Laboratory Testing for Chronic Kidney Disease Diagnosis and Management
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Increase of Urinary Putrescine In3,4-Benzopyrene Carcinogenesis
[CANCER RESEARCH 38, 3509-3511, October 1978] 0008-5472/78/0038-0000$02.00 Increase of Urinary Putrescine in 3,4-Benzopyrene Carcinogenesis and Its Inhibition by Putrescine Keisuke Fujita,1 Toshiharu Nagatsu, Kan Shinpo, Kazuhiro Maruta, Hisahide Takahashi, and Atsushi Sekiya Institute for Comprehensive Medical Science ¡K.F., K. S., K. M.], Research Center for Laboratory Animals ¡H.T.¡,and Department of Pharmacology ¡A.S.¡, Fujita-Gakuen University School of Medicine, Toyoake, Aichi 470-11, Japan, and Laboratory of Cell Physiology, Department of Life Chemistry, Graduate School at Nagatsuta, Tokyo Institute of Technology, Yokohama 227, Japan ¡T.N.¡ ABSTRACT were included. Thirty female BALB/c mice, 19 to 20 weeks old and 25 to 30 g body weight, were given s.c. injections of A significant increase in putrescine was noted in the 2.52 mg of 3,4-benzopyrene in 0.5 ml of tricaprylin (Group urine of mice with experimental s.c. tumors induced by a B) or of 2.52 mg of 3,4-benzopyrene plus 10 mg of putres single injection of 3,4-benzopyrene solution (2.52 mg of cine dissolved in 0.5 ml of tricaprylin (Group B + P). As 3,4-benzopyrene in 0.5 ml of tricaprylin). When 10 mg of controls, 30 mice were given injections of 0.5 ml of tricapry putrescine were added to the 3,4-benzopyrene solution, lin (Group C), and 15 mice received 10 mg of putrescine in the development of tumors was completely inhibited and 0.5 ml of tricaprylin (Group P). -

Wellness Labs Explanation of Results
WELLNESS LABS EXPLANATION OF RESULTS BASIC METABOLIC PANEL BUN – Blood Urea Nitrogen (BUN) is a waste product of protein breakdown and is produced when excess protein in your body is broken down and used for energy. BUN levels greater than 50 mg/dL generally means that the kidneys are not functioning normally. Abnormally low BUN levels can be seen with malnutrition and liver failure. Creatinine – a waste product of normal muscle activity. High creatinine levels are most commonly seen in kidney failure and can also been seen with hyperthyroidism, conditions of overgrowth of the body, rhabdomyolysis, and early muscular dystrophy. Low creatinine levels can indicate low muscle mass associated with malnutrition and late-stage muscular dystrophy. Glucose – a simple sugar that serves as the main source of energy in the body. High glucose levels (hyperglycemia) is usually associated with prediabetes and can also occur with severe stress on the body such as surgery or events like stroke or trauma. High levels can also be seen with overactive thyroid, pancreatitis, or pancreatic cancer. Low glucose levels can occur with underactive thyroid and rare insulin- secreting tumors. Electrolytes – Sodium, Calcium, Potassium, Chloride, and Carbon Dioxide are all included in this category. Sodium – high levels of sodium can be seen with dehydration, excessive thirst, and urination due to abnormally low levels of antidiuretic hormone (diabetes insipidus) as well as with excessive levels of cortisol in the body (Cushing syndrome). Low levels of sodium can be seen with congestive heart failure, cirrhosis of the liver, kidney failure, and the syndrome of inappropriate antidiuretic hormone (SIADH). -

