Diazepam, Pentobarbital, and Methaqualone Effects on Several Behaviors in the Rat and Antagonism by Ro 15-1788 David J
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Diazepam - Alcohol Withdrawal
Diazepam - alcohol withdrawal Why have I been prescribed diazepam? If a person stops drinking alcohol after a time of drinking too much they can experience withdrawal effects. These include “the shakes”, sweating, having fits, seeing things which are not there (hallucinations) and feeling anxious and low in mood. They can feel wound up and find it difficult to sleep. These withdrawal effects can be very uncomfortable and in extreme cases can be dangerous if they persist into “DTs” (delirium tremens). Diazepam is used to help reduce these withdrawal symptoms. It relieves anxiety and tension and aids sleep. Diazepam can also prevent fits. It controls the withdrawal symptoms until the body is free of alcohol and has settled down. This usually takes three to seven days from the time you stop drinking. What exactly is diazepam? Diazepam is a benzodiazepine. This group of medicines is also called anxiolytics or minor tranquillisers. Diazepam has many uses. It can be used to reduce symptoms of anxiety and insomnia, as well as to help people come off alcohol. Diazepam should only be prescribed and taken as a short course. Is diazepam safe to take? Diazepam is safe to take for a short period of time, but it doesn’t suit everyone. Below are a few conditions where diazepam may be less suitable. If any of these apply to you please tell your doctor or key-worker. If you have depression or a mental illness If you have lung disease or breathing problems, or suffer from liver or kidney trouble If you take any other medicines or drugs, including those on prescription and bought from a chemist If you take illicit drugs bought “on the street” If you are pregnant or breast-feeding What is the usual dose of diazepam? The dose of diazepam will usually be started at 10-20mg four times a day. -
What Is Diazepam?
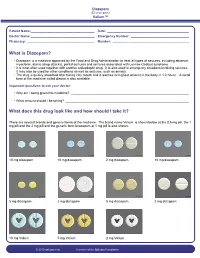
Diazepam (Di-a-ze-pam) Valium™ Patient Name: ___________________________________ Date: _____________________________________________ Doctor Name: ___________________________________ Emergency Number: ________________________________ Pharmacy: _____________________________________ Number: __________________________________________ What is Diazepam? • Diazepam is a medicine approved by the Food and Drug Administration to treat all types of seizures, including absence, myoclonic, atonic (drop attacks), partial seizures and seizures associated with Lennox-Gastaut syndrome. • It is most often used together with another antiepileptic drug. It is also used in emergency situations involving seizures. It may also be used for other conditions as well as seizures, such as anxiety. • The drug is quickly absorbed after taking it by mouth and it reaches its highest amount in the body in 1-2 hours. A rectal form of the medicine called diastat is also available. Important questions to ask your doctor: • Why am I being given this medicine? _________________________________________________________________ • What amount should I be taking? ____________________________________________________________________ What does this drug look like and how should I take it? There are several brands and generic forms of the medicine. The brand name Valium is shown below at the 0.5 mg pill, the 1 mg pill and the 2 mg pill and the generic form lorazepam at 1 mg pill is also shown. 10 mg diazepam 10 mg diazepam 2 mg diazepam 10 mg diazepam 5 mg diazepam 2 mg diazepam 5 mg diazepam 2 mg diazepam 10 mg Valium 5 mg Valium 2 mg Valium © 2010 epilepsy.com A service of the Epilepsy Foundation Diazepam (Di-a-ze-pam) Valium™ Frequently Asked Questions: How do I take Diazepam? To use the tablet form: chew tablets and swallow or swallow the tablet whole. -

Date Rape and Steroid Panels, Updated Feb 1 2010
