Collagenous Gastritis and Collagenous Colitis: a Report with Sequential Histological and Ultrastructural findings
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Inflammatory Bowel Disease Irritable Bowel Syndrome
Inflammatory Bowel Disease and Irritable Bowel Syndrome Similarities and Differences 2 www.ccfa.org IBD Help Center: 888.MY.GUT.PAIN 888.694.8872 Important Differences Between IBD and IBS Many diseases and conditions can affect the gastrointestinal (GI) tract, which is part of the digestive system and includes the esophagus, stomach, small intestine and large intestine. These diseases and conditions include inflammatory bowel disease (IBD) and irritable bowel syndrome (IBS). IBD Help Center: 888.MY.GUT.PAIN 888.694.8872 www.ccfa.org 3 Inflammatory bowel diseases are a group of inflammatory conditions in which the body’s own immune system attacks parts of the digestive system. Inflammatory Bowel Disease Inflammatory bowel diseases are a group of inflamma- Causes tory conditions in which the body’s own immune system attacks parts of the digestive system. The two most com- The exact cause of IBD remains unknown. Researchers mon inflammatory bowel diseases are Crohn’s disease believe that a combination of four factors lead to IBD: a (CD) and ulcerative colitis (UC). IBD affects as many as 1.4 genetic component, an environmental trigger, an imbal- million Americans, most of whom are diagnosed before ance of intestinal bacteria and an inappropriate reaction age 35. There is no cure for IBD but there are treatments to from the immune system. Immune cells normally protect reduce and control the symptoms of the disease. the body from infection, but in people with IBD, the immune system mistakes harmless substances in the CD and UC cause chronic inflammation of the GI tract. CD intestine for foreign substances and launches an attack, can affect any part of the GI tract, but frequently affects the resulting in inflammation. -
Microscopic Colitis: Collagenous Colitis and Lymphocytic Colitis
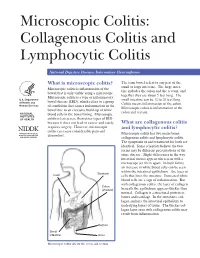
Microscopic Colitis: Collagenous Colitis and Lymphocytic Colitis National Digestive Diseases Information Clearinghouse What is microscopic colitis? The term bowel refers to any part of the small or large intestine. The large intes- Microscopic colitis is inflammation of the tine includes the colon and the rectum, and bowel that is only visible using a microscope. together they are about 5 feet long. The Microscopic colitis is a type of inflammatory U.S. Department small intestine can be 12 to 20 feet long. bowel disease (IBD), which refers to a group of Health and Colitis means inflammation of the colon. Human Services of conditions that causes inflammation in the Microscopic colitis is inflammation of the bowel due to an excessive build-up of white colon and rectum. NATIONAL blood cells in the bowel lining. Microscopic INSTITUTES OF HEALTH colitis is less severe than other types of IBD because it does not lead to cancer and rarely What are collagenous colitis requires surgery. However, microscopic and lymphocytic colitis? colitis can cause considerable pain and Microscopic colitis has two main forms: discomfort. collagenous colitis and lymphocytic colitis. The symptoms of and treatment for both are identical. Some scientists believe the two forms may be different presentations of the same disease. Slight differences in the way intestinal tissues appear when seen with a microscope set them apart. In both forms, an increase in white blood cells can be seen within the intestinal epithelium—the layer of Stomach Liver cells that lines the intestine. Increased white blood cells are a sign of inflammation. But with collagenous colitis, the layer of collagen Colon (shaded) beneath the epithelium appears thicker than normal. -
Practical Approach to Microscopic Colitis and Inflammatory Bowel Disease
