Eastern Cheshire April 2015
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Counciltaxbase201819appendix , Item 47
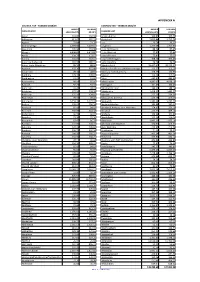
APPENDIX A COUNCIL TAX - TAXBASE 2018/19 COUNCIL TAX - TAXBASE 2018/19 BAND D TAX BASE BAND D TAX BASE CHESHIRE EAST EQUIVALENTS 99.00% CHESHIRE EAST EQUIVALENTS 99.00% Acton 163.82 162.18 Kettleshulme 166.87 165.20 Adlington 613.67 607.53 Knutsford 5,813.84 5,755.70 Agden 72.04 71.32 Lea 20.78 20.57 Alderley Edge 2,699.00 2,672.01 Leighton 1,770.68 1,752.97 Alpraham 195.94 193.98 Little Bollington 88.34 87.45 Alsager 4,498.81 4,453.82 Little Warford 37.82 37.44 Arclid 154.71 153.17 Lower Peover 75.81 75.05 Ashley 164.05 162.41 Lower Withington 308.54 305.45 Aston by Budworth 181.97 180.15 Lyme Handley 74.74 74.00 Aston-juxta-Mondrum 89.56 88.66 Macclesfield 18,407.42 18,223.35 Audlem 937.36 927.98 Macclesfield Forest/Wildboarclough 112.25 111.13 Austerson 49.34 48.85 Marbury-cum-Quoisley 128.25 126.97 Baddiley 129.37 128.07 Marton 113.19 112.06 Baddington 61.63 61.02 Mere 445.42 440.96 Barthomley 98.14 97.16 Middlewich 4,887.05 4,838.18 Basford 92.23 91.31 Millington 101.43 100.42 Batherton 24.47 24.23 Minshull Vernon 149.65 148.16 Betchton 277.16 274.39 Mobberley 1,458.35 1,443.77 Bickerton 125.31 124.05 Moston 277.53 274.76 Blakenhall 70.16 69.46 Mottram St Andrew 416.18 412.02 Bollington 3,159.33 3,127.74 Nantwich 5,345.68 5,292.23 Bosley 208.63 206.54 Nether Alderley 386.48 382.61 Bradwall 85.68 84.82 Newbold Astbury-cum-Moreton 374.85 371.10 Brereton 650.89 644.38 Newhall 413.32 409.18 Bridgemere 66.74 66.07 Norbury 104.94 103.89 Brindley 73.30 72.56 North Rode 125.29 124.04 Broomhall 87.47 86.59 Odd Rode 1,995.13 1,975.18 Buerton -

Index of Cheshire Place-Names
INDEX OF CHESHIRE PLACE-NAMES Acton, 12 Bowdon, 14 Adlington, 7 Bradford, 12 Alcumlow, 9 Bradley, 12 Alderley, 3, 9 Bradwall, 14 Aldersey, 10 Bramhall, 14 Aldford, 1,2, 12, 21 Bredbury, 12 Alpraham, 9 Brereton, 14 Alsager, 10 Bridgemere, 14 Altrincham, 7 Bridge Traffbrd, 16 n Alvanley, 10 Brindley, 14 Alvaston, 10 Brinnington, 7 Anderton, 9 Broadbottom, 14 Antrobus, 21 Bromborough, 14 Appleton, 12 Broomhall, 14 Arden, 12 Bruera, 21 Arley, 12 Bucklow, 12 Arrowe, 3 19 Budworth, 10 Ashton, 12 Buerton, 12 Astbury, 13 Buglawton, II n Astle, 13 Bulkeley, 14 Aston, 13 Bunbury, 10, 21 Audlem, 5 Burton, 12 Austerson, 10 Burwardsley, 10 Butley, 10 By ley, 10 Bache, 11 Backford, 13 Baddiley, 10 Caldecote, 14 Baddington, 7 Caldy, 17 Baguley, 10 Calveley, 14 Balderton, 9 Capenhurst, 14 Barnshaw, 10 Garden, 14 Barnston, 10 Carrington, 7 Barnton, 7 Cattenhall, 10 Barrow, 11 Caughall, 14 Barthomley, 9 Chadkirk, 21 Bartington, 7 Cheadle, 3, 21 Barton, 12 Checkley, 10 Batherton, 9 Chelford, 10 Bebington, 7 Chester, 1, 2, 3, 6, 7, 10, 12, 16, 17, Beeston, 13 19,21 Bexton, 10 Cheveley, 10 Bickerton, 14 Chidlow, 10 Bickley, 10 Childer Thornton, 13/; Bidston, 10 Cholmondeley, 9 Birkenhead, 14, 19 Cholmondeston, 10 Blackden, 14 Chorley, 12 Blacon, 14 Chorlton, 12 Blakenhall, 14 Chowley, 10 Bollington, 9 Christleton, 3, 6 Bosden, 10 Church Hulme, 21 Bosley, 10 Church Shocklach, 16 n Bostock, 10 Churton, 12 Bough ton, 12 Claughton, 19 171 172 INDEX OF CHESHIRE PLACE-NAMES Claverton, 14 Godley, 10 Clayhanger, 14 Golborne, 14 Clifton, 12 Gore, 11 Clive, 11 Grafton, -

