Annual Report 2016/17
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Kanivacollege.Vic.Edu.Au [email protected] Contacts: Mr
Principal: Mr Ashley Munn Phone: 53 922 494 Fax: 53922429 www.kanivacollege.vic.edu.au [email protected] Contacts: Mr. C Bendall Assistant Principal; Kaniva Junior School P-6: Mrs K. Cole, Senior School 7-12: Mrs J. Tuckwell. Student Wellbeing: Mrs F. McDonald 11th June 2015 College Items for newsletter to be sent by 12 noon Wednesdays to: [email protected] No school tomorrow Report writing day - Pupil free I hope everyone had a great long weekend and a reminder that students have a very short week this week with Friday being a pupil free day. Teachers are currently preparing reports which will go out on the last day of term, so now is a great time for parents to have conversations about what work needs to be completed prior to the end of term. Students can then use Friday to catch up or stay on top of their work. A reminder, that the deadline for students to achieve an “S” for their unit 1 or unit 3 VCE study is this Friday at 4.00pm. Hannah Braisby, Remmi King, Caitlyn Cassar and William Braunstein, participated in the Legacy Junior Public Speaking Competition last Friday. Miss McLennan has told me that all our CALENDAR students “did brilliantly” especially JuneJuneJune in the impromptu 12 PUPIL FREE DAY speech. I would like to 16 Yr 7 Cows Create Careers, Cobden congratulate these Yr 10-12 Boys Hockey students for giving Dimboola this competition a go Primary WWSSA Lightning Premiership and also to Miss Nhill McLennan for her 17 Yr 9 GWM Water Conf. -

Minyip Bushland Reserve
Birds you may see in the reserve Visiting Minyip Bushland Reserve Red Wattlebird Minyip is a town in the Minyip Bushland Reserve is Minyip Noisy Miner Wimmera region of Victoria, open to the public all year, Singing Honeyeater Australia, 320 kilometres with wheelchair access and White-plumed Honeyeater north-west of Melbourne. is gopher friendly. Bushland White-fronted Chat Camping site with facilities Jacky Winter (including power) is Red-capped Robin available at the Minyip Reserve Hooded Robin Minyip Wetlands. Horsham Varied Sittella Stawell WesternArarat Hwy Ballarat Public toilets are at Rufous Whistler Melbourne Magpie-lark the camping site and in the township (at the Grey Fantail roundabout in Main Street). Willie Wagtail Restless Flycatcher Acknowledgements Black-faced Cuckoo-shrike Minyip Bushland Reserve Committee acknowledges the Eastern Rosella White-winged Triller following organisations for their support: White-browed Woodswallow Black-shouldered Kite Masked Woodswallow Brown Goshawk Dusky Woodswallow Brown Falcon Pied Butcherbird Australian Hobby Australian Magpie A Victorian Government Project Nankeen Kestrel Australian Raven Crested Pigeon Little Raven Galah Australian Pipit Long-billed Corella Mistletoebird Eastern Rosella Welcome Swallow Red-rumped Parrot Brown Songlark Blue Bonnet Rufous Songlark This Buloke (Allocasuarina luehmannii) F Pallid Cuckoo woodland is of national significance. Fan-tailed Cuckoo Minyip Lions Club Dunmunkle CWA Buloke woodlands are listed as an Horsfield’s Bronze-Cuckoo Tawny Frogmouth endangered community under the Kelm Trust and Pipkorn Trust Laughing Kookaburra Commonwealth Environment Protection Brown Treecreeper and Biodiversity Conservation Act. The Striated Pardalote Photography: birds: Ian Morgan; plants: Keith Boschen; trees, shrubs, native grasses and other Weebill aerial map: Wimmera Catchment Management Authority native understorey species all contribute Chestnut-rumped Thornbill Yellow-rumped Thornbill to the significance of this woodland site. -