INFLAMMATORY BOWEL DISEASE: A PRACTICAL APPROACH, SERIES #15 Seymour Katz, M.D., Series Editor Practical Approach to Microscopic Colitis and Inflammatory Bowel Disease by Noel R. Fajardo and Darrell S. Pardi INTRODUCTION The prevalence of IBD, on the other hand, is higher nflammatory disorders of the intestines can be than microscopic colitis, reflecting the younger age of divided into those with macroscopic mucosal onset in patients with IBD. Ichanges (the traditional inflammatory bowel dis- In North America, the incidence of microscopic eases: ulcerative colitis and Crohn’s disease) and those colitis was 0.8/100,000 person-years from 1985 to with primarily microscopic changes. 1989, and this increased significantly to19.1/100,000 Microscopic colitis is a chronic diarrheal condi- from 1998 to 2001 (1). The incidence of collagenous tion that is separated into two main subtypes: collage- colitis and lymphocytic colitis was 5.1 and 9.8/100,000 nous colitis and lymphocytic colitis. These two condi- person-years, and the prevalence was 36 and tions have similar clinical and histologic features, but 64/100,000 persons, respectively (1). In Europe, the are distinguished by the presence or absence of a incidence of collagenous and lymphocytic colitis ranges thickened subepithelial collagen band. Inflammatory from 0.6 to 5.2/100,000 person-years with a prevalence bowel disease (IBD) is traditionally separated into two between 10 to 16/100,000 persons (2). The reason for distinct clinical entities: Crohn’s disease and ulcera- the significantly higher incidence and prevalence of MC tive colitis. Although there is considerable symptom in North America compared with Europe is not known, overlap between these diseases, there are several fea- though increasing recognition may play a role. -

Chronic Viral Hepatitis in a Cohort of Inflammatory Bowel Disease
pathogens Article Chronic Viral Hepatitis in a Cohort of Inflammatory Bowel Disease Patients from Southern Italy: A Case-Control Study Giuseppe Losurdo 1,2 , Andrea Iannone 1, Antonella Contaldo 1, Michele Barone 1 , Enzo Ierardi 1 , Alfredo Di Leo 1,* and Mariabeatrice Principi 1 1 Section of Gastroenterology, Department of Emergency and Organ Transplantation, University “Aldo Moro” of Bari, 70124 Bari, Italy; [email protected] (G.L.); [email protected] (A.I.); [email protected] (A.C.); [email protected] (M.B.); [email protected] (E.I.); [email protected] (M.P.) 2 Ph.D. Course in Organs and Tissues Transplantation and Cellular Therapies, Department of Emergency and Organ Transplantation, University “Aldo Moro” of Bari, 70124 Bari, Italy * Correspondence: [email protected]; Tel.: +39-080-559-2925 Received: 14 September 2020; Accepted: 21 October 2020; Published: 23 October 2020 Abstract: We performed an epidemiologic study to assess the prevalence of chronic viral hepatitis in inflammatory bowel disease (IBD) and to detect their possible relationships. Methods: It was a single centre cohort cross-sectional study, during October 2016 and October 2017. Consecutive IBD adult patients and a control group of non-IBD subjects were recruited. All patients underwent laboratory investigations to detect chronic hepatitis B (HBV) and C (HCV) infection. Parameters of liver function, elastography and IBD features were collected. Univariate analysis was performed by Student’s t or chi-square test. Multivariate analysis was performed by binomial logistic regression and odds ratios (ORs) were calculated. We enrolled 807 IBD patients and 189 controls. Thirty-five (4.3%) had chronic viral hepatitis: 28 HCV (3.4%, versus 5.3% in controls, p = 0.24) and 7 HBV (0.9% versus 0.5% in controls, p = 0.64). -

Ulcerative Colitis: Diagnosis and Treatment ROBERT C
Ulcerative Colitis: Diagnosis and Treatment ROBERT C. LANGAN, MD; PATRICIA B. GOTSCH, MD; MICHAEL A. KRAFCZYK, MD; and DAVID D. SKILLINGE, DO, St. Luke’s Family Medicine Residency, Bethlehem, Pennsylvania Ulcerative colitis is a chronic disease with recurrent symptoms and significant morbidity. The precise etiology is still unknown. As many as 25 percent of patients with ulcerative colitis have extraintestinal manifestations. The diagnosis is made endoscopically. Tests such as perinuclear antineutrophilic cytoplasmic antibodies and anti-Saccharomyces cerevisiae antibodies are promising, but not yet recommended for routine use. Treatment is based on the extent and severity of the disease. Rectal therapy with 5-aminosalicylic acid compounds is used for proc- titis. More extensive disease requires treatment with oral 5-aminosalicylic acid compounds and oral corticosteroids. The side effects of steroids limit their usefulness for chronic therapy. Patients who do not respond to treatment with oral corticosteroids require hospitalization and intravenous steroids. Refractory symptoms may be