NANTWICH HUNDRED. for the Confinement of Prisoners, Previous to Conviction
380 NANTWICH HUNDRED. for the confinement of prisoners, previous to conviction. There is also a room where the magisterial business is condueteda which is small and inconvenient, but is expected to be enlarged before the expiration of the year 1849. A residence adjoins, for the use of the Special High Constable, now Mr. Charles Laxton. THE THEATRE, a small structure, has been taken down about ten years. THE ExcisE OFFICE is at the Lamb Inn, Hospital street. This inn is much frequented by the farmers on the market-day. There is an excellent bowling-green connected with the Bowling-Green Tavern, situate in Monks lane. The Salt Water Baths are sitnate on Snow Hill; Mr. Thomas Townley, proprietor. THE UNION HousE, situated upon Beam Heath, is a. spacious brick building, erected for the accommodation of 350 inmates. The Union comprises uo less than eighty-six parishes and townships, for which ninety-three guardians are chosen, who meet at the Board-room for the transaction of business. Tbe several places comprised in the Union are-Acton, Alpraham, Alvaston, Aston-Juxta-Mondrum, Audlem, Austerson, Baddiley, Baddington, Bar· thomley, Basford, Batherton, Beeston, Bickerton, Bickley, Blakenball, Bridgemere, Brindley, Hroomhall, Buerton, Bulkeley, Bunbury, Burland, Burwardsley, Calveley, Checkley-cum WrinehiU, Cholmondeley, Cholmondestone, Chorley, Chorlton, Coole-Pilate, CoppenhaU Church, Coppenhall Monks, Crewe, Dodcot-cum-Wilkesley, Doddington, Eaton, Edlaston, Egerton, Faddiley, Hampton, Hankelow, Haslington, Hatherton, Haughton, Henhull, Hough, Hunsterson, Hurlston, La.rton, Lea, Leighton, Macefen, Marbury-cum-Quoisley, Minsbull Church, Minshull Vernon, Nantwich, Newhall, Norbury, Peckforton, Poole, Ridley, Rope, Rushton, Shavington-cum-Gresty, Sound, Spurstow, Stapeley, Stoke, Tarporley, Tilstone Fearnall, Tiverton, Tushingham-cum-Grindley, Utkinton. -

85 Bus Time Schedule & Line Route
85 bus time schedule & line map 85 Nantwich - Crewe - Keele - Newcastle View In Website Mode The 85 bus line (Nantwich - Crewe - Keele - Newcastle) has 4 routes. For regular weekdays, their operation hours are: (1) Crewe: 6:36 AM - 1:35 PM (2) Crewe: 6:00 PM - 7:40 PM (3) Nantwich: 6:48 AM - 5:15 PM (4) Newcastle Town Centre: 6:10 AM - 6:10 PM Use the Moovit App to ƒnd the closest 85 bus station near you and ƒnd out when is the next 85 bus arriving. Direction: Crewe 85 bus Time Schedule 39 stops Crewe Route