A Case Study of Jorhat and Dhubri Districts
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Grower-Details-Report-KARBI ANGLONG
Sl No Grower Name Garden Name Identification No Field office State District Sub Division Possesion Area(in Ha) Tea Area(in Ha) Community Gender 1 ABHIJIT LASKAR APICAS T.G ASKABOAP7155 JORHAT ASSAM KARBI ANGLONG BOKAJAN 3.07 3.07 ST Male 2 ABHIRAM MUNDA PUSHPA MUNDA T.E ASKABAPU1097 JORHAT ASSAM KARBI ANGLONG BARPATHAR 1.85 1.85 OBC Male 3 ABINAS DEY SUJYATA T.P ASKABOSU7194 JORHAT ASSAM KARBI ANGLONG BOKAJAN 0.13 0.13 SC Male 4 AITY TERANGPI SERMILIN T.P ASKABOSE7129 JORHAT ASSAM KARBI ANGLONG BOKAJAN 1.20 1.20 ST Female 5 AJIT KINDO KINDO MTG ASKABOKI1392 JORHAT ASSAM KARBI ANGLONG BOKAJAN 0.26 0.26 OBC Male 6 AJIT KUMAR DEY JOY GURU T.P ASKABOJO7171 JORHAT ASSAM KARBI ANGLONG BOKAJAN 0.67 0.67 ST Male 7 AJOY SINGH BASNU TEA PLANTATION ASKABOBA884 JORHAT ASSAM KARBI ANGLONG BOKAJAN 1.61 1.33 OBC Male 8 AJOY TERANG TERANG TP ASKABOTE1583 JORHAT ASSAM KARBI ANGLONG BOKAJAN 2.60 2.60 ST Male 9 AJUT TERANG MALONGPO T.P ASKABOMA7150 JORHAT ASSAM KARBI ANGLONG BOKAJAN 1.33 1.33 ST Male 10 ALBERT RONGHANG ALBERT TEA GARDEN ASKABOAL1082 JORHAT ASSAM KARBI ANGLONG BOKAJAN 3.33 3.33 ST Male 11 AMAL BORAH AMAL TEA GARDEN ASKABOAM920 JORHAT ASSAM KARBI ANGLONG BOKAJAN 5.00 5.00 OBC Male 12 AMAR SING ENGTI LANGKIRANG MTP ASKABOLA1567 JORHAT ASSAM KARBI ANGLONG BOKAJAN 2.00 2.00 ST Male 13 AMIT LIMBU AMIT TEA PLANTATION ASKABOAM1062 JORHAT ASSAM KARBI ANGLONG BARPATHAR 1.33 0.67 OBC Male 14 AMIT RONGHANG AMIT TP ASKABOAM3489 JORHAT ASSAM KARBI ANGLONG BOKAJAN 2.00 2.00 ST Male 15 AMOS PHANGCHO AMOS TEA ESTATE ASKABAAM1139 JORHAT ASSAM KARBI ANGLONG -

State: Assam Agriculture Contingency Plan for District: Jorhat
State: Assam Agriculture Contingency Plan for District: Jorhat 1.0 District Agriculture profile 1.1 Agro-Climatic/Ecological Zone Agro Ecological Sub Region (ICAR) Assam And Bengal Plain, Hot Subhumid To Humid (Inclusion Of Perhumid) Eco-Region. (15.4) Agro-Climatic Zone (Planning Commission) Eastern Himalayan Region (II) Agro Climatic Zone (NARP) Upper Brahmaputra Valley Zone (AS-2) List all the districts or part thereof falling under the Jorhat, Sivsagar, Golaghat, Tinsukia, Dibrugarh NARP Zone Geographic coordinates of district headquarters Latitude Longitude Altitude 20°10’ N – 27°20’ N 93°37’ E – 93°57’ E 80 – 200 msl Name and address of the concerned ZRS/ ZARS/ RARS/ RRS/ RRTTS RARS, Titabar Mention the KVK located in the district KVK, Jorhat, Kaliapani 1.2 Rainfall Normal Normal Rainy days Normal Onset Normal Cessation RF(mm) (number) SW monsoon (June -Sep): 2100 119 June 2 nd week 4th week of September NE Monsoon(Oct-Dec): - - Oct 2 nd week 3rd week of December Winter (Jan- March) 15 7 Summer (Apr -May) 149 15 Annual 2262 141 1 1.3 Land use Geographical Cultivable Fo rest Land under Permanent Cultivable Land Barren and Current Other Land put or pattern of area area (‘000 area non- Pastures wasteland under uncultivable Fallows fallows non the (‘000 ha) ha) (‘000 agricultural (‘000 ha) (‘000 ha) Misc. land (‘000 (‘000 ha) (‘000 agricultural district ha) use tree ha) ha) use (latest (‘000 ha) crops statistics) and groves (‘000 ha) Area 368.8 152.90 28.54 71.7 4.4 41.57 6.7 27.8 34.87 - - (‘000 ha) 1. -

Waste Management Scenario in Jorhat, Assam Aditya Bhuyan* College of Architecture, Jorhat, Assam, India
