTACTIC RADIOSURGERY TREATMENTS ADDRESSEES All gamma stereotactic radiosurgery (GSR) licensees. INTENT The U.S. Nuclear Regulatory Commission (NRC) is issuing this regulatory issue summary (RIS) to clarify the definition of the term “physically present,” as used in 10 CFR 35.615(f)(3). No specific action or written response is required. BACKGROUND In March 2005, during a licensing visit to a GSR facility, the NRC staff observed that the authorized medical physicist (AMP) did not remain physically present throughout one of the GSR treatments, as required by 10 CFR 35.615(f)(3). Instead, during the treatment, the AMP walked to the other end of the GSR suite and entered a treatment planning room located more than 30.5 meters (100 feet) away from the GSR treatment console. While discussing this incident with the licensee, the NRC staff recognized that the licensee was misinterpreting the physical presence requirement for GSR treatments. Based on the licensee’s interpretation of the regulations, the licensee considered any location within the GSR suite, including the treatment planning room, to be within hearing distance of normal voice from the GSR treatment console. The licensee believed that, within the contiguous boundary of its GSR suite, the human voice has sufficient volume, without electronic amplification, to alert the AMP of an emergency at essentially any location within its suite and the AMP could respond in a timely manner. -
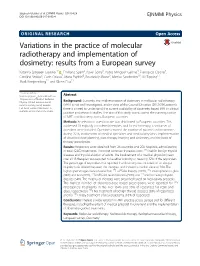
Variations in the Practice of Molecular Radiotherapy and Implementation Of
Sjögreen Gleisner et al. EJNMMI Physics (2017) 4:28 EJNMMI Physics DOI 10.1186/s40658-017-0193-4 ORIGINAL RESEARCH Open Access Variations in the practice of molecular radiotherapy and implementation of dosimetry: results from a European survey Katarina Sjögreen Gleisner1* , Emiliano Spezi2, Pavel Solny3, Pablo Minguez Gabina4, Francesco Cicone5, Caroline Stokke6, Carlo Chiesa7, Maria Paphiti8, Boudewijn Brans9, Mattias Sandström10, Jill Tipping11, Mark Konijnenberg12 and Glenn Flux13 * Correspondence: [email protected] Abstract 1Department of Medical Radiation Physics, Clinical Sciences Lund, Background: Currently, the implementation of dosimetry in molecular radiotherapy Lund University, Lund, Sweden (MRT) is not well investigated, and in view of the Council Directive (2013/59/Euratom), Full list of author information is there is a need to understand the current availability of dosimetry-based MRT in clinical available at the end of the article practice and research studies. The aim of this study was to assess the current practice of MRT and dosimetry across European countries. Methods: An electronic questionnaire was distributed to European countries. This addressed 18 explicitly considered therapies, and for each therapy, a similar set of questions were included. Questions covered the number of patients and treatments during 2015, involvement of medical specialties and medical physicists, implementation of absorbed dose planning, post-therapy imaging and dosimetry, and the basis of therapy prescription. Results: Responses were obtained from 26 countries and 208 hospitals, administering in total 42,853 treatments. The most common therapies were 131I-NaI for benign thyroid diseases and thyroid ablation of adults. The involvement of a medical physicist (mean over all 18 therapies) was reported to be either minority or never by 32% of the responders. -

Radiosurgery Or Fractionated Stereotactic Radiotherapy Plus Whole-Brain Radioherapy in Brain Oligometastases: a Long-Term Analysis