treated with azathioprine or infliximab. Surgical treatment of ulcerative colitis is reserved for patients who fail medical therapy or who develop severe hemorrhage, perforation, or cancer. Longstanding ulcerative colitis is associated with an increased risk of colon cancer. Patients should receive an initial screening colonos- copy eight years after the onset of pancolitis and 12 to 15 years after the onset of left-sided dis- ease; follow-up colonoscopy should be repeated every two to three years. (Am Fam Physician 2007;76:1323-30, 1331. Copyright © 2007 American Academy of Family Physicians.) This article exempli- lcerative colitis is a chronic dis- of ulcerative colitis is not well understood. -

Liver Disease in Ulcerative Colitis: an Epidemiological and Follow up Study
84 Gut 1994; 35:84-89 Liver disease in ulcerative colitis: an epidemiological and follow up study in the county of Stockholm Gut: first published as 10.1136/gut.35.1.84 on 1 January 1994. Downloaded from U Broome, H Glaumann, G Hellers, B Nilsson, J Sorstad, R Hultcrantz Abstract sclerosing cholangitis (PSC) are said to be more In an epidemiological study ofthe incidence of common in patients with UC.47 The incidence of ulcerative colitis (UC) in the county of Stock- these complications varies in different studies holm between 1955 and 1979, 1274 patients depending on selection criteria and on the with UC were discovered. Almost all these definition of hepatobiliary disease.89 The true patients had regularly been investigated with incidence of hepatobiliary dysfunction in UC, liver function tests; 142 (11%) of them showed however, can only be obtained by tests of liver signs of hepatobiliary disease. A follow up function tests such as transaminases, alkaline study on all 142 patients with abnormal liver phosphatases, and bilirubin made routinely in function and UC was made between 1989 and unselected groups of patients with UC. Because 1991 to evaluate the cause of the liver abnor- the cause of hepatic involvement in UC is mality and to find out if the liver disease had enigmatic it is important to find out if the rate affected the survival rates. At follow up, eight of this complication is increasing, because of patients were reclassified as having Crohn's factors unrelated to UC, or if it mirrors the disease, 60 had developed normal liver func- incidence ofUC in itself. -
Familial Occurrence of Lymphocytic Colitis
BRIEF COMMUNICATION Familial occurrence of lymphocytic colitis Hugh J Freeman MD HJ Freeman. Familial occurrence of lymphocytic colitis. Can J Occurrence familiale de la colite Gastroenterol 2001;15(11):757-760. The familial occurrence lymphocytaire of lymphocytic colitis in a female parent and her two female children is reported. No other genetically based disorder, includ- RÉSUMÉ : On fait ici état de l’occurrence familiale de la colite lym- ing celiac disease, was evident. For both children, the age of phocytaire chez une patiente et ses deux filles. Aucune autre maladie diagnosis was more than two decades younger than the age of d’origine génétique, comme la maladie cæliaque, ne s’est manifestée. recognition of disease in the parent, and some clinical features, Pour les deux enfants, le diagnostic a été posé plus d’une vingtaine d’an- including the requirement for pharmacological agents in both nées avant l’âge qu’avait la mère au moment de son diagnostic et cer- taines caractéristiques cliniques, dont le traitement pharmacologique children, suggested that their disease severity was more signifi- chez les deux enfants, donnent à penser que leur maladie est plus grave cant than that of the involved parent. These characteristics of a que chez le parent atteint. Ces caractéristiques de la maladie familiale familial disease have been previously reported and labelled ont déjà été mentionnées et ont été appelées "anticipation génétique" ‘genetic anticipation’ in some monogenetic forms of neurologi- dans le cas de certaines formes monogénétiques de maladies neu- cal disease, as well as in other types of inflammatory bowel dis- rologiques, de même que dans d’autres types de maladies inflammatoires eases, including Crohn’s disease. -

Peptic Ulceration in Crohn's Disease (Regional Gut: First Published As 10.1136/Gut.11.12.998 on 1 December 1970