Timetable: VIEW LINE SCHEDULE Sunday Not Operational Monday 6:36 AM - 1:35 PM Bus Station, Nantwich 51 Beam Street, Nantwich Tuesday 6:36 AM - 1:35 PM Wyche Primary School, Nantwich Wednesday 6:36 AM - 1:35 PM 9 Manor Gardens, Nantwich Thursday 6:36 AM - 1:35 PM Davenport Avenue, Nantwich Friday 6:36 AM - 1:35 PM 54 Manor Road, Nantwich Saturday 7:41 AM - 1:35 PM Cemetery Corner, Nantwich Sainsbury'S, Nantwich 34 Middlewich Road, Nantwich 85 bus Info Colleys Lane, Nantwich Direction: Crewe Stops: 39 Alvaston Hall Hotel, Wistaston Trip Duration: 33 min Line Summary: Bus Station, Nantwich, Wyche Houses, Wistaston Primary School, Nantwich, Davenport Avenue, Nantwich, Cemetery Corner, Nantwich, Sainsbury'S, The Rising Sun, Wistaston Nantwich, Colleys Lane, Nantwich, Alvaston Hall Hotel, Wistaston, Houses, Wistaston, The Rising Sun, The Beefeater, Woolstanwood Wistaston, The Beefeater, Woolstanwood, Marshƒeld Avenue, Marshƒeld, Tarvin Avenue, Marshƒeld, Acton Marshƒeld Avenue, Marshƒeld Road, Marshƒeld, Christleton Avenue, Marshƒeld, Co- -

Council Tax Charges 2020-2021
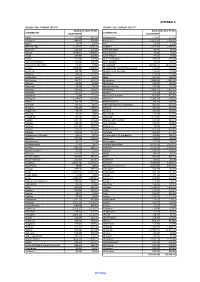
COUNCIL TAX CHARGES 2020-2021 Name A B C D E F G H Parish Total Parish Total Parish Total Parish Total Parish Total Parish Total Parish Total Parish Total Charge Charge Charge Charge Charge Charge Charge Charge Charge Charge Charge Charge Charge Charge Charge Charge Adult Social Care 87.25 101.79 116.33 130.87 159.95 189.03 218.12 261.74 CHESHIRE EAST BOROUGH COUNCIL 915.41 1,067.97 1,220.54 1,373.11 1,678.25 1,983.38 2,288.52 2,746.22 CHESHIRE FIRE AUTHORITY 52.86 61.67 70.48 79.29 96.91 114.53 132.15 158.58 POLICE & CRIME COMMISSIONER 140.29 163.68 187.06 210.44 257.20 303.97 350.73 420.88 1,195.81 1,395.11 1,594.41 1,793.71 2,192.31 2,590.91 2,989.52 3,587.42 ACTON PARISH COUNCIL 9.75 1,205.56 11.37 1,406.48 13.00 1,607.41 14.62 1,808.33 17.87 2,210.18 21.12 2,612.03 24.37 3,013.89 29.24 3,616.66 ADLINGTON PARISH COUNCIL 16.69 1,212.50 19.47 1,414.58 22.25 1,616.66 25.03 1,818.74 30.59 2,222.90 36.15 2,627.06 41.72 3,031.24 50.06 3,637.48 AGDEN PARISH MEETING 6.95 1,202.76 8.10 1,403.21 9.26 1,603.67 10.42 1,804.13 12.74 2,205.05 15.05 2,605.96 17.37 3,006.89 20.84 3,608.26 ALDERLEY EDGE PARISH COUNCIL 45.69 1,241.50 53.30 1,448.41 60.92 1,655.33 68.53 1,862.24 83.76 2,276.07 98.99 2,689.90 114.22 3,103.74 137.06 3,724.48 ALPRAHAM PARISH COUNCIL 18.20 1,214.01 21.23 1,416.34 24.27 1,618.68 27.30 1,821.01 33.37 2,225.68 39.43 2,630.34 45.50 3,035.02 54.60 3,642.02 ALSAGER TOWN COUNCIL 56.53 1,252.34 65.95 1,461.06 75.37 1,669.78 84.79 1,878.50 103.63 2,295.94 122.47 2,713.38 141.32 3,130.84 169.58 3,757.00 ARCLID PARISH COUNCIL 11.35 -

Cheshire. (Kelly's