Renal Cortical Mitochondrial Transport of Calcium in Chronic Uremia
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Elsevier - Publisher Connector Kidney International, Vol. 34 (1988), pp. 32 7—332 Renal cortical mitochondrial transport of calcium in chronic uremia AvIvA CONFORTY, RUTH SHAINKIN-KESTENBAUM, VARDA SHOSHAN, RINA KOL, JAYSON RAPOPORT, and CIDI0 CHAIM0vITz Departments of Nephrology, Pathology and Biology, Ben-Gurion University of the Negev and Soroka Medical Center, Beer Sheva, Israel Renal cortical mitochondrial transport of calcium in chronic uremia. reduce histologic damage in experimental chronic renal failure Calcium overload of tubular cells may occur in uremia, and may be the in rats [4, 5]. underlying functional abnormality in the continued deterioration of The pathogenic role of cellular overload of calcium as a renal function in chronic renal failure. In order to study this question further, the effect of chronic uremia on the calcium transport properties mediator of cell injury in the kidney has long been recognized and respiratory rates was examined in mitochondria (Mi) isolated from [6—8]. Therefore, it is important to determine if calcium over- the cortex of the remnant kidneys of subtotally nephrectomized rats load of renal cells accompanies the phenomenon of uremic renal (SNX) and sham operated controls (C). Plasma calcium concentration calcification. If, indeed, calcium accumulates in renal cells, it was similar in both groups of rats, but a significant hyperphosphatemia was seen in SNX, 8.60.6 mg%, as compared to 7.20.2 mg% in C could be a contributory factor to the continuing loss of func- (P < 0.001). Mi calcium and phosphate concentrations (nmol/mgtioning nephrons in chronic renal failure. -

The Efficacy and Safety of Six-Weeks of Pre-Workout Supplementation in Resistance Trained Rats
W&M ScholarWorks Undergraduate Honors Theses Theses, Dissertations, & Master Projects 4-2017 The Efficacy and Safety of Six-Weeks of Pre-Workout Supplementation in Resistance Trained Rats Justin P. Canakis College of William and Mary Follow this and additional works at: https://scholarworks.wm.edu/honorstheses Part of the Animal Sciences Commons, Exercise Science Commons, Laboratory and Basic Science Research Commons, and the Other Nutrition Commons Recommended Citation Canakis, Justin P., "The Efficacy and Safety of Six-Weeks of Pre-Workout Supplementation in Resistance Trained Rats" (2017). Undergraduate Honors Theses. Paper 1128. https://scholarworks.wm.edu/honorstheses/1128 This Honors Thesis is brought to you for free and open access by the Theses, Dissertations, & Master Projects at W&M ScholarWorks. It has been accepted for inclusion in Undergraduate Honors Theses by an authorized administrator of W&M ScholarWorks. For more information, please contact [email protected]. 1 2 Title Page……………………………………………………………………………………...…..1 Abstract…………………………………………………………………………………………....5 Acknowledgement……………………………………………………………………….………..6 Background.………………………………………………………………………..……………...7 DSEHA and its Effect on the VMS Industry………………...……………………………7 History of Adverse Side Effects from Pre-Workout Supplements ………….……………8 Ingredient Analysis ………………………………………..……………….……………..……....9 2.5g Beta-Alanine…………………………..……………………………………………..9 1g Creatine Nitrate……………………………...……………………………………..…12 500mg L-Leucine……………………………………………………………………...…16 500mg Agmatine Sulfate……………………….………………………………..………18 -

Profiling of Amino Acids in Urine Samples of Patients Suffering from Inflammatory Bowel Disease by Capillary Electrophoresis-Mass Spectrometry
Article Profiling of Amino Acids in Urine Samples of Patients Suffering from Inflammatory Bowel Disease by Capillary Electrophoresis-Mass Spectrometry Juraj Piestansky 1,2, Dominika Olesova 3, Jaroslav Galba 1, Katarina Marakova 1,2, Vojtech Parrak 3, Peter Secnik 4, Peter Secnik jr. 4, Branislav Kovacech 3, Andrej Kovac 3, Zuzana Zelinkova 5, Peter Mikus 1,2,* 1 Department of Pharmaceutical Analysis and Nuclear Pharmacy, Faculty of Pharmacy, Comenius University in Bratislava, Odbojarov 10, SK-832 32 Bratislava, Slovak Republic; [email protected] (J.P.); [email protected] (J.G.); [email protected] (K.M.); [email protected] (P.M.) 2 Toxicological and Antidoping Center, Faculty of Pharmacy, Comenius University in Bratislava, Odbojárov 10, SK-832 32 Bratislava, Slovak Republic 3 Institute of Neuroimmunology, Slovak Academy of Science, Dubravska cesta 9, SK-845 10, Bratislava, Slovak Republic; [email protected] (D.O.); [email protected] (B.K.); [email protected] (A.K.); [email protected] (V.P.) 4 SK-Lab s.r.o., Partizanska 15, SK-984 01, Lucenec, Slovak Republic; [email protected] (P.S.); [email protected] (P.S. jr.) 5 Department of Gastroenterology, St Michael’s Hospital, Satinskeho 1, SK-811 08 Bratislava, Slovak Republic; [email protected] (Z.Z.) * Correspondence: [email protected]; Tel.: +421-2-50 117 243 (Supplementary Material) Table of content Table S1 Normalized concentrations of amino acids in urine samples from healthy volunteers measured by the CE-MS/MS method. Table S2 Normalized concentrations of amino acids in urine samples from IBD patients undergoing thiopurine treatment measured by the CE-MS/MS method. -

