Chapter 4 Chemical Hazards
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Billing Code: 3510-Ds-P Department Of
This document is scheduled to be published in the Federal Register on 01/30/2015 and available online at http://federalregister.gov/a/2015-01795, and on FDsys.gov BILLING CODE: 3510-DS-P DEPARTMENT OF COMMERCE International Trade Administration C-570-009 Calcium Hypochlorite from the People’s Republic of China: Countervailing Duty Order AGENCY: Enforcement and Compliance, International Trade Administration, Department of Commerce SUMMARY: Based on affirmative final determinations by the Department of Commerce (“Department”) and the International Trade Commission (“ITC”), the Department is issuing a countervailing duty order on calcium hypochlorite from the People’s Republic of China (“PRC”). EFFECTIVE DATE: [(Insert date of publication in the Federal Register]. FOR FURTHER INFORMATION CONTACT: Katie Marksberry, AD/CVD Operations, Office V, Enforcement and Compliance, International Trade Administration, U.S. Department of Commerce, 14th Street and Constitution Avenue, NW, Washington, DC 20230; telephone: (202) 482-7906. SUPPLEMENTARY INFORMATION: Background In accordance with section 705(d) of the Tariff Act of 1930, as amended (“the Act”), on December 15, 2014, the Department published its final determination that countervailable subsidies are being provided to producers and exporters of calcium hypochlorite from the PRC.1 On January 21, 2015, the ITC notified the Department of its final determination pursuant to 1 See Calcium Hypochlorite from the People’s Republic of China: Final Affirmative Countervailing Duty Determination; 79 FR -

THE JOURNAL of INDUSTRIAL and ENGINEERING CHEMISTRY 953 with Stirring, and the Flask Allowed to Stand
OCt., 1917 THE JOURNAL OF INDUSTRIAL AND ENGINEERING CHEMISTRY 953 with stirring, and the flask allowed to stand. The ascertaining the presence of aniline, the calcium hypo- solution, when the precipitate has settled, is filtered chlorite test is employed. The quantitative deter- through a Gooch crucible, using a bell jar arrangement, mination is carried out by precipitating the aniline into a 250 to 300 cc. Erlenmeyer flask. The crucible as tribromoaniline with bromine water. The precipi- is fitted preferably with a small circular filter paper tate is caught on a tared filter paper, dried in vacuo, (cut to size) instead of asbestos. The flask should be and weighed. washed with wash-ether (100parts absolute ether and In this connection, it occurred to the writer that it 2 parts alcoholic HC1) while filtering so as not to allow might be possible to work out, for estimating the any ferric chloride to dry on the white precipitate or aniline, a colorimetric method based on the qualita- on the crucible. The usual precautions of washing the tive test with hypochlorite. If this were possible, flask, crucible and funnel are taken to insure complete it certainly would be desirable, for not only would transfer of iron. It is not necessary, however, to trans- considerable time and effort be saved but probably fer all of the aluminum chloride precipitate to the a considerably smaller sample than IO liters would be Gooch crucible. The aluminum precipitate is removed sufficient and quantitative measurements could also with the paper from the crucible by tapping it into a be applied in cases where the amount of aniline in 25 cc. -

Chloroform 18.08.2020.Pdf