270 CREWE. CHESHIRE. (KELLY'S Earl Douglias Henry, Deva villa, Wellington square County Court, Royal hotel, His Honor Beginald Brown Eardley Wilmot, Chester bridge, Crewe K.C., LL.B. judge; Charles Edward Speakman, regis Glover Thomas, Westview, West street trar & high bailiff ; office, CoppenhaH terrace ; Courts Hill ArtJmr Griffiths,Summerfield house,2o7 Nantwich rd are held alternately at Crewe & Nantwich, once a month Hodgson Willinm, Helmsville, Hightown at each place, usually on wednesdays at Crewe & satur Knott John, Ashton house, Victoria ~rtreet day-s at Nantwich. The places in the county court dis Lumb Wallace, Gatefield house, Crewe trict of Nantwich & Crewe are :-Acton, Alpraham, Mc:Neill William, Herdman street Alvaston, Amer Green, Aston-juxta-<.\fondrum, Aston Macrae Kenneth, 2 Wellington villas by-N ewall, Audlem, .Austerson, Baddiley, Baddington, Pedley Richard, Winterley, Crewe Balterley, Bathomley, Basford, Batherton, Barbridge. Robertson J ames, 2152 Hungerford road- Be-am Heath, BeN>ton, Betley, Bickerton, Blakenhall, Swinton Peter, 38 High street 'Blakelow, Bradfield Green, Bridgmere, Brindley, Broad Thomas John, Wedgwood villa, Nantwich road lane, Broomhall, Buerton, Bulkeley, Bunbury, Burland, Wallwork Henry, Chester bridge, Crewe Burwardsley, Oalveley, Checkley-cum-Wrinehill, Chol~ Whale George, We.stbank, Wellington square mondeley, Cholmonde-ston, Chorley, Chorlton, Coole Wilding John William, Linden grange, Hungerford avenue Pilate, C()tebrook, CoppenhaU Church, Crewe, Crewe Clerk, Charles Ed ward .Speakman, CoppenhaU terrace, Green, Doddington, Dodd's Green, Eaton, Edleston, :Market street Egerton, Faddiley, Gorsty hill, Hankelow, Hatherton, Borough Petty Sessions are held at the Court house every Haslington, Haughton, Henhull, 'Highwayside, Hough, alternate tues. at II a.m Hunsterson, Hurleston, lnglesea Brook, Larden Green, Larkton, Lea, Lee Green, Leighton, Minshull Church, CORPORATIO...~. -
Appendix Domestic Taxbase Report 2021-22.Pdf
APPENDIX A COUNCIL TAX - TAXBASE 2021/22 COUNCIL TAX - TAXBASE 2021/22 BAND D TAX BASE 99.00% BAND D TAX BASE 99.00% CHESHIRE EAST EQUIVALENTS CHESHIRE EAST EQUIVALENTS Acton 167.66 165.99 Kettleshulme 174.65 172.90 Adlington 646.45 639.99 Knutsford 5,852.03 5,793.51 Agden 70.04 69.34 Lea 22.23 22.01 Alderley Edge 2,733.87 2,706.53 Leighton 1,922.39 1,903.16 Alpraham 223.62 221.39 Little Bollington 86.34 85.48 Alsager 4,979.84 4,930.04 Little Warford 40.92 40.51 Arclid 207.90 205.82 Lower Peover 77.30 76.53 Ashley 162.00 160.38 Lower Withington 338.83 335.44 Aston by Budworth 190.90 188.99 Lyme Handley 70.02 69.32 Aston-juxta-Mondrum 95.64 94.68 Macclesfield 18,900.97 18,711.93 Audlem 1,058.40 1,047.81 Macclesfield Forest/Wildboarclough 119.36 118.17 Austerson 49.78 49.29 Marbury-cum-Quoisley 136.42 135.06 Baddiley 139.06 137.67 Marton 116.65 115.48 Baddington 65.17 64.51 Mere 491.21 486.30 Barthomley 102.74 101.71 Middlewich 4,981.03 4,931.22 Basford 93.92 92.98 Millington 102.85 101.82 Batherton 24.94 24.69 Minshull Vernon 148.48 146.99 Betchton 289.42 286.52 Mobberley 1,484.97 1,470.12 Bickerton 