Rupanyup/Minyip Community Bank® Branch Newsletter May 2012
Rupanyup/Minyip Community Bank® Branch Newsletter May 2012 Chairman’s report Manager’s report How time flies, it only seems like yesterday since our last community newsletter. Welcome to the winter edition of our Community Bank® branch newsletter, time to rug up, eat pies As mentioned in our last newsletter the Rupanyup/ and watch the footy! Minyip Finance Group has supported two young adults to attend university this year. Under the guidance It is with great excitement that we are able to of the Community Enterprise Foundation™ we have announce that Sam Carter and Sean Walsh were selected Sam Carter and Sean Walsh as the recipients the deserving recipients for the Rupanyup & of these two scholarships. All of the applicants were of very high Minyip Community Bank® Branch’s scholarships. standard. We wish Sam and Sean and all the students the best with their We would like to thank everyone who sent in an application; I hope chosen university courses. that you are all having a wonderful first year at university. This year we have been able to support both district football clubs There were recently amendments to government regulations (Minyip/Murtoa Football Club and Rupanyup Football Club) as well as for farm management deposits which now allows for Farm being joint sponsors of the Wimmera League with Bendigo Bank and Management Deposit’s to be held at more than one provider, give Dimboola & District Community Bank® Branch. us a call for more information, just another way to support your community. The Board of Rupanyup/Minyip Finance Group is working on its budget for 2012/13. -

Fire Operations Plan
o! WYP - BIRDCAGE FFR BIG DESERT - BROADIES TRACK WYP - E WYP - NETTING NETTING FENCE BD NHILL MURRAYVILLE FENCE EAST NETTING FENCE CENTRAL FIRE BREAK o! Lake Hindmarsh Brim E Angip W d a R r ip ra h Netherby c irc E k B n - a al b e e b a na l ck - ra R ar a W in b o Jeparit w R D d im d b it - Warracknabeal R o Jepar o la - R a in b o w R d Bangerang d R y b E y r e d w h R Borung Hwy t t H i e r a a i N p e s - J l - y l i l il a h h Warracknabeal r N n N u S E wy Nhi H l H l - Y Wag llup ana un e c R or n d t B y Nhill H w y SALISBURY - NHILL - SALISBURY Gerang NHILL SOUTH RD SWAMP Gerung S ta LOCHIEL w e ll - WIMMERA RIVER - W a Rd r a r to a ur c M k - n ld a na b Do e E a l R d D im b oo la - Minyip Ra Dimbooilnabow Rd Little Desert - East Block Northern Break Horsham - Minyip Rd E LITTLE DESERT - EAST LITTLE DESERT - d Wail R BLOCK NORTH BREAK MCABES HUT e e k TRACK IB l LITTLE DESERT LITTLE DESERT - a WAIL - IRONBARK K - LINK TRACK IB MALLEE TRACK IB TRK m a h s r E LITTLE DESERT o - EAGLE SWAMP H TRACK IB E Little LITTLE DESERT - Desert (East) RA MCDONALDS d HIGHWAY IB Little Desert R l l Salt Lake Tk e w Pimpinio a t S - LITTLE DESERT - d l a MCABES HUT TRACK n Jung o LITTLE DESERT - D STANS CAMP Murtoa E TRACK IB Rupanyup era Hwy LITTLE DESERT Wimm - DAHLENBURGS Little Desert - East MILL TRACK IB Block Southern LITTLE DESERT Break Tk LITTLE DESERT - JUNGKUM Marnoo CENTRAL BLOCK TRACK IB SOUTHERN BREAK NURCOUNG - LEARS RD NORTH Horsham E Mitre Horsham - Drung South Rd Lake E d R r w Natimuk - Fra e Lubeck o nces Rd iv r d r -

Chief Executive Officer Candidate Information Pack