Chloroform Chloroform, or trichloromethane, is an organic compound with formula CHCl3. It is a colorless, sweet-smelling, dense liquid that is produced on a large scale as a precursor to PTFE. It is also a precursor to various refrigerants. It is one of the four chloromethanes and a trihalomethane. It is a powerful anesthetic, euphoriant, anxiolytic and sedative when inhaled or ingested. Formula: CHCl₃ IUPAC ID: Trichloromethane Molar mass: 119.38 g/mol Boiling point: 61.2 °C Density: 1.49 g/cm³ Melting point: -63.5 °C The molecule adopts a tetrahedral molecular geometry with C3v symmetry. Chloroform volatilizes readily from soil and surface water and undergoes degradation in air to produce phosgene, dichloromethane, formyl chloride, carbon monoxide, carbon dioxide, and hydrogen chloride. Its half-life in air ranges from 55 to 620 days. Biodegradation in water and soil is slow. Chloroform does not significantly bioaccumulate in aquatic organisms. Production:- In industry production, chloroform is produced by heating a mixture of chlorine and either chloromethane (CH3Cl) or methane (CH4). At 400–500 °C, a free radical halogenation occurs, converting these precursors to progressively more chlorinated compounds: CH4 + Cl2 → CH3Cl + HCl CH3Cl + Cl2 → CH2Cl2 + HCl CH2Cl2 + Cl2 → CHCl3 + HCl Chloroform undergoes further chlorination to yield carbon tetrachloride (CCl4): CHCl3 + Cl2 → CCl4 + HCl The output of this process is a mixture of the four chloromethanes (chloromethane, dichloromethane, chloroform, and carbon tetrachloride), which can then be separated by distillation. Chloroform may also be produced on a small scale via the haloform reaction between acetone and sodium hypochlorite: 3 NaClO + (CH3)2CO → CHCl3 + 2 NaOH + CH3COONa Deuterochloroform[ Deuterated chloroform is an isotopologue of chloroform with a single deuterium atom. -
CHEMICAL STORAGE SEGREGATION GUIDELINES Incompatible Chemicals Should Always Be Handled and Stored So That They Do Not Accidentally Come in Contact with Each Other
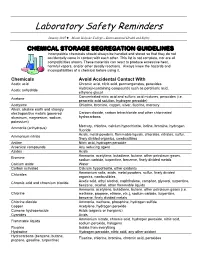
Laboratory Safety Reminders January 2007 ♦ Mount Holyoke College – Environmental Health and Safety CHEMICAL STORAGE SEGREGATION GUIDELINES Incompatible chemicals should always be handled and stored so that they do not accidentally come in contact with each other. This list is not complete, nor are all compatibilities shown. These materials can react to produce excessive heat, harmful vapors, and/or other deadly reactions. Always know the hazards and incompatibilities of a chemical before using it. Chemicals Avoid Accidental Contact With Acetic acid Chromic acid, nitric acid, permanganates, peroxides Hydroxyl-containing compounds such as perchloric acid, Acetic anhydride ethylene glycol Concentrated nitric acid and sulfuric acid mixtures, peroxides (i.e. Acetone peracetic acid solution, hydrogen peroxide) Acetylene Chlorine, bromine, copper, silver, fluorine, mercury Alkali, alkaline earth and strongly electropositive metals (powered Carbon dioxide, carbon tetrachloride and other chlorinated aluminum, magnesium, sodium, hydrocarbons potassium) Mercury, chlorine, calcium hypochlorite, iodine, bromine, hydrogen Ammonia (anhydrous) fluoride Acids, metal powders, flammable liquids, chlorates, nitrates, sulfur, Ammonium nitrate finely divided organics, combustibles Aniline Nitric acid, hydrogen peroxide Arsenical compounds Any reducing agent Azides Acids Ammonia, acetylene, butadiene, butane, other petroleum gases, Bromine sodium carbide, turpentine, benzene, finely divided metals Calcium oxide Water Carbon activated Calcium hypochlorite, other -

NACE Bromine Chemistry Review Paper