131.34 130.03 Moston 373.28 369.55 Blakenhall 71.88 71.16 Mottram St Andrew 417.00 412.83 Bollington 3,234.81 3,202.47 Nantwich 5,388.11 5,334.23 Bosley 219.79 217.60 Nether Alderley 594.59 588.64 Bradwall 89.41 88.51 Newbold Astbury-cum-Moreton 362.93 359.30 Brereton 743.27 735.84 Newhall 431.30 426.98 Bridgemere 69.55 68.86 Norbury 104.34 103.30 Brindley 70.55 69.85 North Rode 127.24 125.96 Broomhall 85.54 84.69 Odd Rode 2,010.80 1,990.69 -

Nantwich Accommodation Leaflet:Layout 1 14/04/2014 09:05 Page 1
Nantwich Accommodation Leaflet:Layout 1 14/04/2014 09:05 Page 1 Self Catering Accommodation Camping & Caravan Sites Reaseheath College The Old Dairy House Nantwich CW5 6DF Batherton lane, Batherton, Nantwich CW5 7QH 01270 613210 / 01270 625131 01270 625891 (Campus Accommodation for groups during July and August) Foxes Bank Farm Hunsterson, Nantwich, CW5 7PN Bank Farm Cottages 01270 520224 Newcastle Road, Hough, Crewe CW2 5JG The Cotton Arms www.bankfarmcottages.co.uk Cholmondeley Road, Wrenbury, 01270 841809 Nantwich CW5 8HG 01270 780377 The Rookery Haughton, Tarporley CW6 9RN New Farm www.therookerycheshire.com Long Lane, Wettenhall, Nr Winsford, CW7 4DW 01829 260069 www.newfarmcheshire.co.uk 01270 528213 Heald Country House Cholmondeley Road, Wrenbury, Manor Farm Nr Nantwich CW5 8HJ Egerton, Cholmondeley, Nr Malpas SY14 8AW 01270 781316 / 07922277292 01829 720261 Combermere Abbey Holiday Cottages Combermere Abbey, Whitchurch, Shropshire SY13 4AJ www.combermereabbey.co.uk 01948 660345 Manor Farm Holiday Cottages Manor Farm, Egerton, Malpas SY14 8AW www.egertonmanorfarm.co.uk For further information contact 01829 720261 Nantwich Information Centre: Civic Hall, Market Street, Nantwich, Cheshire CW5 5DG Millmoor Farm Tel: 01270 303150 / 01270 628633 Nomansheath, Malpas SY14 8ED Email: [email protected] 01948 820304 Website: www.nantwichtowncouncil.gov.uk List correct at time of printing Printed by Delmar Print • Tel: 01270 624122 Nantwich Accommodation Leaflet:Layout 1 14/04/2014 09:05 Page 2 Henhull Hall B&B -

Licencea Name Address1 Address2 Address3 Address4 Address5
licenceA name address1 address2 address3 address4 address5 PHO0036 Mrs Kathleen Birch 31 Biddulph Road Congleton CW12 3LQ PHO 0017 Mr Alan Buffey 25 Beech Avenue Rode Heath Cheshire East ST7 3SH PHO0051 Mr Paul James Ratcliffe 6 Mortimer Drive Sandbach Cheshire East CW11 4HS PHO0029 Mr Derek Anthony Goodale 10 New King Street Middlewich Cheshire East CW10 9EB PHOP 478 Mr Ian Stanley Ogdon 34 Fairfield Avenue Sandbach Cheshire East CW11 4BP PHO0154 Mr Nigel Thomas Davenport Swallow Eaves 214 Padgbury Lane Congleton Cheshire East CW12 4HU PHO 0255 Mr Philip Connor 32 Edwards Way Alsager Cheshire East ST7 2YB PHO0046 Mr John Anders Jennings 29 Rookery Close Sandbach Cheshire East CW11 3NJ PHO 0402 Mr Raymond Lees 38 St Annes Avenue Middlewich Cheshire East CW10 0AE 9 Mr Raymond Hinett 25 Randle Bennett