DRUG-FACILITATED SEXUAL ASSAULT (aka “DATE RAPE”) AND STEROID PANELS (Effective January 26, 2010) Basic Date Rape Panel Comprehensive Date Rape Panel • GHB (Hair Only) • Ketamine • GHB • Benzodiazepines, including Rohypnol • Benzodiazepines Alprazolam Clonazepam Alprazolam Clonazepam Diazepam Flunitrazepam (Rohypnol) Diazepam Flunitrazepam Lorazepam Oxazepam Lorazepam Oxazepam Temazepam Nitrazepam Temazepam Nitrazepam • Opioids Codeine Hydrocodone Comprehensive Date Rape Panel Meperidine Tramadol (Urine Only) Methadone Fentanyl • GHB • Sedatives/Hypnotics Ketamine Methaqualone • Barbiturates Zolpidem Zopiclone Amobarbital Butalbital Pentobarbital Phenobarbital • Over-The-Counter Drugs Secobarbital Diphenhydramine Dextromethorphan Doxylamine Chlorpheniramine • Benzodiazepines Brompheniramine Promethazine Alprazolam Clonazepam Pheniramine Diazepam Flunitrazepam Lorazepam Oxazepam • Muscle Relaxants Temazepam Nitrazepam Carisoprodol Meprobamate • Opioids Cyclobenzaprine Methocarbamol Codeine Morphine • Hallucinogens (PCP) Hydrocodone Hydromorphone Oxycodone Oxymorphone Meperidine Tramadol ANABOLIC STEROID PANEL Methadone Fentanyl (Urine or Blood) Propoxyphene Buprenorphine Androstenedione Boldenone • Sedatives/Hypnotics Fluoxymesterolone Mesterolone Ketamine Methaqualone 17-a-Methyltestosterone Methenolone Zolpidem Zopiclone Methandrostenolone Nandrolone • Over-The-Counter Drugs Norethandrolone Oxandrolone Diphenhydramine Dextromethorphan Stanozolol Trenbolone Doxylamine Chlorpheniramine Brompheniramine Promethazine Pheniramine For additional steroids, • Muscle Relaxants call for details and pricing Carisoprodol Meprobamate EXPERTOX, INC. Cyclobenzaprine Methocarbamol Blood should only be 1803 CENTER STREET, SUITE A submitted for date rape • Hallucinogens DEER PARK, TX 77536 PCP MDMA panels if within five (5) hours of 281.476.4600 MDA MDEA ingestion. FAX 281.930.8856 Cannabinoids (Carboxy-THC) • WWW.EXPERTOX.COM Turaround Time: Ten (10) Urine must be collected within five (5) days business days from specimen of drug exposure receipt at the lab . -

Calculating Equivalent Doses of Oral Benzodiazepines
Calculating equivalent doses of oral benzodiazepines Background Benzodiazepines are the most commonly used anxiolytics and hypnotics (1). There are major differences in potency between different benzodiazepines and this difference in potency is important when switching from one benzodiazepine to another (2). Benzodiazepines also differ markedly in the speed in which they are metabolised and eliminated. With repeated daily dosing accumulation occurs and high concentrations can build up in the body (mainly in fatty tissues) (2). The degree of sedation that they induce also varies, making it difficult to determine exact equivalents (3). Answer Advice on benzodiazepine conversion NB: Before using Table 1, read the notes below and the Limitations statement at the end of this document. Switching benzodiazepines may be advantageous for a variety of reasons, e.g. to a drug with a different half-life pre-discontinuation (4) or in the event of non-availability of a specific benzodiazepine. With relatively short-acting benzodiazepines such as alprazolam and lorazepam, it is not possible to achieve a smooth decline in blood and tissue concentrations during benzodiazepine withdrawal. These drugs are eliminated fairly rapidly with the result that concentrations fluctuate with peaks and troughs between each dose. It is necessary to take the tablets several times a day and many people experience a "mini-withdrawal", sometimes a craving, between each dose. For people withdrawing from these potent, short-acting drugs it has been advised that they switch to an equivalent dose of a benzodiazepine with a long half life such as diazepam (5). Diazepam is available as 2mg tablets which can be halved to give 1mg doses. -

National Clearinghouse for Drug Abuse Information Selected Reference Series, Series 1, No
DOCUMENT RESOHE ED 090 455 CG 008 832 TITLE National Clearinghouse For Drug Abuse Information Selected Reference Series, Series 1, No. 1. INSTITUTION National Inst. of Mental Health (DHEW), Rockville, Hd. National Clearinghouse for Drug Abuse Information.; Student Association for the Study of Hallucinogens, Biloit, His. PDB DATE Nov 73 NOTE 13p. AVAILABLE FROM National Clearinghouse for Drug Abuse Information, p. 0. Box 1908, Rockville, Maryland 20850 EDRS PRICE MF-10.75 HC-S1.50 PLUS POSTAGE DESCRIPTORS ^Bibliographies; *Drug Abuse; *Drug Education; *Drug Therapy; Government Publications; ^Narcotics ABSTRACT One of a series of bibliographies published by the National Clearinghouse for Drug Abuse Information, this reference focuses on the drug, methagualone. Literature is selected for inclusion on the basis of its currency, significance in the field, and its availability to the public. Materials are directed toward researchers, educators, lawyers, physicians, and members of the public with more than a general need for information. Citations are not annotated. (Author/CJ) SERIES 7, No.l NOVEMBER 1973 Each bibliography of