Implementing TI Program Through Group Approach
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
4Th Week, 2012
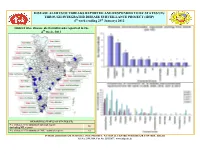
DISEASE ALERTS/OUTBREAKS REPORTED AND RESPONDED TO BY STATES/UTs THROUGH INTEGRATED DISEASE SURVEILLANCE PROJECT (IDSP) th th 4 week (ending 29 January) 2012 District wise disease alerts/outbreaks reported in the 4th week, 2012 REPORTING STATUS OF STATES/UTs No. of States /UTs submitted outbreak report 26 (including NIL report) No. of States/ UTs submitted “NIL” outbreak report 12 INTEGRATED DISEASE SURVEILLANCE PROJECT, NATIONAL CENTRE FOR DISEASE CONTROL, DELHI Tel No. 23913148, Fax No. 23922677; www.idsp.nic.in Sl. Name of Name of Disease/ Illness No. of No. of Date of Date of Current Comments/ Action taken No. State/UT District Cases Deaths start of reporting Status outbreak Clustering of fever cases occurred in Village Srungavruksham, PHC Veervasaram, Narasapuram. Door to door survey done to find new cases. Medical camp conducted to treat cases symptomatically. Andhra Under 1. West Godavari i Dengue 3* 1 23/01/12 29/01/12 Mosquito control measures undertaken. All cases and death tested Pradesh control positive for Dengue (ELISA test and RDT) at Private Nursing Home. IEC activities undertaken regarding early treatment of cases and personal protection measures to be adopted by the community. Outbreak reported from Koloriang village under Kurung Kumey. District RRT visited the affected area and investigated the outbreak. ii Acute Most of the cases were under 5 yrs of age. Active house to house survey Arunachal Kurung Under 2. Diarrhoeal 85 4 27/1/12 29/1/12 conducted to find new cases. All cases treated. ORS packets and Pradesh Kumey control Disease chlorine tablets distributed. IEC activities done regarding personal and surrounding hygiene in the affected area. -

Report of the Comptroller and Auditor General of India STATUS OF
Report of the Comptroller and Auditor General of India STATUS OF ONGOING PROJECTS IN INDIAN RAILWAYS for the year ended March 2014 Laid in Lok Sabha/Rajya Sabha on_____________ Union Government (Railways) No. 48 of 2015 CONTENTS Paragraph Pages List of Abbreviations i to ii Executive Summary iii to ix CHAPTER 1 - Status of Ongoing Projects of Indian Railways- New Lines, Doubling and Gauge Conversion Introduction 1.1 1 Organisation Structure 1.2 2 Audit objectives 1.3 2 Scope and Audit Methodology 1.4 3 Audit Criteria 1.5 3 Audit Findings 1.6 4-35 Conclusion 1.6.14 35 Recommendations 1.6.15 36 CHAPTER 2 - Management of Works Contract in Indian Railways Introduction 2.1 37 Audit Findings 2.2 38-56 Conclusion 2.4 56 Recommendations 2.5 56 CHAPTER 3 - Dedicated Freight Corridor Projects Introduction 3.1 58 About the Project 3.1.1 58 Approval and Planning of the Project 3.2 60 Conclusion 3.4 69 Recommendations 3.5 69 CHAPTER 4 – Modernisation of Signalling and Telecommunication System by Indian Railway Project Management Unit Introduction 4.1 70 Organisation Structure 4.2 72 Audit Findings 4.4 72 Conclusion 4.6 94 Recommendations 4.7 95 APPENDIX Status of Ongoing Projects of Indian Railways- New Lines, Doubling and Gauge Conversion 96-179 