WEST WIMMERA HEALTH SERVICE Chief Executive Officer Candidate Information pack Our vision To pursue excellence in health care services by working collaboratively with our peers and embracing innovation and technology. Our values West Wimmera Health Service has core values that are upheld and translated into reality through the words and behaviours of all our staff. These values are the foundation upon which West Wimmera Health Service is built. Strong leadership and Effective management of the management environment We value our organisation and Our service is managed in ways will encourage exceptional which minimise our impact on the * professional skills and promote * natural environment. collaborative teamwork to drive better outcomes for our consumers. Responsive partnerships with our consumers We maintain a productive A safe environment relationship with our communities The safety of our staff, patients * and stakeholders through open and visitors is fundamental to how communication, honest reporting we operate. and a willingness to embrace * constructive suggestions. A culture of continuing improvement The delivery of superior care to our consumers motivates a * cultural of quality improvement in all that we do. 2 Our principles The following key principles underpin all our decisions: PRINCIPLE 1 PRINCIPLE 5 Evidence-based decision making Regional integration by connecting that informs where we should invest, the the range of organisations, systems and priorities we set and how we deliver our service providers that operate within our services. region to deliver seamless health care services to our consumers. PRINCIPLE 2 Quality care underpins everything we PRINCIPLE 6 do. We meet the Australian standards for Healthy ageing for our community quality in health care. -
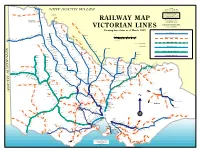
Railway Map Victorian Lines
Yelta Merbein West NOTES Mildura NEW SOUTH WALES All stations are shown with MerbeinIrymple their most recent known names. Redcliffs Abbreviations used Robinvale to Koorakee Morkalla Werrimull Karawinna Yatpool built by VR construction Meringurarrara BG = Broad Gauge (5' 3") Y Pirlta Thurla branch but never handed Benetook over to VR for traffic. Karween Merrinee SG = Standard Gauge (4' 8 1/2") Bambill Carwarp NG = Narrow Gauge (2' 6") Koorakee Boonoonar Benanee RAILWAY MAP Nowingi towards Millewa South Euston All lines shown are or were built by VR construction branch never handed over to VR for traffic, Nowingi Broad Gauge (5' 3") ownership sold to Brunswick Robinvale Plaster Mills 1942 unless otherwise shown. Balranald Bannerton Yangalake No attempt has been made to identify Yungara private railways or tourist lines being Hattah Margooya Impimi Koorkab VICTORIAN LINES run on closed VR lines Annuello Moolpa Kooloonong Trinita Koimbo Perekerten Showing line status as of March 1999 Natya Bolton Kiamal Coonimur Open BG track Kulwin Manangatang Berambong Tiega Piangil Stony Crossing Ouyen MILES Galah Leitpar Moulamein Cocamba Miralie Tueloga Walpeup Nunga 10 5 0 10 20 30 40 Mittyack Dilpurra Linga Underbool Torrita Chinkapook Nyah West Closed or out of use track Boinka Bronzewing Dhuragoon utye 0 5 10 20 30 40 50 60 T Pier Millan Coobool Panitya Chillingollah Pinnaroo Carina Murrayville Cowangie Pira Niemur KILOMETRES Gypsum Woorinen Danyo Nandaly Wetuppa I BG and 1 SG track Swan Hill Jimiringle Tempy Waitchie Wodonga open station Nyarrin Nacurrie Patchewollock Burraboi Speed Gowanford Pental Ninda Ballbank Cudgewa closed station Willa Turriff Ultima Lake Boga Wakool 2 BG and 1 SG track Yarto Sea Lake Tresco Murrabit Gama Deniliquin Boigbeat Mystic Park Yallakool Dattuck Meatian Myall Lascelles Track converted from BG to SG Berriwillock Lake Charm Caldwell Southdown Westby Koondrook Oaklands Burroin Lalbert Hill Plain Woomelang Teal Pt. -