25 YEARS OF BROMINE CHEMISTRY IN INDUSTRIAL WATER SYSTEMS: A REVIEW Christopher J. Nalepa Albemarle Corporation P.O. Box 14799 Baton Rouge, LA 70898 ABSTRACT Bromine chemistry is used to great advantage in nature for fouling control by a number of sessile marine organisms such as sponges, seaweeds, and bryozoans. Such organisms produce small quantities of brominated organic compounds that effectively help keep their surfaces clean of problem bacteria, fungi, and algae. For over two decades, bromine chemistry has been used to similar advantage in the treatment of industrial water systems. The past several years in particular has seen the development of several diverse bromine product forms – one-drum stabilized bromine liquids, all-bromine hydantoin solids, and pumpable gels. The purpose of this paper is to review the development of bromine chemistry in industrial water treatment, discuss characteristics of the new product forms, and speculate on future developments. Keywords: Oxidizing biocide, bleach, bromine, bromine chemistry, sodium hypobromite, activated sodium bromide, Bromochlorodimethylhydantoin, Bromochloromethyethylhydantoin, Dibromodi- methylhydantoin,, BCDMH, BCMEH, DBDMH, stabilized bromine chloride, stabilized hypobromite INTRODUCTION Sessile marine organisms generate metabolites to ward off predators and deter attachment of potential micro- and macrofoulants. Sponges, algae, and bryozoans for example, produce a rich variety of bromine-containing compounds that exhibit antifoulant properties (Fig. 1).1,2,3 Scientists are actively studying these organisms to understand how they maintain surfaces that are relatively clean and slime- free.4 Brominated furanones isolated from the red algae Delisea pulchra, for example, have been found to interfere with the chemical signals (acylated homoserine lactones) that bacteria use to communicate with one another to produce biofilms.5,6 This work may eventually lead to more effective control of microorganisms in a number of industries such as industrial water treatment, oil and gas production, health care, etc. -

Calcium Hypochlorite
Common Name: CALCIUM HYPOCHLORITE CAS Number: 7778-54-3 DOT Number: UN 1748 (Dry or with more than 39% Chlorine) UN 2880 (Hydrated) UN 2208 (Dry with between 10% to 39% RTK Substance number: 0323 Chlorine) Date: December 1996 Revision: April 2003 ------------------------------------------------------------------------- ------------------------------------------------------------------------- HAZARD SUMMARY * Calcium Hypochlorite can affect you when breathed in. * If you think you are experiencing any work-related health * Contact can severely irritate and burn the eyes and skin. problems, see a doctor trained to recognize occupational * Breathing Calcium Hypochlorite can irritate the nose and diseases. Take this Fact Sheet with you. throat. * Breathing Calcium Hypochlorite can irritate the lungs WORKPLACE EXPOSURE LIMITS causing coughing and/or shortness of breath. Higher No occupational exposure limits have been established for exposures may cause a build-up of fluid in the lungs Calcium Hypochlorite. This does not mean that this (pulmonary edema), a medical emergency, with severe substance is not harmful. Safe work practices should always shortness of breath. be followed. IDENTIFICATION WAYS OF REDUCING EXPOSURE Calcium Hypochlorite is a white powder, granule, or pellet * Where possible, enclose operations and use local exhaust with a strong Chlorine-like odor. It is used to kill algae and ventilation at the site of chemical release. If local exhaust bacteria, in bleach and in pool chemical products. ventilation or enclosure is not used, respirators should be worn. REASON FOR CITATION * Wear protective work clothing. * Calcium Hypochlorite is on the Hazardous Substance * Wash thoroughly immediately after exposure to Calcium List because it is cited by DOT, NFPA and EPA. Hypochlorite. * Definitions are provided on page 5. -