Management of Works Contract in Indian Railways 180-181 Modernisation of Signalling and Telecommunication System by Indian Railway Project Management Unit 182-186 ANNEXURE Status of Ongoing Projects of Indian Railways- New Lines, Doubling and Gauge Conversion 187-286 Management of Works Contract in Indian Railways 287-302 Modernisation of Signalling and Telecommunication System by Indian Railway Project Management Unit 303-316 PREFACE This Report for the year ended March 2014 has been prepared for submission to the President of India under Article 151 of the Constitution of India. -

A Case Study of Chitradurga District, in Karnataka
© NOV 2018 | IRE Journals | Volume 2 Issue 5 | ISSN: 2456-8880 Socio-Economic Conditions of Tribal People - A Case Study of Chitradurga District, In Karnataka RANGASWAMY.H.M.A1, Dr. H.H. BHARADI2 1Research Scholar, Ass. Professor in Economics, Gov. Arts College, Karnataka 2Professor in Economics and Research Guide, Dept. of Economics, Karnataka University, Karnataka Abstract -- Chitradurga district is an administrative district ii. The Eastern India: The West Bengal, Bihar, of Karnataka state in southern India the tribal population Orissa. is identified as the aboriginal inhabitants of our country. iii. Central and The West India: Madhya They are seen almost in every State of India. As the name Pradesh, Rajasthan, Gujarat, part of implies, tribes are 'Adivasi' or original dwellers, living in Maharashtra and Northern Andhra Pradesh. the subcontinent. Tribal development aims at increasing the incomes and strengthening the material aspects of iv. Southern India: The Hilly regions of Tamil tribal culture. The folk literature of Kadugollas of Nadu, Kerala, Western and Northern Chitradurga is rich. Folk singers like siriyajji, Eranna of Karnataka and Andhra Pradesh. yaraballi and their contribution is in vogue to day. The inhabitants of hamlets have reposed more confidence in Meaning of 'Tribe' ancestors and elders, and they worship as deities. The tribal community has been giving importance to kinship is a As the name implies, tribes are 'Adivasi' or original practice. The majority of tribal are agriculture labourers, dwellers, living in the subcontinent from unrecorded small farmers and they have shifting of cultivation, but the time and possibly driven into the forests by more cultivation depend upon the rain. -

District Census Handbook, Chitradurga
CENSUS OF INDIA, 1961 MYSORE STATE DISTRICT CENSUS HANDBOOK CHITRADURGA DISTRICT K. BALASUBRAMANYAM OF THE INDIAN ADMINISTRATIVE SERVICE SUPERINTENDENT OF CENSUS OPERATIONS, MYSORE PRINTED AT THE MANIPAL POWER PRESS, MANIPAL (SOUTH KANARA) FOR THE DIRECTOR OF PRINTING, STATIONERY AND PUBLICATIONS, BANGALORE 1967 • -P08ITION or CllffRAIWRfJA DISTRICT III .rlOIlE rrll1r T . DISTRICT MAP OF GH ITRADURGA SCALI , t....it:::i... iii:=O.. iliiiiiiiiiiiiiill1' "'IUS ~ 4 5' 45' -~ <e () ~ ". ..1lI C " '"~'J) III "'.s, ~ 0 I 3(1' -- D Hef,rCl!t~ D;3Ir iC't ~.rJ- flWrt, r 7.. 