SJH Procedures
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Table 1 Table 2 Table 3 Table 4 Colonoscopy-Related Costs
Digestive Health Network, Inc. List of Tables Top 10 Physician Specialties Performing Colonoscopies, Medicare Fee-for- Table 1 Service, 2015 Colonoscopy-related Costs, Medicare Fee-for-Service Beneficiaries who Table 2 Received a Screening or Diagnostic Colonoscopy, 2015 Colonoscopy-related Costs, Medicare Fee-for-Service Beneficiaries who Table 3 Received a Colonoscopy in an Ambulatory Surgical Center (ASC), Hospital Outpatient Department, or Physician Office, 2015 Proportion of Medicare Fee-for-Service Medicare Beneficiaries who Received Table 4 a Colonoscopy and were Treated in the Emergency Department within 7 Days of the procedure, 2015 Digestive Health Network, Inc. Responses to Questions Among Medicare beneficiaries, how many colonoscopies are performed in the US, by type of Q1 physician? Nearly 2 million screening and diagnostic colonoscopies were performed in 2015. Of these, over 78% were performed by a gastroenterologist. Nearly 10% were performed by a general surgeon and about 6% were performed by an internal medicine specialist. These results are shown in Table 1. Q2 What proportion of spending on colonoscopies is accounted for by physician services? In 2015, Medicare expenditures associated with colonoscopies totaled over $1.3 billion. (This excludes anesthesiology, pathology, radiology, and other costs identified in Table 2.) Approximately 31% of this amount, or $416 million was associated with professional fees. Q3 What share of Part B Medicare spending is accounted for by colonoscopies? Medicare Part B expenditures in 2015 totaled over $131 billion (data not shown). Colonoscopy costs accounted for approximately 1.03% of this total. Q4 What are the costs associated with colonoscopies for the different settings of care? Costs associated with colonoscopies in ambulatory surgical centers (ASC), hospital outpatient departments (HOPD), and physician offices are shown in Table 3. -

Laparoscopic Truncal Vagotomy and Gatrojejunostomy for Pyloric Stenosis
ORIGINAL ARTICLE pISSN 2234-778X •eISSN 2234-5248 J Minim Invasive Surg 2015;18(2):48-52 Journal of Minimally Invasive Surgery Laparoscopic Truncal Vagotomy and Gatrojejunostomy for Pyloric Stenosis Jung-Wook Suh, M.D.1, Ye Seob Jee, M.D., Ph.D.1,2 Department of Surgery, 1Dankook University Hospital, 2Dankook University School of Medicine, Cheonan, Korea Purpose: Peptic ulcer disease (PUD) remains one of the most prevalent gastrointestinal diseases and Received January 27, 2015 an important target for surgical treatment. Laparoscopy applies to most surgical procedures; however Revised 1st March 9, 2015 its use in elective peptic ulcer surgery, particularly in cases of pyloric stenosis, has not been popular. 2nd March 28, 2015 The aim of this study was to describe the role of laparoscopic surgery and an easily performed Accepted April 20, 2015 procedure for pyloric stenosis. We accordingly performed laparoscopic truncal vagotomy with gastrojejunostomy in 10 consecutive patients with pyloric stenosis. Corresponding author Ye Seob Jee Methods: Data were collected prospectively from all patients who underwent laparoscopic truncal Department of Surgery, Dankook vagotomy with gastrojejunostomy from August 2009 to May 2014 and reviewed retrospectively. University Hospital, Dankook Results: A total of 10 patients underwent laparoscopic trucal vagotomy with gastrojejunostomy for University School of Medicine, 119, peptic ulcer obstruction from August 2009 to May 2014 in ○○ university hospital. The mean age was Dandae-ro, Dongnam-gu, Cheonan 62.6 (±16.4) years old and mean BMI was 19.3 (±2.5) kg/m2. There were no conversions to open 330-714, Korea surgery and no occurrence of intra-operative complications. -