Close Sandbach Cheshire East CW11 3GA PHO 0282/09 Mr Yani Dimov Yanev 65 Oldfield Road Sandbach Cheshire East CW11 3LX PHO 0010 Mr Peter Vincent Edwards 15 Stringer Avenue Sandbach Cheshire East CW11 4HH PHO003 Mr Andrew Lowe 82 Harpur Crescent Alsager Cheshire East ST7 2SY PHO0018 Mr William Anthony Radcliffe 11 Victoria Avenue Holmes Chapel Cheshire East CW4 7BE PHO0255 Mr Peter Robert Hickey 33 Kitfield Avenue Middlewich Cheshire East CW10 0AJ 27 Mr David John Tulloch 37 Whitemore Road Middlewich Cheshire East CW10 0DY Building 1 Room 10, Ashtenne Business PHO0008 Lifestyle Taxis Centre Radway Green Road Barthomley Crewe CW2 5PR TXOPE4-0209-11 Mr Ricki Bridle 29 Brooks Lane Middlewich Cheshire East CW10 0JG PHO0025 Mr David Goodwin 21 Swettenham -

Woolstanwood 01270 445678 Offers in Excess of £250,000
Offers in Excess of £250,000 3 1 3 5 REASONS WHY WE LOVE THIS HOUSE: THREE BED DETACHED FAMILY HOME SET ON SUNDALE DRIVE IN WOLSTANWOOD WITHIN 1 WALKING DISTANCE TO THE STUNNING QUEEN'S GARDENS OFFERING VERSATILE LIVING SPACE TO THE 2 GROUND FLOOR WITH AMPLE UPPER FLOOR ACCOMMODATION WITHIN A SHORT DRIVE TO BOTH NANTWICH 3 AND CREWE, BOTH OF WHICH OFFER A PLETHORA OF SHOPS, SCHOOLS AND AMENITIES INTERNALLY COMPRISING; ENTRANCE 4 HALLWAY, DINING ROOM, LIVING ROOM, SNUG/PLAYOM, W/C, KITCHEN/BREAKFAST ROOM, THREE DOUBLE BEDROOMS AND A FAMILY BATHROOM EXTERNALLY THERE IS OFF-ROAD PARKING 5 AND A DETACHED GARAGE ALONG WITH SWEEPING GARDENS TO THE FRONT, SIDE AND REAR OFFERING A MIX OF LAID TO LAWN AND STONE PAVED PATIO EPC: D Woolstanwood 01270 445678 6 Sundale Drive, Cheshire, CW2 8UB [email protected] How do you like your eggs in the morning? Sunnyside up? as well as a useful W/C off. To the first floor there are three We're excited to offer FOR SALE with the added benefit of NO double bedrooms, the largest of which boasts a range of fitted ONWARD CHAIN, this wonderful family home on Sundale wardrobes. The first floor is completed by the family bathroom Drive! A truly fantastic opportunity to acquire a spacious offers a four piece suite comprising; corner bath suite, walk in property that boasts versatile living space with ample upper shower cubicle, wash hand basin inset vanity unit and a low floor accommodation throughout. Situated in Wolstanwood, the flush W/C. -
The Boundary Committee for England Further Electoral
SHEET 2, MAP 2 Crewe and Nantwich Borough. Ward boundaries in the town of Crewe 4 0 7 3 0 5 5 A B NE CL Bradfield S LA WARMINGHAM CP AY LANE h MOS nc Green ra B ch R MINSHULL VERNON CP i i w v le e d r d i W l M a e Pond n a CHURCH MINSHULL CP a v Cholmondeston Hall C e on r ni U ire sh op B hr 5 S 0 CHOLMONDESTON CP 76 D A O R M A H G IN F M o R w A l W e B W K r E o I N N F Pond o L k S O T F W ' S O E THE BOUNDARY COMMITTEE FOR ENGLAND R L R S A D L N A E R N E N O E A A L D S S FURTHER ELECTORAL REVIEW OF CREWE AND NANTWICH O M A L Final