Yarriambiack Shire
MILDURA TEMPY YARRIAMBIACK SHIRE H O S P U E N T R O TOWN AND RURAL DISTRICT A U Y N S I PATCHEWOLLOCK A SEA LAKE NAMES AND BOUNDARIES W A RD L P E U P SPEED PATCHEWOLLOCK TURRIFF WYPERFELD NATIONAL PARK LASCELLES H W Y Y W H SEA LAKE RD N U O T E R P D WOOMELANG O H HOPETOUN SEA LAKE Y RD NT YAAPEET HE S U HOPETOUN N R H A W Y Y SI LAKE A D COORONG R LAKE ALBACUTTA W H O EN B IN T A Y R BULOKE N U O ET P O H ROSEBERY HOPETOUN RAINBOW RD RAINBOW BEULAH BIRCHIP RAINBOW RD BIRCHIP RAINBOW RD W A R R A C K N A B E A L R A I N B O W A IN R RSH H DMA W HIN B Y A N BRIM ILLE Y W W H WILKUR LAH CRYMELON D JEPARIT R WARRACKNABEAL RD G N WATCHEM IP CH R A RD BI WEST LEGEND WARRACKNABEAL R AL E BE A G KN TOWN AND RURAL AC R N MURTOA AUBREY AR DISTRICT BOUNDARY W A BORUNG AREEGRA (defined as localities in the Govt. Gazette) Y B HW H WY HORSHAM LGA BOUNDARY S T CANNUM A W E L L W A R R A C Prepared by Customised Mapping, K N A B OLA E Spatial Information Infrastructure, Ballarat DIMBO A L G N U SHEEP R BO ALLUP W HILLS BOOLITE Version 4.3 D April, 2010 R KELLALAC LAWLER Government Gazette:- R D E 23 July 1998, page 1988 Y E T K N L D 3 June 1999, page 1273 E A R H K 20 November 2003, page 2909 MURRA WARRA OA RT 20 November 2003, page 2910 MU LAEN D 15 April 2010, page 742 M AL A ON H D RS HO RD MINYIP S KEWELL T A W E L L HORSHAM MINYIP RD WARRACKNABEAL A O T R U M D L JUNG A R ON D HORSHAM D WIMMERA HWY RUPANYUP 01530 MURTOA WIMMERA HWY M U STAWELL R T O kilometres A G L E N O R W A NORTHERN C H R LONGERENONG Y R A C K GRAMPIANS N A B E A LUBECK L © The State of Victoria, Department of Sustainability and Environment, 2010 Unless defined or depicted otherwise, where the suburb or rural district boundary follows a R D road, as a general principle the boundary is the centre of the formed road, centre of the This publication may be of assistance to you but the State of Victoria and its employees median where two carriageways exist or centre of the reserve where there is no formation. -
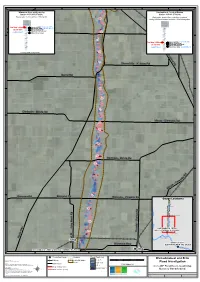
0.5% AEP) Major Flood Level 1 1
1 2 3 4 5 6 7 Wimmera River at Glenorchy Yarriambiack Creek at Mud rtoa R Station 415201B (579001) Station 415241 (579018 ) y g w Rating Htable 18.00 (valid from 07/08/2013) Rating table derived from modellingn completed g 113 a n during the Warracknabeal and Brim Floor d Investigation u e A r A Bo g n a 5m B This Map 5.05m January 2011(38,995 ML/d*) December 2010 (28,001 ML/d) 5m - (0.5% AEP) Major Flood Level 1 1 s Moderate Flood Level 4 l Ailsa Rd l 41,611 ML/d* 4m i Minor Flood Level 4m H 3m p S 3m e 15 ta e 1 h 2m w January 2011S (5,470 ML/d) This Map 2.386me 2m Major Flood Level ll Moderate Flood Level (0.5% AEP) - Minor Flood Level 1m W December 2010 B 6,567 ML/d 1m (2,264 ML/d) B a r r 116 a * Rating table extrapolated c k n a b e a 11 l 7 R Sheep Hills - Kellalac Rd d C Barrat Rd C 119 !. 120 D D 1 21 Dimboola - Minyip Rd Minyip - Dimboola Rd 122 E E 1 23 124 F F 125 Horsham - Minyip Rd 126 d R y b m G o G or - C yip in M 1 28 Banyena Rd Banyena Rd Banyena - Pimpin io Rd Gauge Locations ! Brim H H 129 d R d ! a R o Warracknabeal t h r t r u o M N 130 - g d l n a y u J n w YARRIAMBIACK CREEK o H MURTOA (WIMMERA HIGHWAY) 13 D 1 ! y t .! t I Murtoa I n S e r ! H e Horsham k Jua ng B WIMMERA RIVER Wimmera Hwy GLENORCHY WEIR TAIL GAUGE .!! Glenorchy YARRIAMBIACK CREEK @ MURTOA (WIMMERA HIGHWAY) .! Murtoa 1 2 3 4 5 6 7 .! Streamflow Gauge Cadastre Flood Depth (m) 0 1 2 3 4 5 km Warracknabeal and Brim DATA SOURCES 0 - 0.25 Water Technology, DELWP VIC Railway TUFLOW Model Extent 0.25 - 0.5 Flood Investigation NOTE Major Road Water Technology Pty. -