Safe Handling and Disposal of Chemicals Used in the Illicit Manufacture of Drugs
Vienna International Centre, PO Box 500, 1400 Vienna, Austria Tel.: (+43-1) 26060-0, Fax: (+43-1) 26060-5866, www.unodc.org Guidelines for the Safe handling and disposal of chemicals used in the illicit manufacture of drugs United Nations publication USD 26 Printed in Austria ISBN 978-92-1-148266-9 Sales No. E.11.XI.14 ST/NAR/36/Rev.1 V.11-83777—September*1183777* 2011—300 Guidelines for the Safe handling and disposal of chemicals used in the illlicit manufacture of drugs UNITED NATIONS New York, 2011 Symbols of United Nations documents are composed of letters combined with figures. Mention of such symbols indicates a reference to a United Nations document. ST/NAR/36/Rev.1 UNITED NATIONS PUBLICATION Sales No. E.11.XI.14 ISBN 978-92-1-148266-9 eISBN 978-92-1-055160-1 © United Nations, September 2011. All rights reserved. The designations employed and the presentation of material in this publication do not imply the expression of any opinion whatsoever on the part of the Secretariat of the United Nations concerning the legal status of any country, territory, city or area, or of its authorities, or concerning the delimitation of its frontiers or boundaries. Requests for permission to reproduce this work are welcomed and should be sent to the Secretary of the Publications Board, United Nations Headquarters, New York, N.Y. 10017, U.S.A. or also see the website of the Board: https://unp.un.org/Rights.aspx. Governments and their institutions may reproduce this work without prior authoriza- tion but are requested to mention the source and inform the United Nations of such reproduction. -
Hypochlorite Salts, As Weil As Chlorine Itself, in Aqueous Solution Produce Equilbrium Mixures of Hypochlorous Acid, Hypochlorite Ion and Chlorine
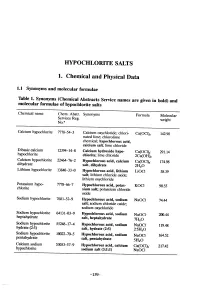
HYOCHLORITE SALTS 1. Chemical and Physical Data 1.1 Synonyms and molecular rormulae Table 1. Synonyms (Chemical Abstracts Service names are given in bold) and molecular rormulae or hyphlorite salts Chemical name Chem. Abstr. Synonyms Formula Molecular Servces Reg. weight No.u Calcium hyphlorite 7778-54-3 Calcium oxychloride; chlori- Ca(OCI)2 142.98 nated lime; chlorolime chemical; hypochlorous acid, calcium salt; lime chloride Dibasic calcium 12394-14-8 Calcium hydroxide hyp Ca(OCI)2" 291.14 hyphlorite chlonte; lime chloride 2Ca(OH)2 Calcium hyphlorite 22476-2 Hypochlorous acid, calcium Ca(OCI)2" 174.98 dihydrate salt, dihydrate 2H2O Lithium hyphlorite 1384-33-0 Hypchlorous acid, lithium LiOCI 58.39 salt; lithium chloride oxide; lithium oxychloride Potasium hyp 7778-6-7 Hypchlorous acid, potas- KOCI 90.55 chlorite sium salt; potasium chloride oxide Sodium hyphlorite 7681-52-9 Hyphlorous acid, sodium NaOCl 74.44 salt; soium chloride oxide; soium oxychloride Soium hyphlorite 64131-03-9 Hypchlorous acid, sodium heptahydrate NaOCl- 20.44 salt, heptahydrate 7H2O Sodium hyphlorite 5524-17-4 Hyphlorous acid, sodium NaOCI. 119.48 hydrate (2:5) salt, hydrate (2:5) 2-5H2O Sodium hyphlorite 10022-70-5 Hyphlorous acid, sodium NaOCI" 164.52 pentahydrate salt, pentahydrate 5H2O Calcium soium 53053-57-9 Hypchlorous acid, calcium Ca(OCI)2- 217.42 hyphlorite sodium salt (3:1:1) NaOCI -159- 160 lARe MONOGRAHS VOLUME 52 1.2 Chernical and physical properties or the pure substances From Weast (1989) unless otherwise specified Calciurn hyphlorite (a) Description: White powder or flat plates (b) Melting-point: Decomposes at 100°C (c) Density Specific gravity = 2.35 (d) Solubility: Soluble in cold water, 21.4% soluble at 25°C (Wojtowicz, 1979); insoluble in ethanol (e) Stability: Solid form decomposes exothermically when heated to 175°C, releasing oxygen (Mannsvile Chemical Products Corp., 1987). -