l o rna f Wa ou s OPEN ACCESS Freely available online J te l a R n e o s i o t u a International Journal of r n c r e e t s n I ISSN: 2252-5211 Waste Resources Research Article Waste Management Scenario in Jorhat, Assam Aditya Bhuyan* College of Architecture, Jorhat, Assam, India ABSTRACT Solid waste management is a major challenge at local, regional and global level. Jorhat, a major urban agglomeration in Assam, India, produces approx. 35 Tons per day (TPD) of municipal waste which is expected to increase up to 39 TPD and 58 TPD by 2025 and 2035 respectively. With such increased future waste production projection, without any focus on waste management, the city will face acute problems leading to health and sanitary issues. There is a single open disposal site in Jorhat without any facility for recycling or infrastructure for a scientific sanitary landfill at the site. Since 2019, the waste collection facility has improved significantly with daily collection of household from majority of wards across the city. However, the question remains regarding the management of the wastes produced. So, a comprehensive plan for solid waste management as well as its execution should start at the earliest hour with focus on transitioning the economy from linear to circular one thus closing the material loop. Keywords: Municipal waste; Waste management; Circularity; Jorhat city INTRODUCTION 58TPD by 2025 and 2035 respectively [2]. So, a comprehensive plan for solid waste management as well as its execution should With an increase in urban population in the tier II and tier III start at the earliest hour. -

Inland Water Transport Terminal, Dhubri
Inland Water Transport Terminal, Dhubri Name of Project Inland Water Transport Terminal, Dhubri Project Location Dhubri Approx. Project cost INR 277 crores (~ USD 42.62 million) Focus sector Inland Water Transport on NW 2 & NW 16 Status of approvals Pre-feasibility study for the proposed project to be implemented on PPP mode has already been completed. Connectivity The district of Dhubri is well connected by NH31 which is one of the main arteries of National Highways in the state of Assam connecting all the districts in lower Assam. NH31 also connects Dhubri to West Bengal and is also connected to NH52 and NH37, thereby connecting Dhubri to the districts in central and upper Assam on both sides of the river Brahmaputra. The town of Dhubri is connected to NH31 by the State Highway SH28. A new National Highway has been proposed which will connect Dhubri to NH31C directly, which in turn will connect it to West Bengal. The District of Dhubri is well connected by Rail. The Dhubri Railway station is connected to the Fakiragram Junction, where the line coming from Dhubri intersects with the line coming from Bengal to Assam – which connects mainland India with Guwahati and further to Dibrugarh. Dhubri is again well connected to the hinterland of Kokrajhar, and also to Cooch Behar and New Jalpaiguri with rail. At present there is no airport in Dhubri as well as in the border sharing districts. The nearest airport is the Lokpriya Gopinath International Airport at Guwahati which is ~ 238 km away Project contours The proposed project involves construction and upgrade of quays and trestle, bank shore protection, creation of terminal infrastructure, cargo handling infrastructure etc. -