Utility of the Digital Rectal Examination in the Emergency Department: a Review
The Journal of Emergency Medicine, Vol. 43, No. 6, pp. 1196–1204, 2012 Published by Elsevier Inc. Printed in the USA 0736-4679/$ - see front matter http://dx.doi.org/10.1016/j.jemermed.2012.06.015 Clinical Reviews UTILITY OF THE DIGITAL RECTAL EXAMINATION IN THE EMERGENCY DEPARTMENT: A REVIEW Chad Kessler, MD, MHPE*† and Stephen J. Bauer, MD† *Department of Emergency Medicine, Jesse Brown VA Medical Center and †University of Illinois-Chicago College of Medicine, Chicago, Illinois Reprint Address: Chad Kessler, MD, MHPE, Department of Emergency Medicine, Jesse Brown Veterans Hospital, 820 S Damen Ave., M/C 111, Chicago, IL 60612 , Abstract—Background: The digital rectal examination abdominal pain and acute appendicitis. Stool obtained by (DRE) has been reflexively performed to evaluate common DRE doesn’t seem to increase the false-positive rate of chief complaints in the Emergency Department without FOBTs, and the DRE correlated moderately well with anal knowing its true utility in diagnosis. Objective: Medical lit- manometric measurements in determining anal sphincter erature databases were searched for the most relevant arti- tone. Published by Elsevier Inc. cles pertaining to: the utility of the DRE in evaluating abdominal pain and acute appendicitis, the false-positive , Keywords—digital rectal; utility; review; Emergency rate of fecal occult blood tests (FOBT) from stool obtained Department; evidence-based medicine by DRE or spontaneous passage, and the correlation be- tween DRE and anal manometry in determining anal tone. Discussion: Sixteen articles met our inclusion criteria; there INTRODUCTION were two for abdominal pain, five for appendicitis, six for anal tone, and three for fecal occult blood. -

Thoracoscopic Truncal Vagotomy Versus Surgical Revision of the Gastrojejunal Anastomosis for Recalcitrant Marginal Ulcers
Surgical Endoscopy (2019) 33:607–611 and Other Interventional Techniques https://doi.org/10.1007/s00464-018-6386-7 2018 SAGES ORAL DYNAMIC Thoracoscopic truncal vagotomy versus surgical revision of the gastrojejunal anastomosis for recalcitrant marginal ulcers Alicia Bonanno1 · Brandon Tieu2 · Elizabeth Dewey1 · Farah Husain3 Received: 1 May 2018 / Accepted: 10 August 2018 / Published online: 21 August 2018 © Springer Science+Business Media, LLC, part of Springer Nature 2018 Abstract Introduction Marginal ulcer is a common complication following Roux-en-Y gastric bypass with incidence rates between 1 and 16%. Most marginal ulcers resolve with medical management and lifestyle changes, but in the rare case of a non-healing marginal ulcer there are few treatment options. Revision of the gastrojejunal (GJ) anastomosis carries significant morbidity with complication rates ranging from 10 to 50%. Thoracoscopic truncal vagotomy (TTV) may be a safer alternative with decreased operative times. The purpose of this study is to evaluate the safety and effectiveness of TTV in comparison to GJ revision for treatment of recalcitrant marginal ulcers. Methods A retrospective chart review of patients who required surgical intervention for non-healing marginal ulcers was performed from 1 September 2012 to 1 September 2017. All underwent medical therapy along with lifestyle changes prior to intervention and had preoperative EGD that demonstrated a recalcitrant marginal ulcer. Revision of the GJ anastomosis or TTV was performed. Data collected included operative time, ulcer recurrence, morbidity rate, and mortality rate. Results Twenty patients were identified who underwent either GJ revision (n = 13) or TTV (n = 7). There were no 30-day mortalities in either group. -

Small Bowel Obstruction After Laparoscopic Roux-En-Y Gastric Bypass Presenting As Acute Pancreatitis: a Case Report
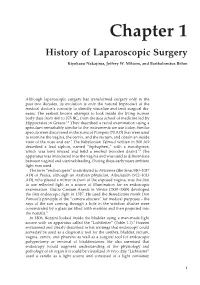
Netherlands Journal of Critical Care Submitted January 2018; Accepted April 2018 CASE REPORT Small bowel obstruction after laparoscopic Roux-en-Y gastric bypass presenting as acute pancreatitis: a case report N. Henning1, R.K. Linskens2, E.E.M. Schepers-van der Sterren3, B. Speelberg1 Department of 1Intensive Care, 2Gastroenterology and Hepatology, and 3Surgery, Sint Anna Hospital, Geldrop, the Netherlands. Correspondence N. Henning - [email protected] Keywords - Roux-en-Y, gastric bypass, pancreatitis, pancreatic enzymes, small bowel obstruction, biliopancreatic limb obstruction. Abstract Small bowel obstruction is a common and potentially life-threatening bowel obstruction within this complication after laparoscopic Roux-en-Y gastric bypass surgery. population, because misdiagnosis We describe a 30-year-old woman who previously underwent can have disastrous outcomes.[1,3-5,7] gastric bypass surgery. She was admitted to the emergency In this report we describe the department with epigastric pain and elevated serum lipase levels. difficulty of diagnosing small Conservative treatment was started for acute pancreatitis, but she bowel obstruction in post- showed rapid clinical deterioration due to uncontrollable pain and LRYGB patients and why frequent excessive vomiting. An abdominal computed tomography elevated pancreatic enzymes scan revealed small bowel obstruction and surgeons performed can indicate an obstruction in an exploratory laparotomy with adhesiolysis. Our patient quickly these patients. The purpose of improved after surgery and could be discharged home. This case this manuscript is to emphasise report emphasises that in post-bypass patients with elevated Figure 1. Roux-en-Y gastric bypass that in post-bypass patients with pancreatic enzymes, small bowel obstruction should be considered ©Ethicon, Inc. -