1"" Villages ~I>ot'e 5(100 P"pgl.ti"n other l"'p"I"unt V'"~I •• ,,,0 T" wns. MMiripalily .I!I (., P"sl orli c~ Police , t.li(", RO./i) Post &- Teleg-rilph officI P.T. ... Travel/us bu~ /o .. TI {) ist rict BOfJfl(jll,.y Q- Ta/uk •• Oivisionil l .. ~ lilli/WilY NlJtiCfl,,1 Hig-h wIIY Stall! other r".ds 0 13° RivrrJ & st re~ms 13 Hills :f;: :':"-"::'-~ ' () rilnb ti PREFACE Census in 'India has all along been a scientific and systematic survey. Gradually through the decades it has also aimed at providing besides a statistical account of the population surveyed, a picture of the Socio-Economic condition of the people. With this end in view, the Census authorities in India have always interested themselves, side by side with the counting of the people, at making several special studies relating to the life of the people. One of these special features of the Census of India at present is the preparation and publication of the District Census Handbooks. -

A1 SYSTEM MAP 2015.Cdr
TO TO TO PUNE (PA) LATUR TO Eó®Ò¨ÉxÉMÉ® ROHA 0.000, 191.590(CST) NANDED nÎIÉhÉ {ÉζSÉ¨É ®ä±É´Éä EóóÉ |ÉhÉɱÉÒ ¨ÉÉxÉÊSÉjÉ DAUND JN.(DD) PARBHANI JN. ÊxÉVÉɨÉɤÉÉn DIVISION 267.180(CST) KARIMNAGAR INDIA NIZAMABAD É N ±ä R ® A SYSTEM MAP =º¨ÉÉxÉɤÉÉn I É L BENGALURU ª W Ò É A i Y ® OSMANABAD S É KURDUWADI JN. (KWV) ¦ OF 376.28(CST) MYSURU BHARAMATI SOUTH WESTERN RAILWAY 310.880(CST) 31-03-2015 iÉE ºÉƶÉÉäÎvÉiÉ è½ÉnÇ We Care We HUBBALLI ÉÆ ºÉÉ Ser XX B´ ve KHED Éä´ÉÉ SOLAPUR (SUR) BIDAR (BIDR) ¨ÉänE º AS ON 31-03-2015 NH 9 ¤ÉÒn® 90.780 BHIMA 454.970, 299.440(GDG) XX RIVER MEDAK BIDAR XX ¶ÉÉä±ÉÉ{ÉÖ® XX HOTGI JN. (HG) NH 7 ºÉiÉÉ®É XX 470.040, 284.090(GDG) NH 65 CHIPLUN SOLAPUR SWR LIMIT AHERWAD I(H) (AHD) 277.100 ENLARGEMENT AT A TO ENLARGEMENT AT C SATARA 282.670 XX MUMBAI SULERJAVALGE (H) (SLGE) 271.520 XX HOSPET JN. (HPT) 143.261, 0.000(GDJ) TORANAGALLU JN. (TNGL) TADWAL (TVL) 264.180 BAYALU VODDIGERI Eó±É¤ÉÙ®MÉÒ SECUNDERABAD JN. (SC) 141.798 (BYO)161.530 175.564, 0.000(RNJP) 257.880 TO XX 194.360 (WADI), 0.000(for GTL) PAPINAYAKANAHALLI BELLARY CANTONMENT MARMAGAO HARBOUR TO HUBLI JN. (PKL)156.510 (MRH) 111.870 KALABURAGI ®ÆMÉÉ®ädÒ 620.650(MMR) DAROJI (BYC) 202.940 MIRAJ ºÉÉÆMɱÉÒ PADNUR (H) (PDNR) 256.300 GADIGANURU (DAJ) 181.270 ¨É½É®É¹]Å XX MUNIRABAD (MRB) 137.290 (GNR)168.470 BELLARY CANTONMENT (H) KONKAN RAILWAY XX ( ) 204.100 XX VASCO-DA-GAMA GULBARGA (GR) RANGAREDDY XX HOSPET BYE PASS LINE LACHYAN (LHN) 251.000 (VSG) 108.458 SANGLI 567.950 2.510 BELLARY JN. -

A Study of Vulnerable Groups in Chitradurga District Study Report - 2010
THE MYRADA EXPERIENCE Including the Excluded A study of Vulnerable Groups in Chitradurga district Study Report-2010 Are SAGs the appropriate institutions to address the needs of the Vulnerable? THE MYRADA EXPERIENCE Including the Excluded A study of Vulnerable Groups in Chitradurga district Study report - 2010 Are SAGs the appropriate institutions to address the needs of the Vulnerable? The Myrada Experience Foreword Including the Excluded The short mission statement which has guided Myrada for the past 25 years is: A study of Vulnerable Groups in Chitradurga district “Building poor peoples institutions”. The Self help Affinity Groups emerged in 1984- 85; these comprised members of poor families identified through participatory Study Report 2010 methods in the village who then formed their own groups