Download Silo Art Trail Brochure
Silo Art Trail Visitor Map Silo Town Patchewollock — Federation Street 10km N Attraction Petrol Station To Mildura Kernot St Yenolom St Federation St Patchewollock Lake Patchewollock-Sea Lake Rd Patchewollock Tyrrell Sunraysia Hwy Trail Lascelles — Silo Road Sunraysia Hwy Hopetoun-Walpeup Rd Snowdrift Mallee St Sand Dunes Lascelles Kaff-eine & Friends Lascelles Silo Rd Birchip-Sea Lake Rd Boree St Animal Mural Silo Lascelles Hopetoun-Sea Lake Rd The Stockman’s Hut Gallery Wyperfeld Hopetoun Bowling Club Henty Hwy National Park Woomelang Rosebery — Henty Highway Hopetoun Hopetoun-Sea Sirum (vs Venom) Mural Lake Rd Henty Hwy Sunraysia Hwy Yaapteet Hopetoun-Rainbow Rd Rosebery E Rd Rosebery Rosebery Birchip-Rainbow Rd Art Kaff-eine Horse Mural Beulah Henty Hwy About To South Australia To Bendigo Brim — Henty Highway The Silo Art Trail is Australia’s largest outdoor gallery. Brim The trail stretches over 200 kilometres, linking Brim, Swann St Henty Hwy Lascelles, Patchewollock, Rosebery, Rupanyup and Sheep Hills. King St Warracknabeal-Birchip Rd Providing an insight into the true spirit of the Wimmera Mallee, the trail recognises and celebrates the region’s people through a series of large-scale Paine St mural portraits painted onto grain silos, many of Brim which date back to the 1930s. Warracknabeal Borung Hwy Lake The project saw a team of renowned artists from Stawell-Warracknabeal Rd Buloke Australia and across the world visit the region, meet the locals and transform each grain silo into an epic work of art; each one telling a unique story about the host town. Sheep Hills Sheep Hills — Sheep Hills-Minyip Road Donald-Murtoa Rd The Silo Art Trail was conceived in 2016 after the Borung Hwy Sheep Hills - success of the first silo artwork in Brim. -

Balmoral Dimboola Donald Edenhope Goroke Harrow Hopetoun
Wimmera Men’s Sheds Contact List 2019 Barkuma Balmoral Men’s Group Dimboola Donald Edenhope Angling Clubroom, Coleraine Arnott Street Horsham 12 Wimmera Street Dimboola Show Grounds, Hammill Street 49 Elizabeth Street (behind Road, PO Box 20 5381 9336 – Caitlyn Kerr 5397 2137 – Greg McKenzie Donald Council Chambers) Edenhope Balmoral [email protected] [email protected] 0417 587 450 – Ray Walker 5585 1270 – Ron Williams 5570 1304 – Lyn Iredell Open: Thu 10am – 3pm [email protected] Open: Tue, Wed & Thu 10am – [email protected] Access by referral only Open: Daily 3.30pm Open: Thu 1.30 – 5pm Hopetoun Harrow Neighbourhood House, PO Box Horsham Kaniva Goroke 25 Hopetoun Commercial Street Kaniva 17 Swanston Street Harrow 0466 080 633 – Brian Decker 20 O’Callaghans Parade 21 Main Street Goroke 5588 2000 [email protected] Horsham – PO Box 501 0418 822 868 Barry Witmitz 5386 1156/0447 861 156 [email protected] 5083 3408 – Cindy Wooding 0428 358 672 – Geoff Witmitz 5392 2493 Maure Ashfield Rob Stacey Open: Thu Open: Wed 10am – 4pm 0417 016 574 – Chas McDonald 0439 855 350 Charlie Ferrier [email protected] [email protected] [email protected] Open: Mon & Wed 9am – 4pm rg.au Open: Tue 2 – 4pm Minyip Open: Tue & Wed 9.30am – Murtoa 4pm Men’s Matters Group &District Minyip West Wimmera Health Services SLAAM, 36 MacDonald Street Nhill Minyip Murtoa South Street, Minyip 5363 1200 Trudy Tegelhuter 57 Victoria Street Nhill 5385 2785 Jill Elliott Natimuk 0429 857 306 Stephen Kirk [email protected] -