An Unusual Presentation of Spigelian Hernia Incarceration After Colonoscopy
Open Access Case Report DOI: 10.7759/cureus.3317 An Unusual Presentation of Spigelian Hernia Incarceration after Colonoscopy Vincent M. Pronesti 1 , Clara Antoury 2 , Ricardo Mitre 2 1. Department of Internal Medicine, Allegheny Health Network, Pittsburgh, USA 2. Department of Gastroenterology, Allegheny Health Network, Pittsburgh, USA Corresponding author: Vincent M. Pronesti, [email protected] Abstract Spigelian hernias are uncommon and predominantly affect the abdominal wall. The incidence of Spigelian hernias after colonoscopy is even rarer with only one case outlined in the surgical literature. This is the case of a 66-year-old man who underwent routine colonoscopy and presented to the hospital with systemic inflammatory response syndrome (SIRS). A computed tomography (CT) scan demonstrated a Spigelian hernia in the location of a prior left ventricular assist device (LVAD) placement. This required surgical resection and resulted in a complicated post-operative course. This case offers a unique perspective on a rare colonoscopic complication not well represented in the literature. It offers the learning point of remaining vigilant for a rare, but potentially deadly, colonoscopic outcome. This case also illustrates the decision-making heuristic of availability bias. Categories: Emergency Medicine, Internal Medicine, Gastroenterology Keywords: spigelian hernia, colonoscopy, systemic inflammatory response syndrome (sirs), bowel incarceration, colonic resection, left ventricular assist device Introduction Clinicians must be aware of potential rare complications after colonoscopy. This is particularly relevant because every patient is advised to get a screening colonoscopy at age 50, making this an exceedingly common procedure. Spigelian hernias are rare and comprise approximately 0.12% of hernias of the abdominal wall [1]. -

High Resolution Anoscopy Overview
High Resolution Anoscopy Overview Naomi Jay, RN, NP, PhD University of California San Francisco Email: [email protected] Disclosures No Disclosures Definition of HRA Examination of the anus, anal canal and perianus using a colposcope with 5% acetic acid and Lugol’s solution. Basic Principles • Office-based procedure • Adapted from gynecologic colposcopy. • Validated for anal canal. • Similar terminology and descriptors. may be unfamiliar to non-gyn providers. • Comparable to vaginal and vulvar colposcopy. • Clinicians familiar with cervical colposcopy may be surprised by the difficult transition. Anal SCJ & AnTZ • Original vs. current SCJ less relevant. • TZ features less common, therefore more difficult to appreciate. • SCJ more subtle, difficult to see in entirety requires more manipulation & acetic acid. • Larger area of metaplastic changes overlying columnar epithelium compared to endocervix. • Most lesions found in the AnTZ. Atypical Metaplasia • Atypical metaplasia may indicate the presence of HSIL. • Radiate over distal rectum from SCJ. • Thin, may wipe off. • Features to look for indicating potential lesions: • Atypical clustered glands (ACG) • Lacy metaplastic borders (LM) • Epithelial Honeycombing (EH) Lugol’s. Staining • More utility in anus compared to cervix. • Adjunctive to help define borders, distinguish between possible LSIL/HSIL. • Most HSIL will be Lugol’s negative • LSIL may be Lugol’s partial or negative • Applied focally with small cotton swabs to better define an acetowhite lesion. •NOT a short cut to determine presence or absence of lesions, acetic acid is used first and is applied frequently. Anal vs. Cervical Characteristics • Punctation & Mosaic rarely “fine” mostly “coarse”. • Mosaic pattern mostly associated with HSIL. • Atypical vessels may be HSIL or cancer • Epithelial honeycombing & lacy metaplasia unique anal descriptors. -