Chemicals Found in Pool Water Can Be Derived from a Number of Sources
CHAPTER 4 CChemicalhemical hhazardsazards hemicals found in pool water can be derived from a number of sources: the source Cwater, deliberate additions such as disinfectants and the pool users themselves (see Figure 4.1). This chapter describes the routes of exposure to swimming pool chemi- cals, the chemicals typically found in pool water and their possible health effects. While there is clearly a need to ensure proper consideration of health and safety issues for operators and pool users in relation to the use and storage of swimming pool chemicals, this aspect is not covered in this volume. Chemicals in pool, hot tub and spa water Source water-derived: Bather-derived: Management-derived: disinfection by-products; urine; disinfectants; precursors sweat; pH correction chemicals; dirt; coagulants lotions (sunscreen, cosmetics, soap residues, etc.) Disinfection by-products: e.g. trihalomethanes; haloacetic acids; chlorate; nitrogen trichloride Figure 4.1. Possible pool water contaminants in swimming pools and similar environments 4.1 Exposure There are three main routes of exposure to chemicals in swimming pools and similar environments: • direct ingestion of water; • inhalation of volatile or aerosolized solutes; and • dermal contact and absorption through the skin. 60 GUIDELINES FOR SAFE RECREATIONAL WATER ENVIRONMENTS llayoutayout SSafeafe WWater.inddater.indd 8822 224.2.20064.2.2006 99:57:05:57:05 4.1.1 Ingestion The amount of water ingested by swimmers and pool users will depend upon a range of factors, including experience, age, skill and type of activity. The duration of ex- posure will vary signifi cantly in different circumstances, but for adults, extended ex- posure would be expected to be associated with greater skill (e.g. -

ECR Calcium Hypochlorite Granules EPA Reg
STORAGE AND DISPOSAL ® Read before using ECR CALCIUM Do not contaminate food or feed by storage, disposal, or cleaning of equipment. Pesticide Storage- Keep this product dry in a tightly closed container when not in use. HYPOCHLORITE Store in a cool, dry, well ventilated area away from heat or open flame. In case of decom- position, isolate container (if possible) and flood area with large amounts of water to dis- solve all materials before discarding this container. PRECAUTIONARY STATEMENTS Pesticide Disposal - Pesticide wastes may be hazardous. Improper disposal of excess HAZARDS TO HUMAN AND DOMESTIC ANIMALS GRANULES pesticide, spray mixture or rinsate is a violation of Federal Law. If these wastes cannot be disposed of use according to label instructions, contact you State Pesticide or Environ- DANGER : Highly corrosive. Causes irreversible eye damage and skin burns. Do not get in Active Ingredient: mental Control Agency, or the Hazardous Waste Representative at the nearest EPA Re- eyes, on skin, or on clothing. Wear goggles or face shield and rubber gloves when handling gional Office for guidance. this product. Wash thoroughly with soap and water after handling and before eating, drink- Calcium Hypochlorite ………………………………… 68.0% Container Disposal - Non-Refillable container. Triple rinse as follows: Empty the remain- ing, chewing gum, using tobacco, or using the toilet. Remove and wash contaminated cloth- Inert Ingredients ……………………………………… 32.0% ing contents into application equipment or a mix tank. Fill the container 1/4 full with water. ing and shoes before reuse. May be Fatal if swallowed. Irritating to nose and throat. Avoid Replace and tighten closures. -