The Efficacy and Safety of Six-Weeks of Pre-Workout Supplementation in Resistance Trained Rats
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by College of William & Mary: W&M Publish W&M ScholarWorks Undergraduate Honors Theses Theses, Dissertations, & Master Projects 4-2017 The Efficacy and Safety of Six-Weeks of Pre-Workout Supplementation in Resistance Trained Rats Justin P. Canakis College of William and Mary Follow this and additional works at: https://scholarworks.wm.edu/honorstheses Part of the Animal Sciences Commons, Exercise Science Commons, Laboratory and Basic Science Research Commons, and the Other Nutrition Commons Recommended Citation Canakis, Justin P., "The Efficacy and Safety of Six-Weeks of Pre-Workout Supplementation in Resistance Trained Rats" (2017). Undergraduate Honors Theses. Paper 1128. https://scholarworks.wm.edu/honorstheses/1128 This Honors Thesis is brought to you for free and open access by the Theses, Dissertations, & Master Projects at W&M ScholarWorks. It has been accepted for inclusion in Undergraduate Honors Theses by an authorized administrator of W&M ScholarWorks. For more information, please contact [email protected]. 1 2 Title Page……………………………………………………………………………………...…..1 Abstract…………………………………………………………………………………………....5 Acknowledgement……………………………………………………………………….………..6 Background.………………………………………………………………………..……………...7 DSEHA and its Effect on the VMS Industry………………...……………………………7 History of Adverse Side Effects from Pre-Workout Supplements ………….……………8 Ingredient Analysis ………………………………………..……………….……………..……....9 2.5g Beta-Alanine…………………………..……………………………………………..9 -

Effects of the Acute Arginine Aspartate Supplement on the Muscular Fatigue
ARTIGO ORIGINAL Efeitos da suplementação aguda de aspartato de arginina na fadiga muscular em voluntários treinados Ricardo Pombo Sales1, Carlos Eduardo César Miné1, Andréia Dellú Franco1, Érika Lima Rodrigues1, Naira Correia Cusma Pelógia2, Renato de Souza e Silva3, José Carlos Cogo1, Rodrigo A.B. Lopes-Martins1, Rodrigo Lazo Osorio1 e Wellington Ribeiro1 RESUMO Palavras-chave: Lactato. Aminoácido. Exaustão. A atividade física influi em mecanismos específicos responsá- Keywords: Lactate. Aminoacid. Exhaustion. veis pela redução da produção de força e conseqüentemente à Palabras-clave: Lactato. Aminoácido. Agotamiento. fadiga. A preocupação em melhorar o desempenho físico tem sido propostos; observamos que estudos dão atenção para reduzir acú- mulos dos metabólitos que diminuem a fadiga durante o exercício cal performance, and we observed that some studies have been físico intenso, usando aminoácidos conhecidos por induzir mudan- focused on the reduction of the metabolites that decrease the ças metabólicas, entre eles a arginina. O presente estudo teve fatigue on intense physical exercising, using aminoacids known como objetivo estudar o efeito da suplementação aguda de aspar- for their properties to induce to metabolic changes, and among tato de arginina em indivíduos sadios treinados submetidos a um these, it is the arginine. The present study had the purpose to protocolo de exaustão em um cicloergômetro. Foram utilizados study the effects of the acute arginine aspartate supplement in 12 indivíduos treinados do sexo masculino, idade de 22,6 ± 3,5 trained healthy individuals submitted to an exhaustion protocol on anos. Realizaram três testes 90 minutos após a administração em ergonomic bicycle. Twelve 22.6 ± 3.5 years old trained individuals dose única do aspartato de arginina ou solução placebo, em um were used in the research. -