the National Clearinghouse for Drug Abuse 3- Information Selected Reference Series is a representative listing of citations on subjects of topical interest. The selection of o literature is based on its currency, its significance in the field, and its availability in local bookstores or research libraries. The scope of the material is directed toward students writing research papers, special interest groups, such as educators, lawyers and phy sicians, and the general public requiring more resources than public information materials can provide. Each reference series is meant to present an overview of the existing literature, but is not meant to be comprehensive or definitive in scope. -

Chemistry Information Sheet Methaqualone © 2014 Beckman Coulter, Inc
SYNCHRON System(s) METQ Chemistry Information Sheet Methaqualone © 2014 Beckman Coulter, Inc. All rights reserved. 475021 For In Vitro Diagnostic Use Rx Only ANNUAL REVIEW Reviewed by Date Reviewed by Date PRINCIPLE INTENDED USE METQ reagent, in conjunction with UniCel® DxC 600/800 System(s) and SYNCHRON® Systems Drugs of Abuse Testing (DAT) Urine Calibrators, is intended for the qualitative determination of methaqualone in human urine at a cutoff value of 300 ng/mL. The METQ assay provides a rapid screening procedure for determining the presence of methaqualone (METQ) and its metabolites in urine. This test provides only a preliminary analytical result; a positive result by this assay should be conrmed by another generally accepted non-immunological method such as thin layer chromatography (TLC), gas chromatography (GC), or gas chromatography/mass spectrometry (GC/MS). GC/MS is the preferred conrmatory method.1,2 Clinical consideration and professional judgement should be applied to any drug of abuse test result, particularly when preliminary positive results are used. CLINICAL SIGNIFICANCE Measurements of methaqualone are used as an aid in the diagnosis and treatment of methaqualone use or overdose. METHODOLOGY The Methaqualone assay utilizes a homogenous enzyme immunoassay method.3 The METQ reagent is comprised of specic antibodies which can detect methaqualone and its metabolites in urine. A drug-labeled glucose-6-phosphate dehydrogenase (G6PDH) conjugate competes with any free drug from the urine sample for a xed amount of antibody binding sites. In the absence of free drug from the sample, the drug-labeled G6PDH conjugate is bound by the specic antibody and the enzyme activity is inhibited. -

Drugs of Abuse: Benzodiazepines
Drugs of Abuse: Benzodiazepines What are Benzodiazepines? Benzodiazepines are central nervous system depressants that produce sedation, induce sleep, relieve anxiety and muscle spasms, and prevent seizures. What is their origin? Benzodiazepines are only legally available through prescription. Many abusers maintain their drug supply by getting prescriptions from several doctors, forging prescriptions, or buying them illicitly. Alprazolam and diazepam are the two most frequently encountered benzodiazepines on the illicit market. Benzodiazepines are What are common street names? depressants legally available Common street names include Benzos and Downers. through prescription. Abuse is associated with What do they look like? adolescents and young The most common benzodiazepines are the prescription drugs ® ® ® ® ® adults who take the drug Valium , Xanax , Halcion , Ativan , and Klonopin . Tolerance can orally or crush it up and develop, although at variable rates and to different degrees. short it to get high. Shorter-acting benzodiazepines used to manage insomnia include estazolam (ProSom®), flurazepam (Dalmane®), temazepam (Restoril®), Benzodiazepines slow down and triazolam (Halcion®). Midazolam (Versed®), a short-acting the central nervous system. benzodiazepine, is utilized for sedation, anxiety, and amnesia in critical Overdose effects include care settings and prior to anesthesia. It is available in the United States shallow respiration, clammy as an injectable preparation and as a syrup (primarily for pediatric skin, dilated pupils, weak patients). and rapid pulse, coma, and possible death. Benzodiazepines with a longer duration of action are utilized to treat insomnia in patients with daytime anxiety. These benzodiazepines include alprazolam (Xanax®), chlordiazepoxide (Librium®), clorazepate (Tranxene®), diazepam (Valium®), halazepam (Paxipam®), lorzepam (Ativan®), oxazepam (Serax®), prazepam (Centrax®), and quazepam (Doral®). -
Injecting Drug Users Etc.)