by self selecting their members. It soon became clear that these groups provided the basis for the poor members to : i) support the diversity in livelihood strategies of each family which Any part of this report may be used with appropriate acknowledgment included several activities - not just assets which were the only purpose accepted by Government and Banks – including education, health, trading, repayment of high Produced and Published by: cost loans, working capital, for houses, sanitation, skills training, health and similar MYRADA purposes which were their priorities; ii) cope with the changing situation in rural areas No.2, Service Road, where agriculture and related activities are diverse and high risk; ii) access credit Domlur Layout Bangalore - 560 071, INDIA quickly to meet urgent needs iv) gather confidence and skills to influence change in Ph.: 080-2535 2028 / 3166 / 8857 / 4457 / 0090 the family and in society. -

M/S. Vidyavinay Enterprises Taralabalu Nagar,Muttugaduru, Holalkere Taluk, Chitradurga Dist, Karnataka Ph No
M/s. Vidyavinay Enterprises Taralabalu Nagar,Muttugaduru, Holalkere Taluk, Chitradurga Dist, Karnataka Ph No. : +917349289306 Date: 27.05.2017 To, Chairman DEIAA Dept. of Mines & Geology, Mineral, #1948/1, Opposite Anjaneya Temple, Vidya Nagar, Davangere. Dear Sir, Sub: Submission of documents for obtaining Environmental Clearance for “Building Stone Quarry” (QL No. 2209/16-17) over an extent of 4-20 Acres at Sy. No.71 situated in Doddabbigere Village, Channagiri Taluk, Davanagere Dist. Karnataka State . We are herewith submitting the following documents for obtaining the Environmental Clearance for “Building Stone Quarry” (QL No. 2209/16-17) over an extent of 4-20 Acres at Sy. No.71 situated in Doddabbigere Village, Channagiri Taluk, Davanagere Dist. Karnataka State. Form – 1M Pre-feasibility report Environmental Management Plan Approved Mining Plan Processing fee (DD No. ………….. dated ……………, …………………………………………………..) In this regards we kindly request you to grant us the Environmental Clearance for the stone quarry at the earliest. Thanking you Sir, Yours faithfully, for M/s. VIDYAVINAY ENTERPRISES APPENDIX VIII (See paragraph 6) FORM 1 M APPLICATION FOR MINING OF MINERALS UNDER CATEGORY ‘B2’ FOR LESS THAN AND EQUAL TO FIVE HECTARE. (I) Basic Information Sl.No Areas Distance in Kilometer/Details i. Name of the Mining Lease Site Building Stone (Granitic gneisses) Quarry of M/s. Vidyavinay Enterprises QL No. 2209/16-17 ii. Location/Site (GPS Co - Sy No. 71 , Doddabbigere Village, Channagiri Ordinate) Taluk, Davangere District Karnataka. The GPS coordinates of the boundary pillars are given below. BP - 1 N14 010’14.2” & E 76 003’38.8” BP - 2 N14 010’10.1” & E 76 003’38.1” BP - 3 N14 010’07.2” & E 76 003’32.2” BP - 4 N14 010’11.5” & E 76 003’32.9” iii. -

Provisional List of Applicants Who Have Applied for the Post of Task Force Commander Gr-1 (Asst