List of Candidates for Interview for the Post of District Programme Manager Under NHM, Assam Sl Regd
List of candidates for interview for the post of District Programme Manager under NHM, Assam Sl Regd. ID Candidate Name Father Name Address No. C/o-GURUPADA CHAKRABORTY, H.No.-59, Vill/Town-DAS NHM/DPM/ ABHIJIT ADHIR KUMAR 1 COLONY PANCHAYET ROAD, P.O.-SILCHAR, P.S.-SILCHAR, 0343 BHATTACHARJEE BHATTACHARJEE Dist.-Cachar, State-ASSAM, Pin-788005 C/o-Dr.(Mrs)T. Borah, SDM&HO Bokajan BPHC, H.No.-H.No.6, NHM/DPM/ 2 AMARJIT TISSO Lt. Mojasing Tisso Vill/Town-Bokajan, Medical Coloney, P.O.-Bokajan, P.S.-Bokajan, 0262 Dist.-Karbi Anglong, State-ASSAM, Pin-782490 C/o-anurag sharma, H.No.-15-01-131,bhawana enclave nowroji road r.k NHM/DPM/ 3 Anurag sharma MR RB Sharma beach, Vill/Town-Visakhapatnam, P.O.-Visakhapatnam, P.S.- 0036 Visakhapatnam, Dist.-Outside State, State-andhdra pradesh, Pin-530002 MR. GHANA C/o-Mr. Ghana kanata Handique, H.No.-T/House No-74, Vill/Town- NHM/DPM/ 4 ARUP HANDIQUE KANTA Merelipathar Village, P.O.-Chabua, P.S.-Chabua, Dist.-Dibrugarh, State- 0136 HANDIQUE Assam, Pin-786184 C/o-ABDUR RAHMAN AHMED, H.No.-OPP VETERINARY NHM/DPM/ AZIZUR RAHMAN ABDUR RAHMAN 5 HOSPITAL, Vill/Town-MATIABAG, P.O.-GAURIPUR, P.S.- 0007 AHMED AHMED GAURIPUR, Dist.-Dhubri, State-ASSAM, Pin-783331 C/o-Mr. Biren Dutta, H.No.-12, Vill/Town-Santipur (Near Law NHM/DPM/ 6 Bikash Ranjan Dutta Mr. Biren Dutta College), Ward No.:-7, P.O.-Bidyapur (Nalbari), P.S.-Nalbari, Dist.- 0138 Nalbari, State-Assam, Pin-781335 NHM/DPM/ C/o-Simon Subba, H.No.-150, Vill/Town-NK Darranga, P.O.-Darranga 7 Deepak Subba Simon Subba 0251 Mela, P.S.-Tamulpur, Dist.-Baksa, State-assam, Pin-781360 C/o-BHABEN CH DAS, H.No.-71, Vill/Town-BELTOLA, TRIPURA NHM/DPM/ DHRUBAJYOTI ROAD, 3RD NO UDAYAN PATH, OPP- AUROGRACE, P.O.- 8 BHABEN CH DAS 0005 DAS BELTOLA, P.S.-BASISTHA, Dist.-Kamrup Metro, State-ASSAM, Pin- 781028 C/o-BHABESH DAS, H.No.-RAJDHANI APARTMENT, FLAT NO. -
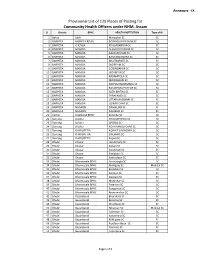
Provisional List of 129 Places of Posting for Community Health
Annexure - IX Provisional List of 129 Places of Posting for Community Health Officers under NHM, Assam Sl District BPHC HEALTH INSTITUTION Type of HI 1 Baksa Jalah Maryajhar SC SC 2 BARPETA BARPETA ROAD BOGRIGURI PATHAR SC SC 3 BARPETA CHENGA KHOLABANDHA SC SC 4 BARPETA MANDIA ALIGAON PATHAR SC SC 5 BARPETA MANDIA BALIKURI PAM SC SC 6 BARPETA MANDIA BAMUNDONGRA SC SC 7 BARPETA MANDIA BHATNAPAITI SC SC 8 BARPETA MANDIA DIGIRPAM SC SC 9 BARPETA MANDIA GOBINDAPUR SC SC 10 BARPETA MANDIA JADABPUR SC SC 11 BARPETA MANDIA KADAMTOLA SC SC 12 BARPETA MANDIA MOWAMARI SC SC 13 BARPETA MANDIA PACHIM BAGHMARA SC SC 14 BARPETA MANDIA RAMAPARA PATHAR SC SC 15 BARPETA MANDIA SATH BHITHA SC SC 16 BARPETA MANDIA TARAKANDI SC SC 17 BARPETA MANDIA UTTAR MAINBARI SC SC 18 BARPETA MANDIA UZIRAR CHAR SC SC 19 BARPETA NAGAON DAMALJAR SC SC 20 BARPETA NAGAON KAHIBARI SC SC 21 Cachar Udarbond BPHC Koomba SC SC 22 Darrang JALJALI CHAULKHOWA SC SC 23 Darrang JALJALI APORIA SC SC 24 Darrang JALJALI NO.4 NANGLI CHAR SC SC 25 Darrang KHARUPETIA NON KE GADHOWA SC SC 26 Darrang KHARUPETIA SIALMARI SC SC 27 Darrang KHARUPETIA Kopati SC SC 28 Dhubri Chapar Hordemara SC SC 29 Dhubri Chapar Kaljani SC SC 30 Dhubri Chapar Noonmati SC SC 31 Dhubri Chapar Simlabari SC SC 32 Dhubri Chapar Sontoshpur SC SC 33 Dhubri Dharmasala BPHC Aironjongla SC SC 34 Dhubri Dharmasala BPHC Alomganj SC Medical SC 35 Dhubri Dharmasala BPHC Boraibari SC SC 36 Dhubri Dharmasala BPHC Falimari SC SC 37 Dhubri Dharmasala BPHC Gaspara SC SC 38 Dhubri Dharmasala BPHC Motirchar SC SC 39 Dhubri Dharmasala -