Economic and Social Council E/NR/2015/3 Annual Reports Questionnaire Part Three. Extent and patterns of and trends in drug use Report of the Government of: Reporting Year: reporting. Completed on (date): (dd/mm/yyyy) Please upload completed questionnaire to: https://arq.unodc.org/ The completed annual report questionnaire is due on: official March 31, 2016 For technical support, contact: for Phone Fax Email UNODC Vienna (+43-1) 26060-3914 (+43-1) 26060-5866 [email protected] Not Note: This is a printable version of the annual report questionnaire, which is in the form of an Excel spreadsheet and is designed to be completed electronically. In this printable version, definitions of key terms used in the questionnairecopy. are provided in the footnotes, whenever relevant; in the electronic version, these definitions (and additional instructions) are repeated throughout the questionnaire through the “Comments” function in Excel. The Excel spreadsheet also uses drop-down lists for some questions, allowing respondents to simply select from a list the answer that is most appropriate for their country. Sample INSTRUCTIONS The annual report questionnaire consists of the following four parts: Part One. Legislative and institutional framework; Part Two. Comprehensive approach to drug demand reduction; Part Three. Extent, patterns and trends in drug use; Part Four. Extent and patterns of and trends in drug crop cultivation and drug manufacture and trafficking This is part three of the annual report questionnaire. Respondents are asked to complete all questions. Where no data are available, this should be indicated by inserting two dashes (--) or writing "not known" in the appropriate cell. -

Antioxidative and Neuroprotective Effects of Leea Macrophylla
Ferdousy et al. Clinical Phytoscience (2016) 2:17 DOI 10.1186/s40816-016-0031-6 ORIGINAL CONTRIBUTION Open Access Antioxidative and neuroprotective effects of Leea macrophylla methanol root extracts on diazepam-induced memory impairment in amnesic Wistar albino rat Sakia Ferdousy1, Md Atiar Rahman1*, Md Mamun Al-Amin2, Jannatul Aklima1 and J. M. Kamirul Hasan Chowdhury1 Abstract Background: A neurological disorder is becoming one of the major health problems worldwide. Synthetic drugs for neurological disorders often produce unwanted effects while traditional plant- derived drugs offer a unique strategy in combating the neurological diseases. This study investigated how the antioxidative properties of Leea macrophylla root extracts integratively help as neuroprotective and antiamnesic in animal model. Methods: Leea macrophylla root methanol extract (LM) was assessed by open field test, hole cross test, elevated plus maze test and thiopental sodium induced sleeping time test for screening neuropharmacological effect on Wistar albino rats using the LM at 100 & 200 mg/kg body weight. Antiamnesic effect of LM was studied on diazepam induced anterograde amnesia in Wistar albino rats. Morris water maze test was performed to evaluate whether the learning and memory of rats are impaired by amnesia produced by diazepam. The antioxidative enzymes superoxide dismutase, catalase, glutathione peroxidase and oxidative biomarkers malondialdehyde, nitric oxide, advanced oxidation protein product from the hippocampus of decapitated animals were measured to assess the antioxidative potential of the extract. Results: LM was found to show significant (p <0.05) reduction in locomotor activity and increase in the duration of sleeping of animals. Morris water maze test showed that animals treated with LM significantly (p <0.05) decreased the mean escape latency compared to animals in diazepam group. -
Alcohol Withdrawal Management Guide
Alcohol Withdrawal Management Guide Withdrawal symptoms may begin within 6 to 12 hours after the last drink Symptoms can occur in heavy drinkers who still have detectable alcohol levels in their blood. Benzodiazepine and GHB (date rape) withdrawal are similarly treated with IV diazepam. A- Management of stable, uncomplicated, mild withdrawal (CIWA-Ar 8-15, see annex) For the prevention of Delirium Tremens (DT) and Wernicke’s Encephalopathy (WE)** 1- Diazepam (Valium) 10-20mg PO q1-2h prn until symptoms abate or CIWA-Ar score <8. Tapering doses are not required after this loading dose. Observe for 1-2 hours after last dose. Take-home medication for outpatients generally not required but if necessary (Diazepam 10mg 2 co prn). Consider