ANTICANCER RESEARCH 35: 3055-3060 (2015) Radiosurgery or Fractionated Stereotactic Radiotherapy plus Whole-brain Radioherapy in Brain Oligometastases: A Long-term Analysis MARIO BALDUCCI1, ROSA AUTORINO1, SILVIA CHIESA1, GIANCARLO MATTIUCCI1, ANGELO POMPUCCI2, LUIGI AZARIO3, GIUSEPPE ROBERTO D’AGOSTINO1, MILENA FERRO1, ALBA FIORENTINO1, SERGIO FERSINO1, CIRO MAZZARELLA1, CESARE COLOSIMO4, VINCENZO FRASCINO1, CARMELO ANILE2 and VINCENZO VALENTINI1 Departments of 1Radiation Oncology, 2Neurosurgery, 3Physics and 4Radiology, Catholic University of the Sacred Heart, Rome, Italy Abstract. Aim: To analyze the outcome of patients with number, size, location, the patient’s Karnofsky performance brain oligometastases treated by radiosurgery (SRS) or status (KPS), age, extent of systematic disease and primary fractionated stereotactic radiotherapy (FSRT) after whole- disease status (4, 5). brain radiotherapy (WBRT). Patients and Methods: Overall Patients with one or two brain metastases and with survival (OS) and local control (LC) were evaluated in favorable prognostic features have a relatively favorable patients (patients) with 1-2 brain metastases. Results: Forty- survival; thus, the treatment is frequently more aggressive seven patients were selected. They were submitted to WBRT than for patients with multiple brain metastases (5). (median dose=3,750 cGy) followed by SRS (17 patients; Radiosurgery (SRS) delivered as a single fraction to median dose=1,500 cGy) or FSRT (30 patients; median individual intracranial lesions has been the most common dose=2,000 cGy). Median follow-up was 102 months technique used to dose-escalate on lesions following whole (range=17-151); the median survival was 22 months for the brain radiotherapy (WBRT) and considered as safe SRS group and 16 months for the FSRT group. -

Implantable Beta-Emitting Microspheres for Treatment of Malignant Tumors
UnitedHealthcare® Commercial Medical Policy Implantable Beta-Emitting Microspheres for Treatment of Malignant Tumors Policy Number: 2021T0445S Effective Date: August 1, 2021 Instructions for Use Table of Contents Page Related Commercial Policy Coverage Rationale ........................................................................... 1 • Abnormal Uterine Bleeding and Uterine Fibroids Documentation Requirements......................................................... 1 Definitions ........................................................................................... 2 Community Plan Policy Applicable Codes .............................................................................. 2 • Implantable Beta-Emitting Microspheres for Treatment of Malignant Tumors Description of Services ..................................................................... 3 Clinical Evidence ............................................................................... 3 Medicare Advantage Coverage Summary U.S. Food and Drug Administration ..............................................15 • Brachytherapy Procedures References .......................................................................................15 Policy History/Revision Information..............................................18 Instructions for Use .........................................................................19 Coverage Rationale Transarterial radioembolization (TARE) using yttrium-90 (90Y) microspheres is proven and medically necessary for the following: • When used -

Of Richard Martin on Yttrium-90 Microsphere Brachytherapy
Page 1 of 1 As of: 2/8/18 2:05 PM Received: February 08, 2018 Status: Pending~Post PUBLIC SUBMISSION Tracking No. lk2-91du-ys8n Comments Due: February 08, 2018 Submission Type: Web Docket: NRC-2017-0215 Yttrium-90 Microsphere Brachytherapy Sources and Devices Therasphere and SIR-Spheres Comment On: NRC-2017-0215-0024 Yttrium-90 Microsphere Brachytherapy Sources and Devices TheraSphere and SIR-Spheres; Draft Guidance; Extension of Comment Period Document: NRC-2017-0215-DRAFT-0132 Comment on FR Doc# 2017-28271 Submitter Information Name: Richard Martin Organization: American Association of Physicists in Medicine General Comment See attached file(s) Attachments AAPM Comment NRC Y-90 Guidance Final RM SUNSI Review Complete Template= ADM - 013 E-RIDS= ADM-03 · Add= l.1 SCA.\), m )11 1lJ:. C) lch) K~~-t.ri11"1 MP.P ( Kris!) https://www.fdms.gov/fdms/getcontent?objectld=0900006482f01e40&format=xml&showorig=false 02/08/2018 ''l, :~:~~.::. ' ••• ·: ·.~ ••~ ~ •'<",• ··:. : •• · 1 • ~ • • • • • ' • • • j db AMERICAN ASSOCIATION ~l7ef PHYSICISTS IN MEDICINE February 8, 2018 May Ma Office of Administration Mail Stop: OWFN-2-A13 U.S. Nuclear Regulatory Commission Washington, DC 20555-0001 RE: Request for Comment: Yttrium-90 Microsphere Brachytherapy Sources and Devices TheraSphere and SIR-Spheres Draft Guidance (NRC-2017-0215) Dear Ms. Ma: The American Association of Physicists in Medicine (AAPM)1 is pleased to submit comments to the U.S. Nuclear Regulatory Commission (NRC) regarding Yttrium-90 Microsphere Brachytherapy Sources and Devices TheraSphere and SIR-Spheres Draft Licensing Guidance (Revision 10). The AAPM commends the NRC on its work in providing the NRC with a set of standard criteria for evaluating a medical use license application for the use of TheraSpheres and SIR-Spheres. -