Yearly Departmental Examination for Taxation Officers Centre …Jorhat
HALF- YEARLY DEPARTMENTAL EXAMINATION FOR TAXATION OFFICERS CENTRE …JORHAT General & Other Book-Keeping Sales Tax Accounts & Markantile Taxation & General Sl. Name of Officers and Present Tribal Laws Office Roll No. Assamese Bengali Hindi Law Laws Commercial Remarks No. Address Language Without Procedure Without Without Knowledge books With Books books Books with books 1 2 3 4 5 6 7 8 9 10 11 12 13 Pankaj Hazarika, 1 335 A Bodo A A A A A A Supdt. Of Taxes®, Sivasagar Rhituraj Neog, 2 Supdt. Of Taxes,Sivasagar Zone, 336 A Bodo A A A A A A Sivasaga Wahida Begum 3 Supdt. Of Taxes,Sivasagar Zone, 337 A Bodo A A A A A A Sivasaga Anamika Borah 4 Supdt. Of Taxes,Tinisukia Zone, 338 A Bodo A A A A A A Tinsukia Sujata Deka 5 Supdt. Of taxes, Tinisukia Zone, 339 A Bodo A A A A A A tinsukia NIHARIKA DUTTA, Supdt. of 6 Taxes, 340 A Bodo A A A A A A Hailakandi Page 2 General & Other Book-Keeping Sales Tax Accounts & Markantile Taxation & General Sl. Name of Officers and Present Tribal Laws Office Roll No. Assamese Bengali Hindi Law Laws Commercial Remarks No. Address Language Without Procedure Without Without Knowledge books With Books books Books with books 1 2 3 4 5 6 7 8 9 10 11 12 13 Kaveri Hazarika, 7 341 A A A A A A A Insp. Of Taxes, Tinsukia Unit Pankaj Sonowal, 8 342 A Insp. Of Taxes, Tinsukia Unit Vinod Kumar Prasad, 9 343 A Bodo A A A A A A Insp. -
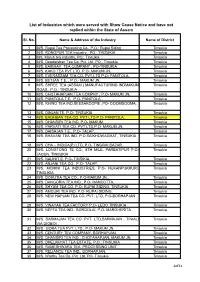
List of Industries Which Were Served with Show Cause Notice and Have Not Replied Within the State of Assam
List of Industries which were served with Show Cause Notice and have not replied within the State of Assam Sl. No. Name & Address of the Industry Name of District 1 M/S. Rupai Tea Processing Co., P.O.: Rupai Siding Tinsukia 2 M/S. RONGPUR TEA Industry., PO.: TINSUKIA Tinsukia 3 M/s. Maruti tea industry, PO.: Tinsukia Tinsukia 4 M/S. Deodarshan Tea Co. Pvt. Ltd ,PO.: Tinsukia Tinsukia 5 M/S. BAIBHAV TEA COMPANY , PO-TINSUKIA Tinsukia 6 M/S. KAKO TEA PVT LTD. P.O- MAKUM JN, Tinsukia 7 M/S. EVERASSAM TEA CO. PVT.LTD P.O- PANITOLA, Tinsukia 8 M/S. BETJAN T.E. , P.O.- MAKUM JN, Tinsukia 9 M/S. SHREE TEA (ASSAM ) MANUFACTURING INDMAKUM Tinsukia ROAD., P.O.: TINSUKIA 10 M/S. CHOTAHAPJAN TEA COMPNY , P.O- MAKUM JN, Tinsukia 11 M/S. PANITOLA T.E. ,P.O- PANITOLA , Tinsukia 12 M/S. RHINO TEA IND.BEESAKOOPIE ,PO- DOOMDOOMA, Tinsukia 13 M/S. DINJAN TE, P.O- TINSUKIA Tinsukia 14 M/S. BAGHBAN TEA CO. PVT LTD P.O- PANITOLA, Tinsukia 15 M/S. DHANSIRI TEA IND. P.O- MAKUM, Tinsukia 16 M/S. PARVATI TEA CO. PVT LTD,P.O- MAKUM JN, Tinsukia 17 M/S. DAISAJAN T.E., P.O- TALAP, Tinsukia 18 M/S. BHAVANI TEA IND. P.O.SAIKHOWAGHAT, TINSUKIA Tinsukia 19 M/S. CHA – INDICA(P) LTD, P.O- TINGRAI BAZAR, Tinsukia 20 M/S. LONGTONG TE CO., 8TH MILE, PARBATIPUR P.O- Tinsukia JAGUN, TINSUKIA 21 M/S. NALINIT.E. P.O- TINSIKIA, Tinsukia 22 M/S. -

E4182 V1: Draft Final Report Vol. I