Recommendations for Ward Boundaries in the Borough of Crewe and Nantwich June 2007 LEIGHTON URBAN S ' Leighton Hospital NE B N LA O THY 5 PARISH WARD I R SM 0 7 Sheet 2 of 4 D h 6 nc L ra A h B PARKER'S ic ROAD W lew idd Mablins Lane G l M R R a Community ON D O an INGT C BEX B on Primary School Y ni R U B O e LEIGHTON CP R hir A s W O op ARE D r H U Sh AM G DRI LEIGHTON WARD VE H LEIGHTON RURAL T O M N D A C A PARISH WARD R O B R R O Y KEY E L RIV O E D I L Marina H A N E LEIG M N M D R S O FA E ST DISTRICT BOUNDARY Scale : 1cm = 0.10000 km R L A D N R PROPOSED WARD BOUNDARY R E I D V Grid interval 1km E L M E PARISH BOUNDARY E R R L T MAW GREEN WARD IN W S PARISH BOUNDARY COINCIDENT WITH WARD BOUNDARY A E BRADFIE Y K PARISH WARD BOUNDARY LD ROAD M I PARISH WARD BOUNDARY COINCIDENT WITH WARD BOUNDARY N MAW LANE S H C U RIGB L Y A I L VE F NUE S N ST MICHAEL'S WARD L PROPOSED WARD NAME F O MINSHULL WARD A R Monks E T N N H S S E E R D T Coppenhall E V R WISTASTON CP W F E I O PARISH NAME D E W R L -
Nantwich and Wybunbury, 1680-1819: a Demographic Study of Two Cheshire Parishes
NANTWICH AND WYBUNBURY, 1680-1819: A DEMOGRAPHIC STUDY OF TWO CHESHIRE PARISHES Grace M. Wyatt This study uses the parish registers of Nantwich and Wybunbury with their bare record of baptisms, marriages, and burials, to bring to life the families who lived there in the eighteenth century by examining such topics as years of excess mortality, infant mortality, adult mortality, age at marriage, and size of family. Nantwich and Wybunbury are adjacent parishes in south Cheshire. Cheshire parishes are mostly large and consist of several townships. Nantwich, with five, was much smaller in area than Wybunbury, which had eighteen townships. How ever, Nantwich itself has been a market town for several hundred years. Its other townships, Woolstanwood, Leighton, Alvaston, and Willaston (partly in the parish), are mainly agricultural. Nantwich has been claimed as a gentry town in the late seventeenth century.' In 1674 Nantwich parish had thirty-two large houses with six or more hearths, accounting for about 7| per cent of all taxed hearths, but most of the houses had only one or two. In addition, there were 128 households discharged from paying the hearth tax because of poverty.2 These figures differ from Hodson's but he is perhaps right about domination by the gentry. Nantwich does not compare with York, where 15 per cent of taxed hearths were in houses with six or more. 3 Salt manufacturing at Nantwich was in decline in the late 2 G.M. Wvatt seventeenth century as the loss of nearby wood supplies and the change from wood to coal shifted the centre of the industry to Northwich and Middlewich, which were linked to the Lancashire coalfields by the improvement of the Weaver Navigation.4 The discovery of rock salt at Marbury near Northwich in 1670 and brine springs at Winsford accelerated Nantwich's decline.