Renal Effects of the Serine Protease Inhibitor Aprotinin in Healthy Conscious Mice
www.nature.com/aps ARTICLE OPEN Renal effects of the serine protease inhibitor aprotinin in healthy conscious mice Stefan Wörner1, Bernhard N. Bohnert1,2,3, Matthias Wörn1, Mengyun Xiao1, Andrea Janessa1, Andreas L. Birkenfeld1,2,3, Kerstin Amann4, Christoph Daniel4 and Ferruh Artunc 1,2,3 Treatment with aprotinin, a broad-spectrum serine protease inhibitor with a molecular weight of 6512 Da, was associated with acute kidney injury, which was one of the reasons for withdrawal from the market in 2007. Inhibition of renal serine proteases regulating the epithelial sodium channel ENaC could be a possible mechanism. Herein, we studied the effect of aprotinin in wild- type 129S1/SvImJ mice on sodium handling, tubular function, and integrity under a control and low-salt diet. Mice were studied in metabolic cages, and aprotinin was delivered by subcutaneously implanted sustained release pellets (2 mg/day over 10 days). Mean urinary aprotinin concentration ranged between 642 ± 135 (day 2) and 127 ± 16 (day 8) µg/mL . Aprotinin caused impaired sodium preservation under a low-salt diet while stimulating excessive hyperaldosteronism and unexpectedly, proteolytic activation of ENaC. Aprotinin inhibited proximal tubular function leading to glucosuria and proteinuria. Plasma urea and cystatin C concentration increased significantly under aprotinin treatment. Kidney tissues from aprotinin-treated mice showed accumulation of intracellular aprotinin and expression of the kidney injury molecule 1 (KIM-1). In electron microscopy, electron-dense deposits were observed. There was no evidence for kidney injury in mice treated with a lower aprotinin dose (0.5 mg/day). In conclusion, high doses of aprotinin exert nephrotoxic effects by accumulation in the tubular system of healthy mice, leading to inhibition of proximal tubular 1234567890();,: function and counterregulatory stimulation of ENaC-mediated sodium transport. -

Interpretive Guide
INTERPRETIVE GUIDE Contents INTRODUCTION .........................................................................1 NUTREVAL BIOMARKERS ...........................................................5 Metabolic Analysis Markers ....................................................5 Malabsorption and Dysbiosis Markers .....................................5 Cellular Energy & Mitochondrial Metabolites ..........................6 Neurotransmitter Metabolites ...............................................8 Vitamin Markers ....................................................................9 Toxin & Detoxification Markers ..............................................9 Amino Acids ..........................................................................10 Essential and Metabolic Fatty Acids .........................................13 Cardiovascular Risk ................................................................15 Oxidative Stress Markers ........................................................16 Elemental Markers ................................................................17 Toxic Elements .......................................................................18 INTERPRETATION-AT-A-GLANCE .................................................19 REFERENCES .............................................................................23 INTRODUCTION A shortage of any nutrient can lead to biochemical NutrEval profile evaluates several important biochemical disturbances that affect healthy cellular and tissue pathways to help determine nutrient -