1311 Diploma in Medical Record Science Second
[LD 0212] AUGUST 2013 Sub. Code: 1311 DIPLOMA IN MEDICAL RECORD SCIENCE SECOND YEAR PAPER II – INTERNATIONAL CLASSIFICATION OF DISEASES (ICD-10) & SURGICAL PROCEDURES (ICM-9CM) Q.P. Code : 841311 Time : Three Hours Maximum : 100 marks Answer ALL questions I Write appropriate codes using ICD -10 (30 x 1 = 30) 1. Therapeutic introduction of hand tendon. 2. Excision of major partial thickness of eyelid excision. 3. Interphalangeal arthrodesis of Toe. 4. Division of percutaneous spinal cord nerve tracts. 5. Transfusion of allograft bone aetriosus. 6. Rastelli operation of truncus arteriosus. 7. Pyoloric sphincter dilatation. 8. Stapling of radius epiphyseal plate. 9. Suture of hands fascia. 10. Suture of hand fascia. 11. Repair of anterior wall (abdomen) hernia. 12. Foreign body removal without incision in t o the brain. 13. Repair of Tetrology of fallot. 14. Frontal Sinusectomy. 15. Urethral sling suspension. 16. Bone shaft transfer. 17. Coil of aneuryum repair. 18. Sling suspension. 19. Radio isotope scanning, pituitary gland. 20. Spinal shunt removal. 21. Acute lung edema. Due to external agent. 22. Proximal end tibial closed fracture was riding a two wheeler-slip & fell down. 23. Thrombosed internal hemorrhoids. 24. Secondary hypertension due to renal disorder. 25. Old myocardial infarction. 26. Fall from high place, injured elbow. 27. Chronic venous (peripheral) insufficiency. 28. Acute myeloid leukemia. 29. Post-operative intestine obstruction. 30. Abnormal pregnancy. II Writes appropriate codes using ICS-9CM (20 x 2 = 40) 1. Pregnant women suffering from acute salphingo oophoritis. 2. Accidental intake of ferrous salt. 3. Sprain of lumbar spine as stuck by another person. 4. -

Submitted in Partial Fulfillment for MD DEGREE EXAMINATION BRANCH
MDCT EVALUATION OF NON-TRAUMATIC ACUTE ABDOMEN Submitted in partial fulfillment for M.D. DEGREE EXAMINATION BRANCH - VIII , RADIO DIAGNOSIS COIMBATORE MEDICAL COLLEGE AND HOSPITAL COIMBATORE – 14 Dissertation submitted to THE TAMILNADU Dr.M.G.R. MEDICAL UNIVERSITY CHENNAI – 600 032 TAMILNADU APRIL 2017 1 CERTIFICATE This dissertation titled “MDCT EVALUATION OF NON- TRAUMATIC ACUTE ABDOMEN” is submitted to The Tamilnadu Dr.M.G.R Medical University, Chennai, in partial fulfillment of regulations for the award of M.D. Degree in Radio Diagnosis in the examinations to be held during April 2017. This dissertation is a record of fresh work done by the candidate Dr. P. P. BALAMURUGAN, during the course of the study (2014 - 2017). This work was carried out by the candidate himself under my supervision. GUIDE: Dr.N.MURALI, M.D.RD, Professor & HOD, Department of Radio Diagnosis, Coimbatore Medical College, Coimbatore – 14 HEAD OF THE DEPARTMENT: Dr.N.MURALI, M.D.RD, Professor & HOD Department of Radio Diagnosis, Coimbatore Medical College, Coimbatore – 14 2 DEAN: Dr. A. EDWIN JOE, M.D, BL., Dean, Coimbatore Medical College and Hospital, Coimbatore – 14. 3 4 5 6 DECLARATION I, Dr. P.P. Balamurugan, solemnly declare that the dissertation titled “MDCT EVALUATION OF NON-TRAUMATIC ACUTE ABDOMEN” was done by me at Coimbatore Medical College, during the period from July 2015 to August 2016 under the guidance and supervision of Dr. N. Murali, M.D.RD, Professor, Department of Radio Diagnosis, Coimbatore Medical College, Coimbatore. This dissertation is submitted to the Tamilnadu Dr.M.G.R. Medical University towards the partial fulfillment of the requirement for the award of M.D. -