Public Disclosure Authorized Consultancy Services for Undertaking Environmental Assessment for the Rural Water Supply & Sanitation Project in Assam Public Disclosure Authorized March 2013 DRAFT FINAL REPORT VOLUME I Public Disclosure Authorized Submitted To: Chief Engineer (PHE), Assam. World Bank Project, Hengrabari,Guwahati-781036 Submitted By: IPE Global Pvt. Ltd. Public Disclosure Authorized (Formerly Infrastructure Professionals Enterprise (P) Ltd.) Address: IPE Towers, B-84, Defence Colony, Bhisham Pitamah Marg, New Delhi – 110024, India Tel: +91-11-40755920, 40755923; Fax: +91-11-24339534 Consultancy Services for Undertaking Environmental Assessment for the Rural Water Supply & Sanitation Project in Assam Draft Final Report Table of Contents Abbreviations and Acronyms ...............................................................................................................9 Executive Summary .......................................................................................................................... 11 1. INTRODUCTION ......................................................................................................................... 21 1.1 Background ....................................................................................................................... 21 1.2 Present World Bank Assisted Rural Water Supply and Sanitation Project............................... 23 1.2.1 Components............................................................................................................... 23 -

Central Water Commission Central Flood Control Room, New Delhi Special Advisories for Arunachal Pradesh & Assam 11-07-2020 D
Central Water Commission Central Flood Control Room, New Delhi Special Advisories for Arunachal Pradesh & Assam 11-07-2020 Due to continuous rainfall for the past 3-4 days in the catchment areas of river Brahmaputra and its tributaries in Arunachal Pradesh, Assam & Meghalaya and Sub-Himalayan West Bengal as well as in Bhutan portions of the catchment, River Brahmaputra and its tributaries are rising rapidly. State/ River wise flood situation is as under Arunachal Pradesh Due to rainfall of more than 50 cm in last two days (at 8.30 hrs on 11th July 2020) at Passighat, River Siang at Passighat is flowing in Severe Flood Situation. It is likely to remain in Severe Flood Situation for some more time and then stabilise. As the rainfall is likely to reduce from 13th onwards, there will be slow fall in river thereafter. Assam Brahmaputra River Brahmaputra is in Spate all along its course from Dibrugarh to Dhubri. Station wise situation based on 0800 hrs level of today is as under: Dibrugarh (Dibrugarh District): River is rising and is flowing 0.28 m above its Danger Level of 105.70 m and is expected to flow about 0.44 m above it Danger Level by 2100 hrs today. Since extreme rainfall is likely to continue for 1 more day, there may not be immediate fall. River may stabilise very close to its previous HFL of 106.48 m by tomorrow early morning depending upon the intensity and severity of rainfall. Neamatighat (Jorhat District): River is rising and is flowing 2m above its Danger Level of 85.04 m and is expected to cross HFL of 87.37 m probably today late evening and flow at around 87.40 m by 0900 hrs tomorrow. -

Heavy Floods in Assam Have Affected All the 27 Districts of the State