Anew Drug Design Strategy in the Liht of Molecular Hybridization Concept
www.ijcrt.org © 2020 IJCRT | Volume 8, Issue 12 December 2020 | ISSN: 2320-2882 “Drug Design strategy and chemical process maximization in the light of Molecular Hybridization Concept.” Subhasis Basu, Ph D Registration No: VB 1198 of 2018-2019. Department Of Chemistry, Visva-Bharati University A Draft Thesis is submitted for the partial fulfilment of PhD in Chemistry Thesis/Degree proceeding. DECLARATION I Certify that a. The Work contained in this thesis is original and has been done by me under the guidance of my supervisor. b. The work has not been submitted to any other Institute for any degree or diploma. c. I have followed the guidelines provided by the Institute in preparing the thesis. d. I have conformed to the norms and guidelines given in the Ethical Code of Conduct of the Institute. e. Whenever I have used materials (data, theoretical analysis, figures and text) from other sources, I have given due credit to them by citing them in the text of the thesis and giving their details in the references. Further, I have taken permission from the copyright owners of the sources, whenever necessary. IJCRT2012039 International Journal of Creative Research Thoughts (IJCRT) www.ijcrt.org 284 www.ijcrt.org © 2020 IJCRT | Volume 8, Issue 12 December 2020 | ISSN: 2320-2882 f. Whenever I have quoted written materials from other sources I have put them under quotation marks and given due credit to the sources by citing them and giving required details in the references. (Subhasis Basu) ACKNOWLEDGEMENT This preface is to extend an appreciation to all those individuals who with their generous co- operation guided us in every aspect to make this design and drawing successful. -
A Roadmap for Replacing High-Risk Radioactive Sources and Materials
1 Permanent Risk Reduction: A Roadmap for Replacing High-Risk Radioactive Sources and Materials Miles A. Pomper James Martin Center for Nonproliferation Studies The National Academies of Sciences Radioactive Sources: Applications and Alternative Technologies Meeting January 31, 2020 2 Overview • CNS Workshops and Studies • Materials of Security Concern • Uses of Current High-Risk Materials ▫ Medicine ▫ Oil and gas industry • Strategy for Replacing High Activity Sources • Replacement Priority • Encouraging Replacement: Actions • Conclusions 3 CNS Workshops and Studies Since 2008, CNS has led a series of workshops and studies: . Alternatives to High-Risk Radiological Sources: The Case of Cesium Chloride in Blood Irradiation (2014) . Permanent Risk Reduction: A Roadmap for Replacing High-Risk Radioactive Sources and Materials (2015) . Treatment Not Terror: Strategies to Enhance External Beam Cancer Therapy in Developing Countries While Permanently Reducing the Risk of Radiological Terrorism (2016) . Additional material since: for NYC, NTI, and IAEA ICONS, draft language for 2016 NSS 4 Important Current Uses for High-Risk Materials, Existing Alternatives and Challenges, and Suggested Next Steps 5 High-Risk Sources • A task force report by the NRC listed 1. Americium-241 (Am-241) 2. Am-241/Beryllium (Be) 16 radionuclides as those of principal 3. Californium-252 (Cf-252) concern when considering the 4. Cesium-137 (Cs-137) problems they would cause if used in a 5. Cobalt-60 (Co-60) radiological dispersion device (RDD) 6. Curium-244 (Cm-244) • Considered an immediate danger only 7. Gadolinium-153 (Gd-153) when found in large enough amounts 8. Iridium-192 (Ir-192) to threaten life or cause severe 9.