Flexible Sigmoidoscopy in Asymptomatic Patients with Negative Fecal Occult Blood Tests Joy Garrison Cauffman, Phd, Jimmy H
Flexible Sigmoidoscopy in Asymptomatic Patients with Negative Fecal Occult Blood Tests Joy Garrison Cauffman, PhD, Jimmy H. Hara, MD, Irving M. Rasgon, MD, and Virginia A. Clark, PhD Los Angeles, California Background. Although the American Cancer Society and tients with lesions were referred for colonoscopy; addi others haw established guidelines for colorectal cancer tional lesions were found in 14%. A total of 62 lesions screening, questions of who and how to screen still exist. were discovered, including tubular adenomas, villous Methods. A 60-crn flexible sigmoidoscopy was per adenomas, tubular villous adenomas (23 of the adeno formed on 1000 asymptomatic patients, 45 years of mas with atypia), and one adenocarcinoma. The high age or older, with negative fecal occult blood tests, est percentage of lesions discovered were in the sig who presented for routine physical examinations. Pa moid colon and the second highest percentage were in tients with clinically significant lesions were referred for the ascending colon. colonoscopy. The proportion of lesions that would not Conclusions. The 60-cm flexible sigmoidoscope was have been found if the 24-cm rigid or the 30-cm flexi able to detect more lesions than either the 24-cm or ble sigmoidoscope had been used was identified. 30-cm sigmoidoscope when used in asymptomatic pa Results. Using the 60-cm flexible sigmoidoscope, le tients, 45 years of age and over, with negative fecal oc sions were found in 3.6% of the patients. Eighty per cult blood tests. When significant lesions are discovered cent of the significant lesions were beyond the reach of by sigmoidoscopy, colonoscopy should be performed. -
Chapter 1 History of Laparoscopic Surgery
Chapter 1 History of Laparoscopic Surgery Kiyokazu Nakajima, Jeffrey W. Milsom, and Bartholomäus Böhm Although laparoscopic surgery has transformed surgery only in the past two decades, its evolution is only the natural byproduct of the medical doctor’s curiosity to directly visualize and treat surgical dis- eases. The earliest known attempts to look inside the living human body date from 460 to 375 BC, from the Kos school of medicine led by Hippocrates in Greece.1,2 They described a rectal examination using a speculum remarkably similar to the instruments we use today. Similar specula were discovered in the ruins of Pompeii (70 AD) that were used to examine the vagina, the cervix, and the rectum, and obtain an inside view of the nose and ear.1 The Babylonian Talmud written in 500 AD described a lead siphon, named “Siphophert,” with a mouthpiece, which was bent inward and held a mechul (wooden drain).1,3 The apparatus was introduced into the vagina and was used to differentiate between vaginal and uterine bleeding. During these early years ambient light was used. The term “endoscopein” is attributed to Avicenna (Ibn Sina, 980–1037 AD) of Persia, although an Arabian physician, Albulassim (912–1013 AD), who placed a mirror in front of the exposed vagina, was the fi rst to use refl ected light as a source of illumination for an endoscopic examination. Giulio Caesare Aranzi in Venice (1530–1589) developed the fi rst endoscopic light in 1587. He used the Benedictine monk Don Panuce’s principle of the “camera obscura” for medical purposes – the -

Lower Gastrointestinal Tract
Lower Gastrointestinal Tract Hemorrhoids—Office Management and Review for Gastroenterologists Mitchel Guttenplan, MD, FACS 1 and Robert A Ganz, MD, FASGE 2 1. Medical Director, CRH Medical Corp; 2. Minnesota Gastroenterology, Chief of Gastroenterology, Abbott-Northwestern Hospital, Associate Professor of Medicine, University of Minnesota Abstract symptomatic hemorrhoids and anal fissures are very common problems. This article provides a review of the anatomy and physiology of the anorectum along with a discussion of the diagnosis and treatment of hemorrhoids and the commonly associated matters of anal sphincter spasm and fissures. The various office treatment modalities for hemorrhoids are discussed, as are the specifics of rubber band ligation (rBL), and a strategy for the office treatment of these problems by the gastroenterologist is given. The crh o’regan system™ is a technology available to the gastroenterologist that provides a safe, effective, and efficient option for the non-surgical treatment of hemorrhoids in the office setting. Keywords hemorrhoids, anal fissure, rubber band ligation, crh o’regan system™ Disclosure: Mitchel guttenplan is Medical Director of crh Medical Products corporation, the manufacturer of the crh o’regan system™. robert A ganz is a consultant to and holds equity in crh Medical Products corporation. Received: 2 november 2011 Accepted: 30 november 2011 Citation: Touchgastroentorology.com ; December, 2011. Correspondence: Mitchel guttenplan, MD, fAcs, 3000 old Alabama rd, suite 119 #183, Alpharetta, gA 30022-8555, us. e: [email protected] Diseases of the anorectum, including hemorrhoids and anal fissures, are experience also makes it clear that hemorrhoid sufferers frequently very common. The care of these entities is typically left to general and have additional anorectal issues that may both confuse the diagnosis colorectal surgeons.