Annual Report 2018 Rupanyup/Minyiprupanyup/Minyip Financefinance Group Limitedgroup Limited
Annual Report 2018 Rupanyup/MinyipRupanyup/Minyip FinanceFinance Group LimitedGroup Limited Rupanyup/Minyip Community Bank® Branch bendigobank.com.au ABN 79 083 123 924 Contents Chairman’s report 2 Manager’s report 3 Minutes of 2017 AGM 4 Celebrating 20 years 6 Bendigo and Adelaide Bank report 8 Directors’ report 9 Auditor’s independence declaration 12 Financial statements 13 Notes to the financial statements 17 Directors’ declaration 27 Independent audit report 28 Auditor disclaimer 30 Income statement 31 Annual Report Rupanyup/Minyip Finance Group Limited 1 Chairman’s report For year ending 30 June 2018 Happy 20th Birthday RMFG. What a wonderful achievement for both our small towns, keeping face to face banking alive. This has proven to be a very successful venture, time and profit has proven many experts wrong. Many thanks for Rob Hunt’s vision, which has resulted in the Community Bank® model. Thank you to all our loyal customers. Be proud of this achievement, without your continued support, 20 years would not have happened. Not only is the bank open in both towns, you have created employment and continued roles for a large number of employees, who enjoy working in our local community. All Bendigo and Adelaide Bank banking services are available at our branches. However, we need to look forward to our next twenty years. With a general decline in rural population, we need to encourage more customers to join us. It’s time to retell the bank’s story. Everyone can help. If there are people who aren’t banking with us, ask them why! The income stream generated from their banking is going into shareholder’s pockets. -

Yarriambiack Facilities Guide
Yarriambiack FPOCKET acilities GUIDE QUICK REFERENCE FOR: ACCOMMODATION | FOOD & DRINKS | AMENITIES | TOWN ATTRACTIONS Yarriambiack Silo Art Trail F acilitiesQUICK REFERENCE FOR: ACCOMMODATION | FOOD & DRINKS | AMENITIES | TOWN ATTRACTIONS LEGEND: INFORMATION CENTRE/ INFORMATION BOARD TOURISM FEATURE ARTWORK FEATURE p CARAVAN PARK m DUMP POINT r CAMPING FACILITIES b FISHING FACILITIES H SKIING PERMITTED F LAKE SWIMMING P HORSE RIDING DINING FACILITIES > COFFEE FACILITIES HOTEL/MOTEL HOTEL POLICE STATION MEDICAL CENTRE ATM SERVICES POST OFFICE BUS V/LINE TRANSPORT BEULAH beulahvictoria.com.au p b F P > Beulah GALAQUIL Monument of 36th parallel | Dingo FenceGalaquil history HOPETOUN hopetounvictoria.com.au p m b H F > ATTRACTIONS INCLUDE: Beulah Weir | Caravan Park 0428 105 930 | First round hospital building | Wall Murals and Bollards | Victoria Hotel 5390 2248 | Beulah IGA 5390 2220 | Beulah Pharmacy Depot 5390 2231 | Beulah Flutterbuys Op Shop Information Centre 5390 2200 BH 0 Located near Hall 9 Service Station – Weekdays / MOGAS 24hrs ATTRACTIONS INCLUDE: Lake Lascelles | Mallee Bush Retreat Accommodation 0439 529 973 | BRIM /Brim Silo Art /Brim Hotel Takeaway food outlets | Corrong Homestead (internal viewing 5083 3240) | Street Mural on shop wall | Hopetoun CommunityHopetoun Hotel 5083 3070 | p r b H F Caravan Park 0417 237 587 | Lakeside House 0408 805 472 | Several B&B Brim Accommodation options | Model Car Raceway 0438 301 566 to arrange an appointment | Bow Bakery 5083 3152 | Wellingtons Butchers | Coffee Shop