Gut, 1970, 11, 998-1000 Peptic ulceration in Crohn's disease (regional Gut: first published as 10.1136/gut.11.12.998 on 1 December 1970. Downloaded from enteritis) J. F. FIELDING AND W. T. COOKE From the Nutritional and Intestinal Unit, The General Hospital, Birmingham 4 SUMMARY The incidence of peptic ulceration in a personal series of 300 patients with Crohn's disease was 8%. Resection of 60 or more centimetres of the small intestine was associated with significantly increased acid output, both basally and following pentagastrin stimulation. Only five (4 %) of the 124 patients who received steroid therapy developed peptic ulceration. It is suggested that resection of the distal small bowel may be a factor in the probable increase of peptic ulceration in Crohn's disease. Peptic ulceration was observed in 4% of 600 1944 and 1969 for a mean period of 11-7 years patients with Crohn's disease by van Patter, with a mean duration of the disorder of 13.7 Bargen, Dockerty, Feldman, Mayo, and Waugh years. Fifty-one of these patients had Crohn's http://gut.bmj.com/ in 1954. Cooke (1955) stated that 11 of 90 patients colitis. Diagnosis in this series was based on with Crohn's disease had radiological evidence of macroscopic or histological criteria in 273 peptic ulceration whilst Chapin, Scudamore, patients, on clinical and radiological data in 25 Bagenstoss, and Bargen (1956) noted duodenal patients, and on clinical data together with minor ulceration in five of 39 (12.8%) successive radiological features in two patients with colonic patients with the disease who came to necropsy. -

Crohn's Disease and Ulcerative Colitis in the Same Patient
Gut: first published as 10.1136/gut.24.9.857 on 1 September 1983. Downloaded from Gut, 1983, 24, 857-862 Case report Crohn's disease and ulcerative colitis in the same patient C L WHITE III, S R HAMILTON, M P DIAMOND, AND J L CAMERON From the Departments ofPathology, Medicine, and Surgery, The Johns Hopkins University School of Medicine and Hospital, Baltimore, Maryland, USA SUMMARY A well documented case of a patient with both Crohn's disease and ulcerative colitis is presented. A 29 year old woman underwent resection of her terminal ileum and ascending colon for typical Crohn's disease with ileocolitis. Eleven years later, an ileoproctocolectomy was performed for typical ulcerative colitis involving the left colon. The resection specimen also showed evidence of colonic Crohn's disease near the anastomotic site. This unusual case shows that Crohn's disease and ulcerative colitis can occur in the same patient. The rarity of such cases supports the concept that Crohn's disease and ulcerative colitis are separate entities, rather than different manifestations of the same disease process. Crohn's disease and ulcerative colitis are the two healed with conservative measures. Four months well recognised forms of idiopathic inflammatory later she developed rectal bleeding. Proctoscopy bowel disease. As the aetiologies (or aetiology) of showed slightly inflamed rectal mucosa, but no idiopathic inflammatory bowel disease are biopsy was performed. Barium enema showed a unknown, these entities are distinguished on the stricture in the ascending colon; the caecum and basis of their pathologic and resulting clinical, and colon distal to the hepatic flexure were normal. -

Colitis and Proctitis
Customer Name, Street Address, City, State, Zip code Phone number, Alt. phone number, Fax number, e-mail address, web site Colitis and Proctitis (Inflammation of the Colon and Rectum) Basics OVERVIEW • “Colitis” is inflammation of the colon • “Proctitis” is inflammation of the rectum GENETICS • Breed susceptibility to histiocytic ulcerative colitis in boxers; histiocytic ulcerative colitis is inflammation characterized by a thickened lining of the colon with varying degrees of loss of the superficial lining (known as “ulceration”); the thickening is due to infiltration of various cells (histiocytes, plasma cells, and lymphocytes) in the layers under the lining • Possible association between inflammation of the colon (colitis) and one or multiple draining tracts around the anus (known as “perianal fistulas”) in German shepherd dogs SIGNALMENT/DESCRIPTION OF PET Species • Dogs • Cats Breed Predilections • Boxers—histiocytic ulcerative colitis; histiocytic ulcerative colitis is inflammation characterized by a thickened lining of the colon with varying degrees of loss of the superficial lining (known as “ulceration”); the thickening is due to infiltration of various cells (histiocytes, plasma cells, and lymphocytes) in the layers under the lining • German shepherd dogs—possible association between inflammation of the colon (colitis) and one or multiple draining tracts around the anus (perianal fistulas) Mean Age and Range • Any age • Boxers usually have clinical signs by 2 years of age SIGNS/OBSERVED CHANGES IN THE PET • Feces vary from semiformed -