Common Laboratory Tests
Common Laboratory Tests BMP (Basic Metabolic Panel): A BMP is a common blood chemistry test that measures your sugar level, electrolyte balance, and kidney function. CBC (Complete Blood Count): A common blood test that helps determine an individual’s general health status. It evaluates hemoglobin, hematocrit, white blood cells, red blood cells, red blood cell indices, and platelets. It can be used as a tool to help diagnose various conditions, such as anemia, infection, inflammation, bleeding disorder, or leukemia. CMP (Complete Metabolic Panel): A CMP is similar to a BMP, in that it measures your sugar level, electrolyte balance, kidney function, but it also measures liver function. ESR (Erythrocyte Sedimentation Rate): A non-specific blood test that is used to help detect inflammation. It is said to be non-specific because an elevated result often indicates inflammation but does not tell exactly where the inflammation is in the body or what is causing it. It is typically used in conjunction with other testing. Ferritin: A blood test that assesses a person’s iron stores in the body. The test is sometimes ordered with an iron test and a TIBC (Total Iron Binding Capacity) to detect the presence and severity of iron deficiency or iron overload. FT4 (Free Thyroxine): Free T4 is a blood test used to help evaluate thyroid function and diagnose thyroid diseases usually after discovering that the TSH level is abnormal. FT3 (Free Triiodothyronine): Free T3 is a blood test used to assess thyroid function. It is primarily used to help diagnose hyperthyroidism and may be ordered to help monitor treatment of a person with a known thyroid disorder. -
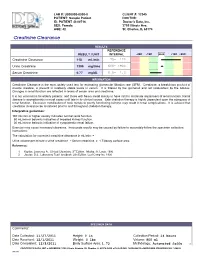
Creatinine Clearance 118 Ml/Min 75- 120
LAB #: U000000-0000-0 CLIENT #: 12345 PATIENT: Sample Patient DOCTOR: ID: PATIENT -S-00716 Doctor's Data, Inc. SEX: Female 3755 Illinois Ave. AGE: 42 St. Charles, IL 60174 !!"#$%&'&'#(!)#$"$'*# RESULTS REFERENCE RESULT / UNIT INTERVAL -2SD -1SD MEAN +1SD +2SD Creatinine Clearance 118 mL/min 75- 120 Urine Creatinine 1300 mg/time 600- 1900 Serum Creatinine 0.77 mg/dL 0.6- 1.3 INFORMATION Creatinine Clearance is the most widely used test for estimating glomerular filtration rate (GFR). Creatinine, a breakdown product of muscle creatine, is present in relatively stable levels in serum. It is filtered by the glomeruli and not reabsorbed by the tubules. Changes in renal function are reflected in levels of serum urea and creatinine. It is not uncommon for elderly patients, and those with heavy metal toxicity to have mild to moderate impairment of renal function. Renal disease is asymptomatic in most cases until late in its clinical course. Safe chelation therapy is highly dependent upon the adequacy of renal function. Excessive mobilization of toxic metals to poorly functioning kidneys may result in renal complications. It is advised that creatinine clearance be monitored prior to and throughout chelation therapy. Interpretive guidelines: 100 mL/min or higher usually indicates normal renal function. 50 mL/min or below is indicative of impaired kidney function. 30 mL/min or below is indicative of symptomatic renal failure. Exercise may cause increased clearance. Inaccurate results may be caused by failure to accurately follow the specimen collection instructions. The calculation for corrected creatinine clearance in mL/min: = Urine volume per minute x urine creatinine ÷ Serum creatinine x 1.73/body surface area References: 1. -

Pneumomediastinum in a Patient with Cannabinoid Hyperemesis Syndrome
IMAGES IN MEDICINE Pneumomediastinum in a Patient with Cannabinoid Hyperemesis Syndrome MARC J. VECCHIO, MD; WILLIAM D. BINDER, MD, FACEP 48 49 EN CASE PRESENTATION Figure 1. (A) Red arrows illustrating extensive pneumomediastinum and pneumo- A 23-year-old man with a past medical retroperitoneum; (B) illustrating air extending into the neck and spinal canal. history of cannabinoid hyperemesis syn- drome presented to the emergency depart- A B ment with 1 week of nausea, emesis and poor oral intake. Prior to presentation, the patient had been treated in the emer- gency department several times for intrac- table vomiting. The patient reported he was a daily long-term user of marijuana cigarettes. On presentation, the patient was afebrile with a pulse of 117 beats per minute, res- pirations of 20 per minute, blood pressure of 111/79 and oxygen saturation of 99% on room air. Physical examination revealed a thin man with eructation and subcutane- ous crepitation over the neck and thorax. Lung sounds were clear to auscultation bilaterally. Laboratory testing revealed a pH of 7.26, anion gap of 33, blood-urea nitrogen of 107 mg/dL and a newly ele- vated creatinine of 13.01 mg/dL. Nota- bly, the patient had normal labs with a creatinine of 0.84 mg/dL during a similar presentation for intractable vomiting one month prior to presentation. Chest X-ray showed evidence of subcutaneous gas and pneumomediastinum. Computed tomog- raphy (CT) of the chest and abdomen with intravenous contrast revealed pneu- momediastinum and pneumoretroperito- neum with extension into the spinal canal (Figure 1).