Conversion from Traditional Biocide to Miox On-Site Generation at Nrg Phoenix Chilled Water Plant
Fehr Solutions, LLC Water Treatment Services and Consulting CONVERSION FROM TRADITIONAL BIOCIDE TO MIOX ON-SITE GENERATION AT NRG PHOENIX CHILLED WATER PLANT MICHAEL FEHR, PH.D. FEHR SOLUTIONS, LLC Fehr Solutions, LLC Water Treatment Services and Consulting BACKGROUND ON BIOLOGICAL CONTROL • BIOLOGICAL CONTROL WITHIN COOLING TOWERS HAS ALWAYS BEEN IMPORTANT FROM A PERFORMANCE AND SAFETY STANDPOINT. • IT HAS BECOME EVEN MORE IMPORTANT WITH THE ASHRAE 188-2015 STANDARD BEING ISSUED • COOLING TOWERS FOR DISTRICT ENERGY SYSTEMS ARE ALMOST BY DEFINITION LOCATED IN HIGHLY POPULATED AREAS • INCREASES POTENTIAL EXPOSURE • THE TECHNOLOGY USED TO CONTROL BACTERIAL GROWTH HAS STAGNATED Fehr Solutions, LLC Water Treatment Services and Consulting THE “BIOLOGICAL CONTROL” PLAYERS Non-Oxidizers (slow acting) Oxidizers (fast acting) Activated Bromine (Sodium Bromide + Bleach (12.5%) Isothiazolin Glutaraldehyde HOCl) Stabilized Chlorine Bromine (12 Dioxide %) Quats DBNPA BCDMH (Solid) Fehr Solutions, LLC Water Treatment Services and Consulting THE FEED AND CONTROL STRATEGIES • CONTINUOUS • MAINTAIN CONTINUOUS RESIDUAL • SLUG FEED • SLUG FEED ON REGULAR BASIS ON A REPEATING CYCLE • OFTEN OVERLAID WITH REGULAR NON-OXIDIZER USAGE • CONTROL • ORP • FREE CHLORINE ANALYZERS • REAGENT TYPE • MEMBRANE TYPE Fehr Solutions, LLC Water Treatment Services and Consulting THE HANDLING PROBLEM • BIOCIDES ARE GENERALLY THE MOST • CHLORINE DIOXIDE HAZARDOUS MATERIALS IN A FACILITY • PRECURSORS CAN BE EXPLOSIVE (IF DRIED) • THEY ARE DESIGNED TO KILL BACTERIA AND • OSHA LIMIT -

Calcium Hypochlorite from China
UNITED STATES INTERNATIONAL TRADE COMMISSION Washington, DC Investigation Nos. 701-TA-510 and 731-TA-1245 (Final) CALCIUM HYPOCHLORITE FROM CHINA Scheduling of the final phase of countervailing duty and antidumping duty investigations. AGENCY: United States International Trade Commission. ACTION: Notice. SUMMARY: The Commission hereby gives notice of the scheduling of the final phase of antidumping and countervailing duty investigation Nos. 701-TA-510 and 731-TA-1245 (Final) under sections 705(b) and 731(b) of the Tariff Act of 1930 (19 U.S.C. '' 1671d(b) and 1673d(b)) (the Act) to determine whether an industry in the United States is materially injured or threatened with material injury, or the establishment of an industry in the United States is materially retarded, by reason of subsidized and less-than-fair-value imports from China of calcium hypochlorite, provided for in subheadings 2828.10.00, 3808.94.50, or 3808.99.95 of the Harmonized Tariff Schedule of the United States.1 For further information concerning the conduct of this phase of the investigations, hearing procedures, and rules of general application, consult the Commission=s Rules of Practice and Procedure, part 201, subparts A through E (19 CFR part 201), and part 207, subparts A and C (19 CFR part 207). EFFECTIVE DATE: Friday, July 25, 2014. FOR FURTHER INFORMATION CONTACT: Fred Ruggles (202-205-3187), Office of Investigations, U.S. International Trade Commission, 500 E Street SW, Washington, DC 20436. Hearing-impaired persons 1 For purposes of these investigations, the Department of Commerce has defined the subject merchandise as Acalcium hypochlorite, regardless of form (e.g., powder, tablet (compressed), crystalline (granular), or in liquid solution), whether or not blended with other materials, containing at least 10% available chlorine measured by actual weight.