Page 1 PROVISIONAL LIST OF APPLICANTS WHO HAVE APPLIED FOR THE POST OF TASK FORCE COMMANDER GR-1 (ASST. ENGINEER) Sl.No. Appl Name of Candidate Address Father's Name Date of Qualifica Max Marks Percenta Place of Birth District Caste Category Whether Remarks No Birth tion Marks Obtained ge of Rural/ P.H./ Marks Ex- servicemen/ Lady Candidates 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 1 516 Nayana A S # LIG 291, 22nd Cross, Kuvempunagar, Hassan- Shive Gowda 14-Sep-89 BE(Civil) 6100 5299 86.87 Aladahally Hassan Vokkaliga 3A Lady -- 573201 2 380 Hemalatha M D D/o Doreswamy M, "Sri Lakshmi" Near Nethaji Doreswamy M 24-Sep-89 BE(Civil) 6100 5214 85.48 Hassan Hassan GM GM Lady -- Public School, Ashok Road, Vidyanagar, Hassan- 573201 3 176 Swathi P Gowda C/o K P Krishne Gowda, Siddeshwara Nilaya, Puttaswamy Gowda 22-Aug-88 BE(Civil) 6800 5789 85.13 Alur Hassan Vokkaliga 3A Rural/ Lady -- Near Holy Children School, Jayanagar 1st Block, Hassan-573201 4 569 Mohamed Hussain S/o Noorjahan, #2, Bunder Road, 1st Cross, Ahamed Bawa 11-Jul-87 BE(Civil) 6675 5573 83.49 Bhatkal Karwar Muslim 2B - -- Bhatkal-581320 5 617 Bharath Kumar P K S/o Kumarappa P, New Police Quarters, Hosalli Kumarappa P 3-Mar-89 BE(Civil) 83.30 Kadur Chickamagalur GM 3B - Road, Kadur Tq, Chikkamagalure-577548 6 621 Sushma Mathad #67, "Parvati Nilaya", 4th Main, 7th Cross, Sangayya 12-Jan-90 BE(Civil) 82.90 Chitradurga Chitradurga Lingayath GM Lady -- Gandhinagar, Dharwad-580004 7 513 Sagar S R Kittagalale Village, K Hoskote (P), Alur (T), Ramesh S M 20-Mar-89 BE(Civil) 6800 5623 82.69 Sakelshpur Hassan Vokkaliga 3A Rural -- Hassan (D)-573129. -

RAILWAY BUDGET-2018 HIGHLIGHTS for SOUTH WESTERN RAILWAY Function at Ginigera on 31.03.17
Search : Commercial ,Freight About Us News & Recruitment Tenders Construction Projects Information & Public For IR Personnel Contact Us Information Home QUICK LINKS Bookmark Mail this page Print this page Functions of Railway Minister Select Function at KSR Bengaluru on 15.05.16 Press Release No. 205 Dt. 06.02.2018 07-02-2018 Function at YPR on 23.07.2016 Press Release No. 205, RAILWAY BUDGET-2018 HIGHLIGHTS FOR SOUTH WESTERN RAILWAY Function at Ginigera on 31.03.17 Function at Hubballi & Mysuru on 23.05.2017 Function at YPR on 26.03.2017 News & Announcements Announcements SOUTH WESTERN RAILWAY Press Releases Recruitment Press Release No. 205 Dt. 06.02.2018 By RRB Active Recruitment on SW Rly RAILWAY BUDGET-2018 HIGHLIGHTS FOR SOUTH WESTERN Engagement of Act Apprentice RAILWAY Railway Recruitment Cell Train Accidents Inquiry Reports Public Information Regarding Train Accident After tabling of Summary of Works and Grants in Parliament the details of budget allocation and work sanctioned was available to Railway. Today Shri A.K. GUPTA, General Manager, South Western Railway has conducted press Conference and shared the details of work sanctioned to SWR &allocation of funds to SWR. In the current year Rs. 3353 Crore is sanctioned as against Rs. 3174 Crore last year. He was sharing the Union budget announcements with the media at Rail Soudha, Hubballi. Shri B.B. Singh, Additional General Manager; Shri G.J. Prasad, Principal Chief Operations Manager; Shri K. Shiva Prasad, Chief Commercial Manager; Shri Rajiv Kumar, Principal Chief Electrical Engineer; Shri D.L. Chowdhry, Principal Chief Mechanical Engineer; and other senior officers were present in conference.