reassessing patient daily to readjust dosing prn. If patient has : Medication of choice History of withdrawal seizures Diazepam 20mg PO q1h x minimum 3 doses Renal or liver dysfunction Lorazepam Elderly (>60 yr old) Lorazepam Hallucinosis (12-48hr after last drink) Consider adding antipsychotics (Olanzapine, Haloperidol) must consider Delirium Tremens NB antipsychotics can lowers seizure threshold **This loading guide will NOT prevent seizures in patients already taking regular large doses of benzodiazepines or barbiturates in addition to alcohol. Consider admission to ward. Accepted alternatives: - Lorazepam (Ativan) 1-2mg PO q2hr prn (Take-home medication: 1-2mg QID prn x 3-4 days #10 tabs). - Carbamazepine (Tegretol) 200mg PO q6hr day 1, q8hr day 2, q12h day 3, once daily day 4. NB do not use carbamazepine in moderate/severe alcohol withdrawal: does not prevent seizures. 2-Thiamine 100mg IM x 1, then 100mg PO for 3 days Decreases risk of Wernicke's encephalopathy: clinical triad of encephalopathy, oculomotor dysfunction, and gait ataxia. -

Chloral Hydrate: Summary Report
Chloral Hydrate: Summary Report Item Type Report Authors Yuen, Melissa V.; Gianturco, Stephanie L.; Pavlech, Laura L.; Storm, Kathena D.; Yoon, SeJeong; Mattingly, Ashlee N. Publication Date 2020-02 Keywords Compounding; Food, Drug, and Cosmetic Act, Section 503B; Food and Drug Administration; Outsourcing facility; Drug compounding; Legislation, Drug; United States Food and Drug Administration; Chloral Hydrate Rights Attribution-NoDerivatives 4.0 International Download date 26/09/2021 09:06:16 Item License http://creativecommons.org/licenses/by-nd/4.0/ Link to Item http://hdl.handle.net/10713/12087 Summary Report Chloral Hydrate Prepared for: Food and Drug Administration Clinical use of bulk drug substances nominated for inclusion on the 503B Bulks List Grant number: 2U01FD005946 Prepared by: University of Maryland Center of Excellence in Regulatory Science and Innovation (M-CERSI) University of Maryland School of Pharmacy February 2020 This report was supported by the Food and Drug Administration (FDA) of the U.S. Department of Health and Human Services (HHS) as part of a financial assistance award (U01FD005946) totaling $2,342,364, with 100 percent funded by the FDA/HHS. The contents are those of the authors and do not necessarily represent the official views of, nor an endorsement by, the FDA/HHS or the U.S. Government. 1 Table of Contents REVIEW OF NOMINATION ..................................................................................................... 4 METHODOLOGY ................................................................................................................... -

Tranxene (Clorazepate Dipotassium)
Tranxene* T-TAB® Tablets (clorazepate dipotassium tablets, USP) Rx only DESCRIPTION Chemically, TRANXENE is a benzodiazepine. The empirical formula is C16H11ClK2N2O4; the molecular weight is 408.92; 1H-1, 4-Benzodiazepine-3-carboxylic acid, 7-chloro-2,3 dihydro-2-oxo-5-phenyl-, potassium salt compound with potassium hydroxide (1:1) and the structural formula may be represented as follows: The compound occurs as a fine, light yellow, practically odorless powder. It is insoluble in the common organic solvents, but very soluble in water. Aqueous solutions are unstable, clear, light yellow, and alkaline. TRANXENE T-TAB tablets contain either 3.75 mg, 7.5 mg or 15 mg of clorazepate dipotassium for oral administration. Inactive ingredients for TRANXENE T-TAB Tablets: Colloidal silicon dioxide, FD&C Blue No. 2 (3.75 mg only), FD&C Yellow No. 6 (7.5 mg only), FD&C Red No. 3 (15 mg only), magnesium oxide, magnesium stearate, microcrystalline cellulose, potassium carbonate, potassium chloride, and talc. CLINICAL PHARMACOLOGY Pharmacologically, clorazepate dipotassium has the characteristics of the benzodiazepines. It has depressant effects on the central nervous system. The primary metabolite, nordiazepam, quickly appears in the blood stream. The serum half-life is about 2 days. The drug is metabolized in the liver and excreted primarily in the urine. Studies in healthy men have shown that clorazepate dipotassium has depressant effects on the central nervous system. Prolonged administration of single daily doses as high as 120 mg was without toxic effects. Abrupt cessation of high doses was followed in some patients by nervousness, insomnia, irritability, diarrhea, muscle aches, or memory impairment.