Microscopic Colitis: Collagenous Colitis and Lymphocytic Colitis
A SPECIAL ARTICLE Microscopic Colitis: Collagenous Colitis and Lymphocytic Colitis Brennan A. Scott Thomas P. Prindiville Collagenous colitis and lymphocytic colitis are chronic relapsing diarrheal illnesses, which are often referred to together as microscopic colitis. It most commonly occurs in women in their fifth to sixth decade. The symptoms usually include profuse watery diarrhea and crampy abdominal pain. Laboratory and endoscopic studies are gener- ally normal but microscopic inflammation is seen when colonic biopsies are performed. In collagenous colitis there is a subepithelial collagen band in addition to chronic inflammation in the lamina propria. The etiology is not known but multiple theories exist including autoimmune, infectious, and medication-induced. Although the course is generally benign, patients may have multiple relapses over many years. Treatment regimens vary and have included anti-diarrheals, antibiotics, 5-aminosalicylates, steroids, and immunosuppressive agents. INTRODUCTION abdominal pain. Both conditions have normal mucosa ollagenous colitis (CC) (Figure 1) and lympho- when viewed endoscopically, however biopsy speci- cytic colitis (LC) (Figure 2) are uncommon mens show chronic mucosal inflammation. In CC C chronic relapsing diarrheal illnesses. The major- there is a subepithelial collagen band of varying thick- ity of patients are women in their fifth to sixth decade ness in association with an inflammatory cell infiltrate who complain of profuse, watery diarrhea, and crampy in the lamina propria (1). The collagen band is absent in LC (2,3). The term microscopic colitis (MC) was Brennan A. Scott, MD, Clinical Fellow, Division of Gas- originally used to describe patients with chronic diar- troenterology, University of California, Davis Medical rhea and normal endoscopic and barium enema stud- Center. -

Digestive Involvement in Primary Sjögren's Syndrome: Analysis from the Sjögrenser Registry
Digestive involvement in primary Sjögren’s syndrome: analysis from the Sjögrenser registry S. Melchor1, C. Sánchez-Piedra2, M. Fernández Castro3, J.L. Andreu3, V. Martínez Taboada4, A. Olivé5, J. Rosas6, R. Menor7, Á. García-Aparicio8, F.J. López Longo9, S. Manrique-Arija10, J.A. García Vadillo11, R. López-González12, J. Narváez13, C. Galisteo14, J. González Martín15, A. Naranjo16, Ó. Illera17, B. Moreira18, E. Raya19, M. Rodríguez López20, E. Júdez21, C. Moriano22, V. Torrente-Segarra23, B. García Magallón24, C. Guillén Astete25, I. Castellvi26, C. Bohórquez27, J. Loricera4, J. Belzunegui28, P.E. Carreira1, on behalf of the Sjögrenser group, part of the Spanish Society of Rheumatology Systemic Autoimmune Diseases Study Group (EASSER) Affiliations: page S115. ABSTRACT pancreatic involvement presented more Sheila Melchor, Carlos Sánchez-Piedra, Objective. Digestive involvement (DI) central nervous system and renal in- Mónica Fernández Castro, Jose Luis has been reported in 10–30% of prima- volvement, Raynaud’s phenomenon, Andreu, Víctor Martínez Taboada, ry Sjögren’s syndrome (pSS) patients, lymphoma and C3/C4 hypocomplemen- Alejandro Olivé, José Rosas, Raúl Menor, Ángel García-Aparicio, Francisco Javier and few studies have systematically taemia. López Longo, Sara Manrique-Arija, Jesús analysed the prevalence of DI in pSS Conclusion. DI is frequent in Sjög- Alberto García Vadillo, Ruth López- patients. The aim of this study was to renser patients, mainly in the form of González, Javier Narváez, Carlos Galisteo, describe DI prevalence in pSS patients autoimmune disorders, and seem to be Jorge González Martín, Antonio Naranjo, from the Sjögrenser Study, and to ana- associated with a more severe pheno- Óscar Illera, Begoña Moreira, Enrique Raya, Marina Rodríguez López, Enrique lyse its clinical associations.