SITUATION REPORT - ASSAM FLOODS NATURE OF HAZARD : FLOODS DATE: 03.08.04 at 9.30 AM Heavy floods in Assam have affected all the 27 districts of the state. These districts are Tinsukia, Dibrugarh, Shivsagar, Jorhat, Golaghat, Nagoan, Morigaon, Kamrup, Kamrup Metro, Darrang, Sonitpur, Dhemaji, Lakhimpur, Nalbari, Berpetta, Bongaigaon, Kokrajhar, Goalpara, Dhubri, Chirang, Karbi Anglong, Karimganj, Hailakhandi, Cachar, Udalguri, North Cachar Hills and Baska. Heavy rainfall over the state and in neighboring uphill states and countries for a sustained period since the last week of June has resulted in the rise of water level in the whole river network – Brahmaputra and it’s tributaries in the state. Large no. of villages got submerged with the overflowing of these rivers.The worst affected districts during the current flood are Barpeta, Cachar, Dhemaji, Dhubari, Goalpara, Kamrup ( rural), Morigaon, Nagaon, Nalbari, Sonitpur, Udalguri. The rise in the water level, breaches along the river & dam embankments, release of water from upper catchment areas (Bhutan), landslides and sudden change of course by rivers, aggravated and deteriorated overall flood situation of the state. The flood has also caused widespread damages to human life, property, standing crops, flood control embankments, tea gardens and other basic infrastructure in the state. Most of the wild life sanctuaries - Kaziranga National Park, National Parks of Manas, Orang and Dibru-Saikhowa, and Wild Life Sanctuaries Burha Chapori, Pobitora, Laokhowa and Bornodi were affected under the grip of the flood. CURRENT SITUATION : Overall flood situation of the state is improving with the receding of the rivers and less rainfall over the state and adjoining areas in the past few days and there has been no fresh damages reported except the increase in the death toll. -

Inland Water Transport in NER By
Presentation on Inland Water Transport in NER By Inland Waterways Authority of India (Ministry of Shipping, Road Transport & Highways) Guwahati, the 9th March 2007 SADIYA Subansiri Hydel project SAIKHOWA Digboi refinery JAMGURI DIBRUGARH BOGIBIL TEJPUR Bongaigon refinery NEAMATI Numaligarh refinery JOGIGHOPA SILGHAT Legend Guwahati refinery DHUBRI Declared waterway (SHISHUMARA) PANDU BANGLADESH River distance B.Border (Dhubri) – Guwahati 260 km BANGLADESH Guwahati - Dibrugarh 508 km Dibrugarh– Sadiya 123 km Total length 891 km 1 North Bank South Bank Subanasiri Noa dihang Burali Burhi dihang Bargang Disang SADIYA Dhansiri Dikhu Puthimari Jhanju SAIKHOWA Pagladiya Dhansiri DIBRUGARH Beki Kopili Manas Kulsi BOGIBIL Aie Krishnai JAMGURI Champamati Jinary Gadadhar TEJPUR SILGHAT R. RA PUT HMA JOGIGHOPA BRA GUWAHATI DHUBRI PANDU H B A N G L A D SHISHUMARA E S Barak Valley Bhanga Badarpur Silchar 2 Objective Freight transportation by IWT to rise from the present level of 0.03 btkm to 5 btkm by 2025 Importance of IWT for NER z IWT offers shorter route compared to Road/rail z IWT operational even during flood season z Best suited for bulk commodities & Project cargo/ODC- z Provides best and low cost connectivity to hinterland z Employment potential enormous (NCAER Study Feb 2006) every km of IWT operation generates about 3000 jobs 1 lakh investment in IWT results in 6.5 manyears while in rail 0.58 and in other modes 0.87 manyears 3 Importance of IWT for NER Therefore, z Development of IWT mode in NER a strategic & economic imperative z Need for an investment & development strategy z Also need for increasing the efficiency of IWT mode.